
Remember me
Over 100 million Americans suffer from chronic pain, a serious public health issue estimated to cost $261 to 300 billion annually.57 Significant physical, psychological, and socioeconomic effects of chronic pain include sleep disturbance,1 mood disorders,65 and reduced work productivity.28 Although all racial groups experience chronic pain, there are differences in the perception, experience, and impact of pain across groups. African Americans (AAs) experience a greater burden of pain, including more frequent, intense, and debilitating pain severity and functional disability compared with non-Hispanic Whites (NHWs).1,25,35 Differences in socioeconomic status (SES),26 racial discrimination,72 neighborhood disadvantage,53 rates of posttraumatic stress disorder,22 and other mental health conditions4 are commonly cited explanations for these chronic pain disparities, but other potentially relevant factors such as physical activity levels are less explored.
Lower levels of physical activity may be an important driver of pain disparities affecting AAs. African Americans show lower levels of physical activity compared with NHWs46,56,67 and report fewer opportunities to engage in physical activity due to structural factors (eg, fewer safe, walkable neighborhoods, and gyms).53 Physical activity is known to improve a host of chronic pain outcomes including pain severity,5 sleep,29 cellular inflammation,60 and quality of life.20 In addition, physical activity reduces the rates of other adverse health conditions such as hypertension and cardiovascular disease.19 Thus, physical activity may be particularly important in mitigating high-impact chronic pain20,44 and may even protect against chronic pain. Conversely, sedentary behavior may have a pronociceptive effect and increase chronic pain risk.
Previous research suggests that physical activity is associated with antinociceptive mechanisms, whereas sedentary behavior is associated with pronociceptive mechanisms.31 First, the literature on pain processing in athletes demonstrates higher pain tolerance for professional athletes compared with nonathletes.62 Second, prolonged sitting has been associated with higher prevalence of lower back pain in a nationally representative sample of >7000 Korean adults.42 Third, higher physical activity has been associated with reduced chronic pain risk on 2 pain vulnerability markers: temporal summation of pain (TSP) and conditioned pain modulation (CPM).40,41 However, such associations have focused largely on NHWs and have not been systematically explored in AAs. In addition, greater physical activity is not consistently associated with all QST outcomes (less facilitation and more inhibition as reflected in TSP and CPM, respectively), necessitating further examination.31
Temporal summation of pain occurs when a painful stimulus is repeatedly administered at the same intensity, with <3 seconds interstimulus intervals, and perceived pain intensity increases across the stimulus series.15 This pain “summation” is thought to reflect hyperexcitability in spinal nociceptive neurons and captures pain facilitation mechanisms associated with central sensitization, a salient contributor to chronic pain.15,61,69 Conditioned pain modulation is a “pain inhibits pain” task in which pain experienced in response to a test stimulus is reduced through contemporaneous application of a second conditioning stimulus applied distally.32 Greater reduction in pain ratings is thought to reflect more efficient CPM and greater descending inhibition. This type of pain inhibition is mediated through brain to spinal cord circuitry (ie, periaqueductal gray–rostral ventral medulla connections to the spinal cord). Less efficient pain inhibition during a CPM task is associated with the development of chronic postsurgical pain and has been demonstrated in individuals with existing chronic pain conditions.70,71
In sum, previous research has found that decreased pain inhibition and increased pain facilitation play significant roles in conferring chronic pain risk. Physical activity may buffer against chronic pain risk by enhancing antinociceptive processes in the ascending (ie, TSP) and descending (ie, CPM) modulatory pathways. Conversely, sedentary behavior may increase chronic pain risk through pronociceptive mechanisms. Thus, it was hypothesized that greater physical activity and less sedentary behavior would be associated with lower TSP and greater CPM. Finally, to assess whether physical activity and sedentary behavior would be associated with increased overall pain sensitivity, relationships with heat pain threshold and tolerance were also examined.
2. Methods 2.1. ParticipantsThis study used baseline data from a larger ongoing longitudinal study examining the relationship between adversity and pain in healthy AA adults without chronic pain. Exclusion criteria were age (younger than 18 years or older than 45 years due to parent study requirements), chronic pain (ie, reporting clinically significant pain daily/almost daily for past 3 months6), medical conditions affecting the central nervous system (eg, Cushing, hyperthyroidism), medications affecting the pain or stress response, and meeting criteria for substance use disorder within 3 months (assessed through Structured Clinical Interview for DSM-V [SCID]).18
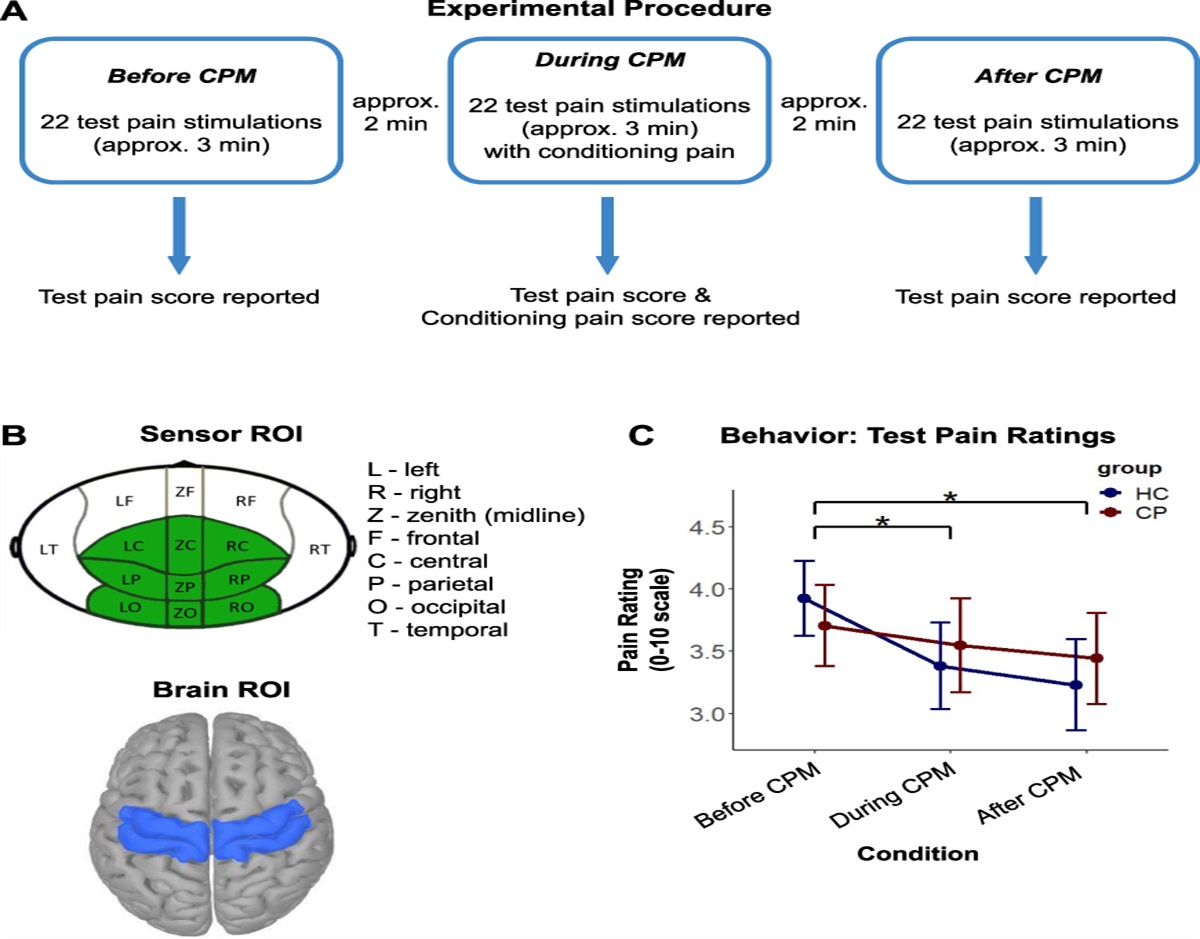
2.2. ProcedureOn arrival at the laboratory, participants provided verbal and written informed consent and the experimenter gave an overview of procedures. Next, exclusion criteria were assessed, the numerical rating scale was explained (NRS: 0 = no pain, 100 = worst pain possible), and participants were instructed on how to rate pain during procedures. The quantitative sensory testing (QST) protocol was identical to one used previously.36,38 Thermal stimuli were delivered through a computerized Medoc TSA-II NeuroSensory Analyzer (Medoc US, Minneapolis, MN) using commercially available software (TPS-CoVAS version 3.19; Medoc Inc, Ramat Yishay, Israel). Order of testing was as follows: heat pain threshold, heat pain tolerance, TSP, and CPM. All tasks were practiced before testing commenced. Questionnaires were administered at the end of the testing session using a research electronic data capture system (REDCap).
Thermode heat stimuli were always applied to the nondominant volar forearm. For assessment of heat pain threshold, participants were instructed to press a button as soon as the heat stimulus first became painful (starting temperature: 32°C, ramp rate: 0.5°C/second). For assessment of heat pain tolerance, participants were instructed to press the button when they could not stand the pain from the heat any longer (starting temperature was 40°C, ramp rate of 0.5°C/second). For both threshold and tolerance, 4 trials were administered and thermode was moved slightly in between trials. For TSP, a sequence of 10 heat pulses with a 48°C target stimulus intensity was delivered. Each pulse was 0.5 seconds in duration and started at a temperature of 40°C, with sequential pulses administered at a frequency of 0.4 Hz. Participants were instructed to rate the NRS pain intensity shortly after the peak of each heat pulse. For CPM, the Pain-60 temperature (P60) for use as the test stimulus was determined first: thermode temperature was set at 45°C and adjusted until a pain rating of 60/100 was achieved.36 Next, the 2 phases of the CPM task were administered. For the test phase, the P60 test stimulus was administered for 3 trials of 30 seconds each (10 seconds ITIs), with NRS ratings obtained after each trial. In the conditioning phase, 3 trials of 30 seconds were again administered, while participants also experienced the conditioning stimulus (submerging dominant hand in a hot 46.5°C water bath; Boekel General Purpose Water Bath, Boekel Scientific, Feasterville, PA).37,39 NRS ratings of test stimulus pain were obtained after each trial.
2.3. Measures 2.3.1. International physical activity questionnaire short formThe international physical activity questionnaire (IPAQ) is a self-report measure capturing the levels of physical activity among adults.10 Three specific types of activity are assessed: walking, moderate-intensity activities, and vigorous-intensity activities. Scoring followed the IPAQ protocol (available online at https://sites.google.com/view/ipaq/score). Responses of less than 10 minutes were set to 0 (applied to 2 participants' data). Then, total physical activity in minutes per week was calculated (walk + moderate + vigorous activity in min total), and activities of greater than 180 were recoded to 180 minutes. The “number of days” variables were examined to ensure no participant had entered a value > 7.
Consistent with the IPAQ scoring manual, groups were formed based on energy requirement defined in METs (ie, metabolic equivalent of a task) multiplied by minutes performed. Specifically, each type of activity (walking, moderate, and vigorous activity) has a MET energy expenditure estimate. Reported time spent in minutes for each activity was multiplied by its MET value, so a total MET-min/week value across activities was estimated to derive physical activity groups representing low, moderate, and high activity levels (according to standard IPAQ scoring instructions). The continuous MET-min/week variable was not used for analyses due to significant positive skew that remained after applying corrective transformations (ie, outlier correction, log transformation).
2.3.2. Sedentary behavior (sitting time)To measure sedentary behavior, participants were asked to estimate their time spent sitting per day. Response options included number of hours and minutes. Sitting time was normally distributed. Therefore, this variable was included as a continuous variable in analyses.
2.3.3. Pain intensity during temporal summation of pain and conditioned pain modulation tasksParticipants rated perceived pain intensity on a numeric rating scale ranging from 0 (no pain) to 100 (worst pain possible).
2.3.4. Control variablesAge, sex, and years of education were assessed using a brief demographic questionnaire. Given established sex differences in pain processing50 as well as known associations between age, sex, education, and chronic pain,11,27 these variables were included as control variables.
2.4. Analysis planAll variables were first examined for non-normality. Outliers were identified using Wilcox MAD–median procedure66 with a threshold of 2.2452 and then winsorized to the nearest neighbor value before analysis (age, years of education, and sitting time were winsorized). The criterion for significance was set at α = 0.05 (2-tailed) for all analyses. Previous literature on physical activity and QST showed associations in the moderate to strong range.21,40,41,54 Using the lowest value for power calculation (f2 = 0.16, based on Ref. 54), a sample of N = 52 would provide a power of 0.80 at 0.05 (2-tailed). Our sample consisted of 129 participants.
2.4.1. Preliminary analysesFirst, the relationship between physical activity and sitting time was examined to determine whether both variables should be included in the same model. A 2 (sex) × 3 (physical activity group) ANCOVA assessing the relationship between physical activity and sitting time was conducted, controlling for age and years of education.
2.4.2. Heat pain threshold and toleranceFor analyses of pain threshold and tolerance, the mean of the last 3 trials was used. For each heat pain threshold and tolerance analysis, a multiple regression was conducted including physical activity, sitting time, age, years of education, and sex. Physical activity was dummy coded before analyses.
2.4.3. Temporal summation of painMultilevel models were conducted in HLM v. 847 to assess the relationship between physical activity (level 2), sitting time (level 2), and within-person changes in pain ratings across the 10 heat pulses (level 1) during TSP. Preliminary analyses showed an initial increase in pain ratings during the train of stimuli which captures sensitization that occurs during TSP, followed by deceleration in pain ratings. Analyses focused on relations between predictors and the linear TSP slope (entered as linear trend). Age, sex, and years of education were entered as control variables for analysis of initial pain ratings (intercept) and TSP slope. The interaction between physical activity and TSP slope across the pulse series was examined as well as the interaction between sitting time and TSP slope. Significant interactions in all analyses were followed up by probing simple effects.45
2.4.4. Conditioned pain modulationMultilevel models were conducted as above to assess the relationship between physical activity (level 2), sitting time (level 2), and within-person changes in pain ratings across the CPM task (level 1). A decrease in pain ratings from the testing phase (P60 alone) to conditioning phase (P60 + hot water bath) was expected if CPM was successfully elicited. As within-person differences across the pulse series during conditioning have been reported previously,37 we focused on predicting the CPM slope (ie, the linear trend). A linear trend was created with baseline value at time point 0 (average rating across 3 preconditioning trials of the test phase) and the 3 conditioning trials as time points 1 to 3 (conditioning phase). The interaction between physical activity and CPM slope was examined as well as the interaction between sitting time and CPM slope.
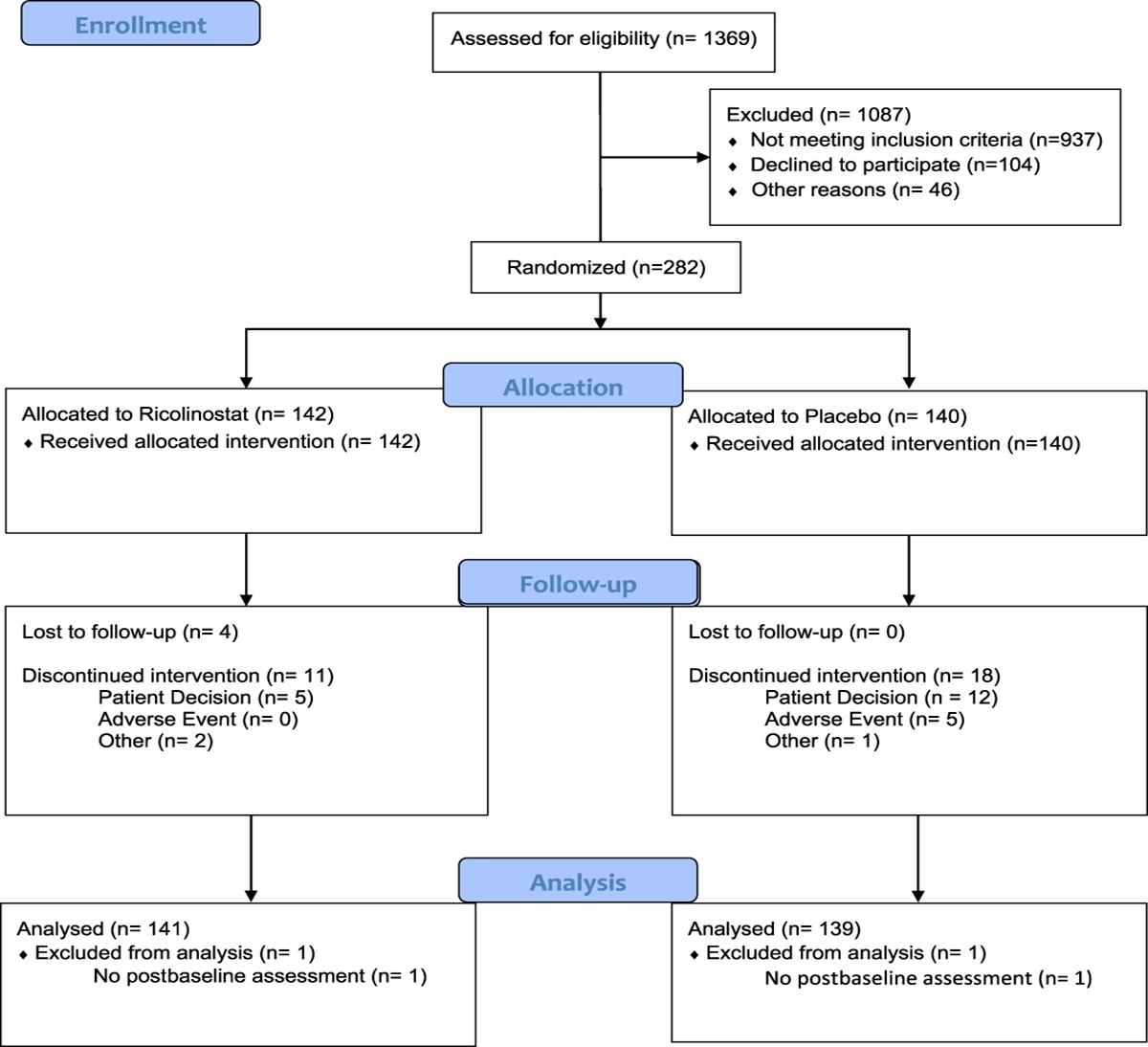
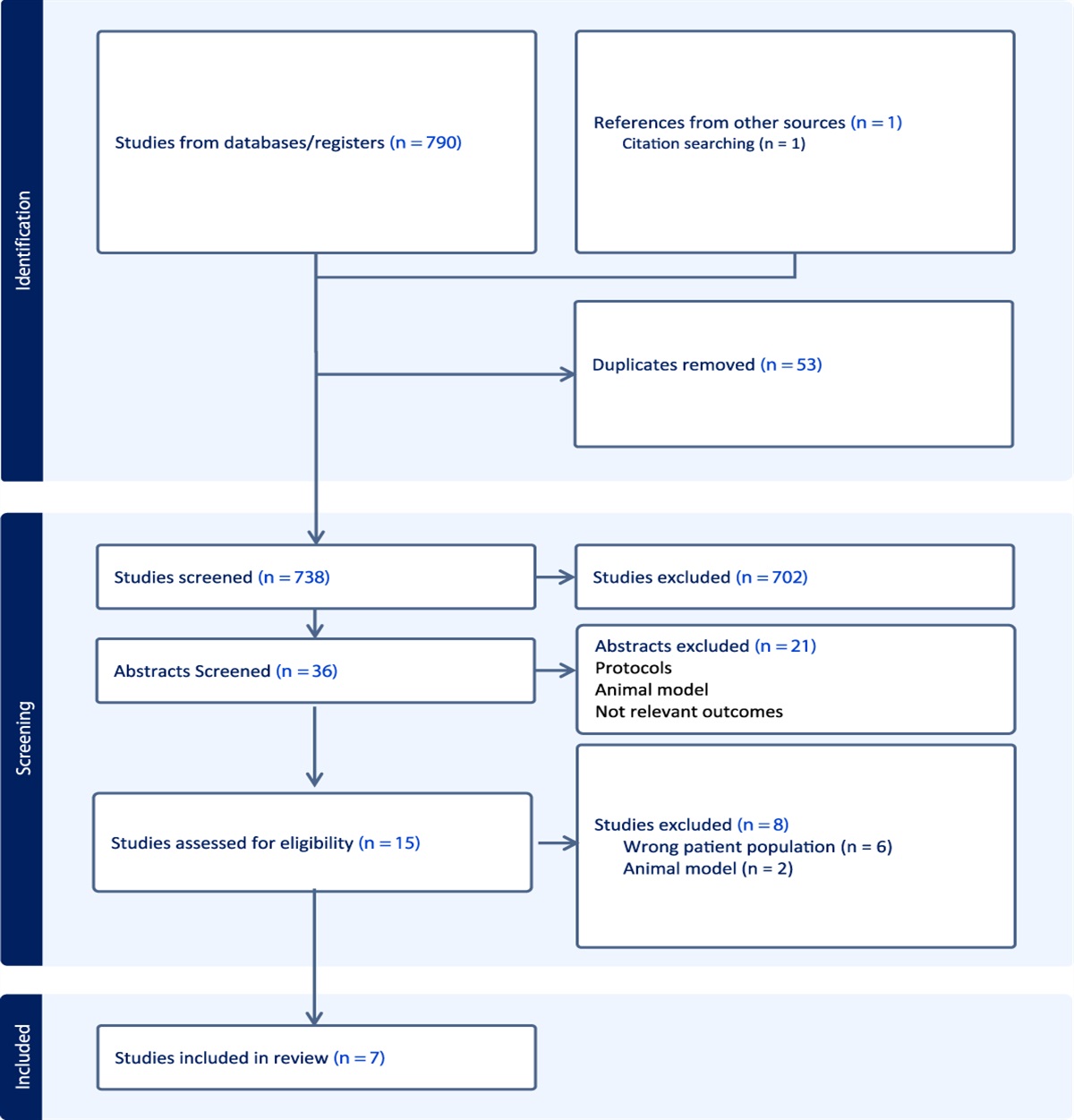
3. Results 3.1. Participants and background characteristicsOf 162 participants enrolled, one was excluded for not meeting age requirements and another was excluded due to chronic pain diagnosis (both revealed after baseline assessment was completed). Three participants did not complete the TSP task (for 2, the maximum pain rating was reached before task completion; 1 participant declined to finish). One participant did not complete the study because of scheduling issues. Twelve participants were excluded because of physical activity scoring issues (ie, entering “I don't know” on key questions). Two participants were excluded due to questionable validity in responding to the “sitting time” question (ie, endorsed 0 time spent sitting). Finally, 13 participants had missing survey data due to experimenter error. This left a total of 129 participants for analysis. In the sample of 129 participants, 79 (61.2%) were female and 50 (31.8%) were male. Table 1 presents mean and standard deviations (SD) for sample demographic characteristics.
Table 1 - Participant demographic characteristics. Characteristics M/n SD/% Age (y) Mean (SD) 25.82 6.27 Range 18–44 Sex Female 79 61.2% Male 50 38.8% Hispanic or Latino Heritage Non-Hispanic/Latinx 127 98.4% Hispanic/Latinx 2 1.6% Marital status Single 110 85.3% Married 13 10.1% Cohabitating 6 4.7% Employment In school 59 45.7% <40 h/wk 24 18.6% > 40 h/wk 38 29.5% Unemployed 3 2.3% Education High school/GED 49 38% Vocational/technical degree 2 1.6% Associate's degree 5 3.9% Bachelor's degree 38 29.5% Graduate degree 35 27.1%Group 1 (low activity) averaged 176.78 total MET-min/week (median = 82.50, interquartile range = 396.00, n = 30), group 2 (moderate activity) averaged 1681.23 total MET-min/week (median = 1732.50, interquartile range = 1150.00, n = 41), and group 3 (high activity) averaged 5558.49 total MET-min/week (median = 4297.50, interquartile range = 3589.40, n = 58). See Figure 1 for distribution of MET-min/week per category.
 Figure 1.:
Figure 1.: Total MET/min per week for each group (dots represent participants). Physical activity groups based on International Physical Activity Questionnaire Short Form scoring. Physical activity group 1 = low level of activity, group 2 = medium level of activity, group 3 = high level of activity; MET, metabolic equivalent of a task.
3.3. Sitting timeOn average, participants estimated spending 440.24 minutes per week sitting (median = 420 minutes, interquartile range = 300). Figure 2 depicts the distribution of sitting time.
 Figure 2.:
Figure 2.: Histogram of weekly time spent sitting in minutes.
3.4. Preliminary analyses (relationship between physical activity and sitting time)The results from the ANCOVA indicated that there were no significant main effects of physical activity (F(2,121) = 1.45, P = 0.24, η2 = 0.023) or sex on sitting time (F(1,121) = 0.02, P = 0.88, η2 <0.001). There was also no significant interaction between sex and physical activity on sitting time (F(2,121) = 2.74, P = 0.07). Given the lack of association between physical activity and sitting time, both were included as predictors in the same model.
3.5. The relationship between physical activity, sitting time, and heat pain threshold and toleranceIn the regression analysis predicting heat pain threshold, the results indicated a nonsignificant model (F(6,122) = 1.30, P = 0.26) that explained 6% of the variance (R2 = 0.06). Neither physical activity, sitting time, nor any of the control variables emerged as significant predictors (medium activity β = 0.04, high activity β = 0.02, sitting time β = 0.06, sex β = −0.09, age β = 0.10, education β = 0.16).
In the regression analysis predicting heat pain tolerance, the results also indicated a nonsignificant model (F(6,122) = 2.04, P = 0.07) that explained 9% of the variance (R2 = 0.09). Sex emerged as the only significant predictor (B = −0.83, SEB = 0.29, β = −0.25, P = 0.005), with male sex being associated with higher heat pain tolerance. Neither physical activity, sitting time, nor any of the control variables emerged as significant predictors (medium activity β = 0 .13, high activity β = 0.04, sitting time β = 0.11, age β = 0.001, education β = 0.07).
3.6. The relationship between physical activity, sitting time, and temporal summation of painTable 2 and Figure 3 present the results of multilevel modeling analysis of TSP. The results revealed a significant TSP slope, indicating a significant TSP effect over time across groups (ie, pain ratings were increasing across pulse series). The interaction between physical activity and TSP slope was significant, indicating that physical activity affected the steepness of the TSP slope. Tests of simple slopes revealed that all groups exhibited TSP; however, groups engaging in greater amounts of physical activity showed reduced TSP slopes (Fig. 3; low activity: slope = 2.36, P < 0.001, medium activity: slope = 2.14, P < 0.001, high activity: slope = 1.91, P < 0.001), which is consistent with an association between greater physical activity and reduced pain facilitation.
Table 2 - Results of multilevel modeling analysis of temporal summation of pain. Estimate CI SE P Fixed effects Pain ratings Intercept 63.539 29.69, 97.39 17.272 <0.001 Sex 1.203 −7.37, 9.77 4.372 0.784 Sitting time −0.024 −0.05, 0.00 0.012 0.048 Age 0.350 −0.42, 1.12 0.392 0.374 Education −1.203 −2.77, 0.36 0.797 0.134 Physical activity group −4.022 −9.37, 1.33 2.731 0.143 TSP slope 2.584 1.48, 3.69 0.562 <0.001 Sex × TSP slope −0.481 −0.74, −0.23 0.130 <0.001 Sitting × TSP slope 0.001 0.001, 0 0.0006 0.126 Age × TSP slope −0.030 −0.05, −0.01 0.012 0.011 Education × TSP slope 0.016 −0.03, 0.06 0.024 0.499 Physical activity group × TSP slope −0.224 −0.38, −0.07 0.081 0.006 Quadratic trend −0.148 −0.20, −0.10 0.025 <0.001Physical activity group based on scoring of the International Physical Activity Questionnaire Short Form; quadratic trend models habituation across pulse series; bolded values are significant.
Confidence Interval: Estimate ± (1.96 × standard error).
CI, confidence interval; Intercept, mean pain rating when predictors are equal to 0, ie, pain rating for first pulse; TSP slope, temporal summation of pain slope.
 Figure 3.:
Figure 3.: Physical activity and temporal summation (TSP) of pain. Each line depicts a simple regression line relating heat pulse number to the dependent variable (pain) at different levels of the physical activity moderator; physical activity groups based on International Physical Activity Questionnaire Short Form scoring; differences in slope indicate differences in summation between groups; the group × pulse interaction indicates that the slopes for these groups were all significantly different from one another; the asterisks are indicating that slopes are all positive and different from 0. *P < 0.001.
The interaction between sex and TSP slope was significant as well, indicating that sex affected the extent of TSP. Tests of simple slopes revealed that while both men and women showed TSP, men showed a steeper slope (ie, greater TSP) than women (men: slope = 2.10, P < 0.001; women: slope = 1.62, P = 0.002). The interaction between age and TSP slope was significant as well: Whereas all age groups showed TSP, greater TSP was observed in younger (slope = 2.76, P < 0.001) as compared with older (slope = 2.41, P < 0.001) participants.
3.7. The relationship between physical activity, sitting time, and conditioned pain modulationTable 3 presents the results of a multilevel model predicting CPM. Contrary to expectation, none of the predictors emerged as significant. Figures 4 and 5 portray the pattern of observed CPM effects. Similar to previous studies,12,13 some individuals exhibited pain inhibition, whereas others exhibited pain facilitation during the CPM protocol. It is thus unlikely that our results are due to unusual CPM responses in our sample.
Table 3 - Results of multilevel modeling analysis of conditioned pain modulation. Estimate CI SE P Fixed effects Pain ratings Intercept 51.630 26.38, 76.88 12.881 <0.001 Sex 0.316 −6.07, 6.70 3.259 0.923 Sitting time 0.005 −0.01, 0.02 0.009 0.564 Age −0.033 −0.61, 0.54 0.293 0.912 Education 0.118 −1.05, 1.28 0.595 0.843 Physical activity group 0.284 −3.70, 4.27 2.035 0.889 CPM slope −1.088 −8.28, 6.11 3.670 0.767 Sex × CPM slope −0.656 −2.47, 1.16 0.928 0.480 Sitting × CPM slope −0.004 −0.01, 0 0.003 0.104 Age × CPM slope 0.013 −0.15, 0.18 0.084 0.876 Education × CPM slope 0.084 −0.25, 0.42 0.171 0.622 Physical activity group × CPM slope −1.027 −2.16, 0.11 0.579 0.077Physical activity group based on scoring of the International Physical Activity Questionnaire Short Form; bolded values are significant.
Confidence Interval Estimate ± (1.96 × standard error).
CI, confidence interval; CPM slope, conditioned pain modulation slope; Intercept, mean pain rating when predictors are equal to 0, ie, average rating across 3 preconditioning trials of phase 1.
 Figure 4.:
Figure 4.: Mean test stimulus pain ratings in the test phase and during presentation of stimuli 1 to 3 during the conditioning phase of the CPM protocol. Each line = 1 participant. The first number is a within-person mean of the test phase ratings (pulse 0); the next 3 are within-person ratings, not means (pulse 1–3). CPM, conditioned pain modulation.
 Figure 5.:
Figure 5.: Histogram depicting the frequency with which individuals inhibited (negative values), facilitated (positive values), or showed no change during conditioned pain modulation (CPM). Values depict average change score = (average of 3 preconditioning trials) − (average of 3 conditioning trials).
4. DiscussionHigher pain facilitation (reflected in TSP) and decreased pain inhibition (reflected in CPM) both significantly contribute to the risk of developing chronic pain.59 Physical activity may lower the likelihood of developing chronic pain by engaging antinociceptive mechanisms in pain modulatory pathways.40,41 Conversely, sedentary behavior may raise the risk of chronic pain through pronociceptive pathways. We aimed to explore the relationship between physical activity/sitting time and degree of pain facilitation and pain inhibition in AAs using dynamic QST measures. In addition, given the general lack of research on (in)activity and pain in AAs, pain sensitivity (as measured with static QST) was also examined. Higher levels of physical activity were associated with reduced TSP in AAs. However, greater physical activity was neither associated with elevated CPM nor reduced static pain sensitivity. In addition, contrary to expectation, self-reported sitting time was not associated with TSP, CPM, or static QST.
4.1. Greater physical activity was associated with reduced temporal summation of painConsistent with prior literature in predominately White samples,40,41 greater physical activity was associated with reduced TSP in this sample of AAs. These findings suggest that being physically active could potentially reduce the risk for chronic pain in AAs, given that greater TSP is predictive of the development of chronic postsurgical pain43 and is frequently found in chronic pain populations.34 Temporal summation of pain is thought to capture mechanisms associated with central sensitization, specifically hyperexcitability of spinal nociceptive neurons.15,49,69 The present findings suggest the possibility that greater physical activity may dampen this spinal hyperexcitability, associated supraspinal signaling, and/or pain perception. Although one can only speculate about potential biological mechanisms that mediate this effect, research on the role of physical activity in aging suggests that physical activity may have anti-inflammatory and antioxidant effects.16,33,40,58,68 Specifically, physical activity is associated with lower levels of inflammatory markers such as C-reactive protein and IL-6, and regular exercise upregulates antioxidant defense systems68 that reduce oxidative stress linked to elevated pain.7 Either of these mechanisms may contribute to the antinociceptive effects of physical activity. Furthermore, TSP is hypothesized to involve N-methyl-d-aspartate (NMDA) receptor activation,3,23 and animal research shows that regular exercise leads to reduced NMDA receptor phosphorylation.31,33 Thus, greater physical activity may lead to reduced NMDA receptor activity, ultimately resulting in reduced TSP. More basic science research is needed to clarify the role of these mechanisms in conveying the antinociceptive effects of physical activity.
4.2. Physical activity was not associated with conditioned pain modulationSurprisingly, physical activity was not associated with CPM, which suggests that physical activity may not improve CPM-associated descending inhibition. This is contrary to previous research which found associations between elevated physical activity and improved pain inhibition.21,40,41,54 Reasons for these discrepant findings are unclear. Our CPM results may reflect altered associations between physical activity and pain inhibition in AAs, but this could only be addressed in studies directly comparing these associations across racial groups. Another potential explanation for these conflicting results relates to the younger age of our sample (mean age of sample = 25.8 years). Given that CPM efficiency is known to decrease with age,24 physical activity may be less relevant as a determinant of CPM in younger individuals because their CPM is already efficient. On a speculative note, physical activity may improve CPM inhibition as we age and protect against pronociceptive age-related effects. Indeed, one study of healthy middle-aged participants found that greater physical activity was linked to reduced TSP and greater CPM (mean age: men = 39.28; women = 45.6441). Finally, the issue of dose-response effects may be relevant. Athletes have been shown to exhibit improved CPM,21 perhaps due to improved opioidergic functioning,48 and our sample may not have been exercising strenuously enough to produce these favorable effects. Prior work does suggest associations between exercise intensity and degree of exercise-related analgesia.5
4.3. Sitting time was not associated with temporal summation of pain or conditioned pain modulationIn this study, sitting time was not associated with TSP or CPM. This may be due to how sitting time was measured. Naugle et al.40 indicated that less sedentary time was associated with better CPM, but sedentary behavior was defined with an accelerometer, not with self-report as in the current work.40 As sedentary behavior is defined as any waking behavior characterized by an energy expenditure of ≤1.5 metabolic equivalents (eg, watching TV, reading63), it is possible that sitting time was not accurately captured by our subjective measure.
Alternatively, it is possible that our sample was not showing enough sedentary behavior to observe deleterious effects on CPM or TSP. Park et al.42 determined that sitting increases chronic pain risk if individuals sit for more than 7 hours. In our sample, the mean sitting time was exactly 7 hours, potentially indicating that time spent sitting was not high enough to affect pain modulation. Overall, more research is needed on validity of self-reported sedentary behavior measures and whether there is a dose-dependent effect of sitting time on pain modulation.
4.4. Heat pain threshold and toleranceNeither our heat pain threshold nor tolerance measures were associated with physical activity or sitting time. Prior research has found mixed results with some studies finding no assoc
Comments (0)