Discussion
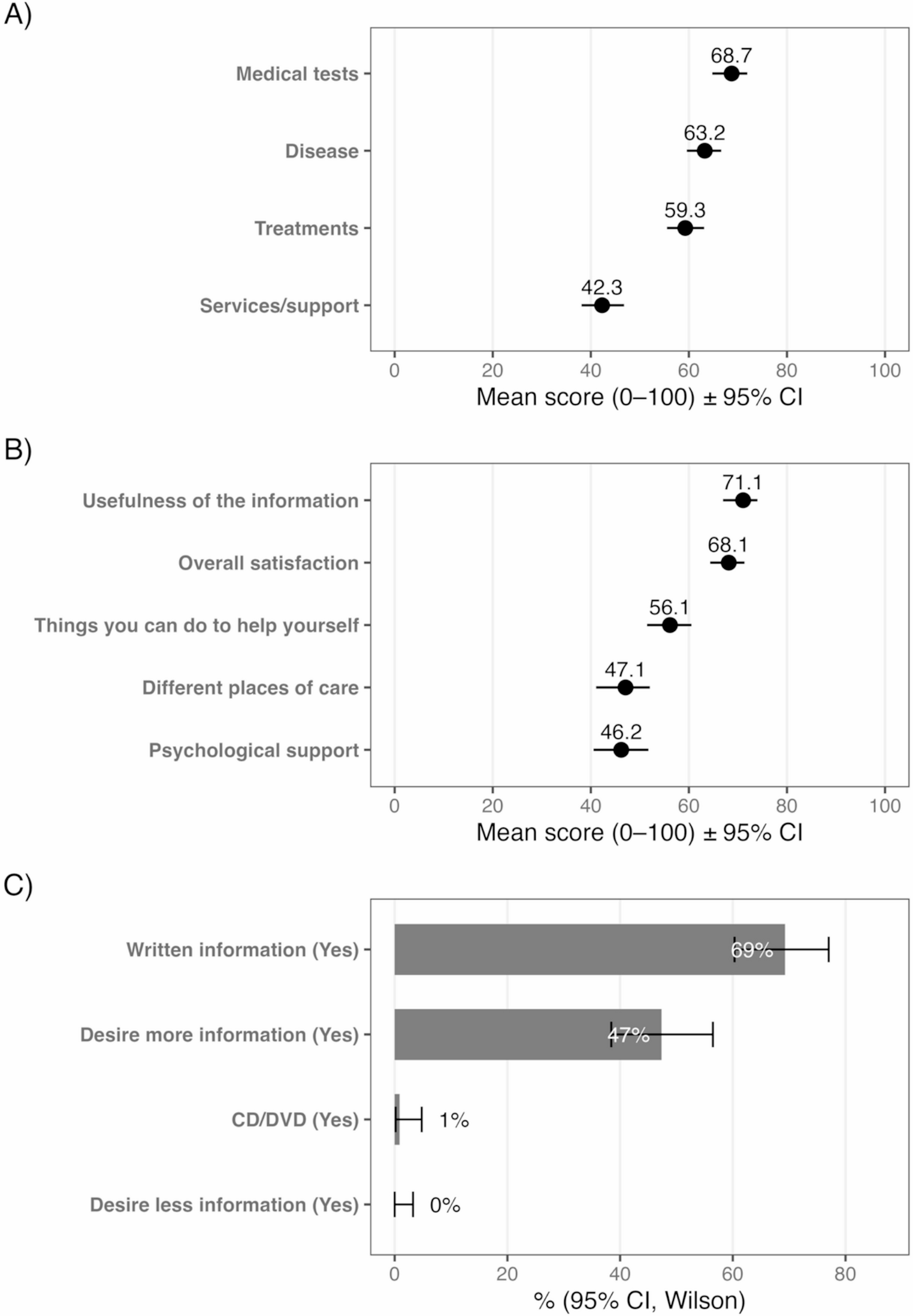
This study included a mixture of long-term survivors and patients undergoing treatment for recurrent disease following resection of CRLM. Patients were, in general, very satisfied with the information provided to them during their treatment and they found it helpful. There were no specific factors that influenced patient satisfaction with the information they received or how helpful it was during treatment. Areas of improvement identified include providing information about other supportive services within the hospital (e.g., the cancer nurse coordinator (CNC)) or outside the hospital (psychological support, occupational therapy, physiotherapy, and acupuncture services) and additional support options from in-home support nurses or other allied health professionals.
In a study from Spain on patient satisfaction with information provision in patients with colorectal cancer (CRC), Rodriguez et al. compared the inpatient and outpatient settings [12]. Overall, patients were happy with the information provided, as was found in the current study. However, the provision of information about such things as supportive services outside the hospital or about the causes of the disease were rated poorly by patients. In a similar study from Sweden, which has a universal healthcare system, Lithner et al. examined patients who underwent resection of CRC using the EORTC QLQ-INFO25 questionnaire, and these patients rated their experience with information provision poorly across all the domains [13]. They received the most information about their medical tests and the disease itself, but the least about other supportive services outside the hospital. Interestingly, these authors found that women and patients with significant comorbidities received the least amount of information. Spain and Sweden both have universal healthcare systems funded primarily by tax revenue. It might be expected that services are less fragmented than in other countries with large components of private healthcare. However, this does not appear to guarantee an adequate level of information provision during cancer care. To date, minimal studies have assessed the impact of the type of healthcare system on the provision of information provided to cancer patients. The findings in the study from Spain and Sweden may simply reflect the clinicians’ understanding or bias about whether information provision is helpful or not [1].
Husson et al. conducted two studies in the Netherlands comparing information provision in different cancer types. The first was in patients with either primary or metastatic CRC (mCRC), and the second was in patients with non-GIT cancers (endometrial, Hodgkin lymphoma, non-Hodgkin lymphoma, and myeloma) [14, 15]. In both studies, they found low average scores similar to the findings of Lithner et al. A consistent theme across all studies is that information provision is the lowest in relation to support services available outside the hospital, including receiving treatment at home.
From the literature published to date, it is evident that irrespective of the healthcare system where the patient is being treated, there seems to be inconsistency in the delivery of information to patients, suggesting room for improvement. One way to improve information provision might be for the treating clinician to provide written information on an ongoing basis so that patients can better understand information explained verbally during consultations. This could be in the form of a regular follow up letter to the patient, similar to what is written by a specialist to the general practitioner (GP) following a consultation.
Whilst numerous online resources are available, surgeons or medical oncologists providing a summary or brochure with specific links and resources for further information as a routine part of their care may give the patient more confidence and the opportunity to absorb the information and ask questions. This information may include the cause of the disease, information about the treatment options, and any self-help advice. Ideally, all specialist consultations should be for an adequate amount of time to allow patients the opportunity to ask questions, especially during follow-up consultations or just prior to commencing treatment, where the discussion is recorded and documented in writing, which may reduce concerns and clarify outstanding issues. There is an opportunity for professional colleges (especially the Royal Australasian College of Surgeons and the Royal Australasian College of Physicians) to consider introducing training and workshops for junior doctors on communication, particularly in cancer care. Currently, there are a few dedicated training or continuing professional development opportunities offered in Australia. There are some communications skills training modules offered by Cancer Australia that might also be mandated to improve the provision of information to patients in the future [16].
The provision of information to patients undergoing any form of treatment for CRLM, including liver resection, is a complex issue that transcends the type of healthcare system. Effective information provision can have a significant impact on patient outcomes and beyond just making the patient treatment pathway easier. High levels of information provision reduce levels of anxiety and stress, improve treatment adherence, increase the sense of patient empowerment during treatment, and improve quality of life [17,18,19].
In this study, information about other services, including rehabilitation and psychological support, were particularly inadequate. It is not clear who should inform patients about these services, at what stage they should be provided, and how patients can best take advantage of them. Undoubtedly, healthcare providers should relay as much information as possible to those in closest contact with the patient, including their GP, family members, or the relevant CNC. A systematic review by Meiklejohn et al. supports a greater role for GPs in care coordination, cancer screening, and the management of the physical and psychological effects of the diagnosis and treatment of cancer [20]. Vogel et al. also studied the role of a GP in cancer care and found that most patients wanted their GP to offer more complementary and alternative medicine options [21].
The limitations of this study include the fact that a survey such as this involves recall bias, particularly in patients diagnosed with CRLM who were treated many years ago, as well as reliance on self-reported measures of information provision. From the data collected, it was not possible to assess if a specific clinician or type of specialist was responsible for either good or bad information provision. Furthermore, the EORTC QLQ-INFO25 assessment tool does not describe when the information was provided to the patient. A future area of work might involve assessing information provision prospectively at different time points, such as at the time of diagnosis, before their primary cancer surgery, before the administration of chemotherapy, and before the liver resection. The cross-sectional nature of the current study provides a snapshot in time, limiting the causal association between the outcomes and the factors of interest. Due to the number of deceased patients and non-responders, the sample size was small. Regardless, this is the first study to assess patient information provision in patients who have undergone liver resection for CRLM.
Conclusion
This study showed that, overall, patients who underwent treatment for CRLM received sufficient information about their medical tests and proposed treatment, were satisfied with the information they received, and found it helpful. However, some patients felt they could have received more information about additional support services. Information provision can improve, and it is likely that this will only be achieved through further education of specialists, GPs, and allied health staff about the value of high-level communication and by ensuring there is appropriate infrastructure support to ensure this happens.



Comments (0)