
Remember me
Worldwide, one in four to five children and adolescents suffers from a mental or behavioural disorder (1–5). With one-third to half of all mental and behavioural disorders starting in adolescence or earlier, childhood and adolescence are particularly vulnerable periods for mental health over the entire lifespan (1, 6–10). Additionally, mental and behavioural disorders are among the leading causes of disability and premature death in childhood and adolescence in industrialised nations (2, 3, 11). Currently, children and adolescents are experiencing multiple global crises and existential threats, such as the climate crisis, the aftermath of the COVID-19 pandemic, and the global effects of terror, war, and displacement. These experiences further strain the physical and mental health of children and adolescents worldwide (12–23).
Untreated mental and behavioural disorders in childhood and adolescence exhibit high rates of chronicity and persistence, along with a significant risk of developing comorbid disorders (1, 6–10). This can lead to long-term impairment in social participation and substantial secondary costs for society. Therefore, early intervention is essential to prevent mental health issues in adulthood and promote well-being and productivity throughout life. Psychotherapy is a central component of guideline-based treatment of mental and behavioural disorders in childhood and adolescence, and its effectiveness is well documented for numerous mental and behavioural disorders in these age groups (24–32). Nevertheless, even in wealthy Western countries with relatively well-developed public healthcare systems, access to professional mental health services often remains inadequate (33–35). To address this issue, the European Commission Reform Support, in cooperation with UNICEF, has recently launched a Flagship project in four EU member states to initiate reforms to expand access to mental healthcare for children and adolescents (36). To generally improve the provision of psychotherapeutic care for children and adolescents systematic and multimodal evaluations of the provision of psychotherapeutic care are needed but often lacking.
This review focusses on data regarding the outpatient psychotherapeutic care in Germany but offers a general discussion of different data sources and aims to provide an example how to evaluate access to psychotherapeutic care. Internationally, the German mental health care system for children and adolescents stands out, as it is largely funded by statutory health insurance (SHI), which covers approximately 90% of the population, including children and adolescents (37). Before accessing SHI-funded healthcare, low-threshold support is available through school-based resources such as counselling teachers, social workers, and psychologists, as well as external counselling services like family counselling centres or anonymous support via phone, chat, or email. School-based psychosocial services focus on prevention, diagnosing learning and school-associated mental disorders, crisis intervention, and referrals to external support and treatment, but they do not treat mental disorders and are highly limited in capacity (38, 39). Paediatricians and general practitioners are often the first point of contact, providing guidance to children, adolescents and their families while referring them to specialised psychotherapeutic or psychiatric care when needed. However, accessing outpatient mental health services does not require a mandatory referral from a physician, as patients can independently seek these services. Accessing specialised outpatient care funded by SHI involves an initial consultation with a psychotherapist or psychiatrist, which is a mandatory step regulated by the “Psychotherapy Guideline” and includes initial diagnostics and treatment recommendations (40). Afterward, patients may proceed to a more comprehensive diagnostic assessment and/or guideline-based outpatient psychotherapy. Guideline-based psychotherapy refers to SHI-funded psychotherapeutic treatment provided by SHI-accredited psychotherapists and psychiatrists, following initial consultations and probationary sessions, and is regulated in the “Psychotherapy Guideline” (40). Although Germany offers the highest number of inpatient beds in psychotherapeutic and psychiatric units in Europe, the number of child and adolescent psychologists/psychotherapists relative to the population seems to be lower compared to other European high-resource countries, and relatively less children and adolescents receive outpatient mental health care (34, 41, 42). One reason for the latter is that children and adolescents with mental disorders are often unable to find care or have to put up with unacceptably long waiting times (43, 44). Since the COVID-19 pandemic, the demand for psychotherapy, especially among children and adolescents, has increased, leading to a further rise in waiting times for psychotherapy. In 2021 and 2022, children and adolescents waited on average around 10 weeks for an initial consultation and around 25 weeks for the start of guideline-based psychotherapy (45–48). Meanwhile, SHI agencies only recorded a small increase in applications for guideline-based psychotherapy of 4–6% during the COVID-19 pandemic (49). This suggests that the supply capacities have already been fully exhausted before the pandemic and therefore, the increase in psychotherapeutic services and applications is only a poor reflection of the increased demand for psychotherapy. It is estimated that in the end only 5–10% of children and adolescents with a confirmed diagnosis of a mental or behavioural disorder receive access to guideline-based psychotherapy (32, 50, 51).
Current demand planning regulations, which determine the capacity and distribution of SHI-funded outpatient healthcare in Germany, are based solely on the continuation of historical healthcare capacities rather than on empirical analyses of demand and supply (52–54). There is a lack of specific and systematic structures for psychotherapeutic care research in Germany (e.g., a longitudinal, nationwide, state-funded, and multimodal empirical monitoring), which are essential to accurately assess the demand for mental healthcare and systematically evaluate and improve access to it (55, 56).
To comprehensively assess the state of psychotherapeutic care it is necessary to use valid measures for the need and demand for, the service use and provision, and the availability and accessibility of psychotherapeutic care. Therefore, different data sources are needed, such as epidemiological studies, administrative data, and reports of psychotherapists and patients themselves. Epidemiological data can be used to quantify the theoretical need for psychotherapy by estimating the prevalence of mental and behavioural disorders indicating psychotherapy. Administrative data, derived from billing data provided by SHI agencies, offer objective information on the utilisation of psychotherapeutic services over a specific period of time (e.g., profession of the service provider, coded diagnoses, billed services). Psychotherapists can furnish insights into the demand for psychotherapy (e.g., appointment requests), the need for psychotherapy (e.g., disorder diagnoses, severity of impairment, stress factors in treated patients), and their treatment capacities (e.g., waiting times). Surveys conducted among children, adolescents, or their caregivers can yield data on the self-perceived mental health, demand for psychotherapeutic treatment, and barriers to accessing psychotherapeutic care.
This review aims to provide an overview of the general epidemiological findings on mental and behavioural disorders in children and adolescents in Germany, examine the state of outpatient psychotherapeutic care for this population, and critically discuss various methodological approaches used to assess the state of child and adolescent outpatient psychotherapeutic care. Thus, the following research questions are investigated in this paper:
1. What is the current prevalence of the most common mental and behavioural disorder diagnoses and symptoms in childhood and adolescence in Germany?
2. What is the state of outpatient psychotherapy regarding need and demand, use and provision, and availability and accessibility of care according to the current database?
3. Which methods are used to assess the outpatient psychotherapeutic care for children and adolescents in Germany? Which data is particularly suitable for a valid assessment of the outpatient psychotherapeutic care situation of children and adolescents?
2 Methods 2.1 Literature researchThis review was conducted in accordance with the guidelines proposed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (57). There was no registered protocol. The literature search was conducted in the PubPsych, PubMed, APA PsycInfo, and Google Scholar databases, each consulted last on 25 October 2023. Additionally, we searched in the grey literature database ProQuest on the same day, as administrative data on the mental healthcare system is often not published as empirical studies in scientific journals.
The following English search string was used to identify studies that examined the epidemiology of mental and behavioural disorders in children and adolescents or assessed the state of child and adolescent outpatient psychotherapeutic care in Germany: (((“healthcare” OR treatment) AND (mental OR psychotherap* OR psycholog*)) AND ((“health insurance” OR “claims data”) OR (patient*) OR (*therapist* OR “clinical psychologist*” OR “mental health personnel”) OR ((epidemiolog* OR prevalence OR morbidity) AND ((mental OR psycholog* OR psychopath*) AND (health OR disorder* OR status OR illness* OR depress* OR anxi* OR conduct OR internali* OR externali*))))) AND (child* OR adolescent* OR youth) AND (German* OR Baden-W*rttemberg OR Bavaria OR Berlin OR Brandenburg OR Bremen OR Hamburg OR Hesse OR Mecklenburg-Vorpommern OR “Lower Saxony” OR “North Rhine-Westphalia” OR Rhineland-Palatinate OR Saarland OR Saxony-Anhalt OR Saxony OR Schleswig-Holstein OR Thuringia).
An equivalent German search string was used: ((((Versorgung* OR Behandlung) AND (Psychotherap* OR psycholog*)) AND ((Abrechnung* OR *kasse* OR GKV OR *versicherung*) OR (Patient* OR Betroffene*) OR (*therapeut* OR “KJP” OR Versorger* OR *psycholog*))) OR ((epidemiolog* OR Pr*valenz OR H*ufigkeit*) AND (“psychische Gesundheit” OR “psychische Erkrankung*” OR “psychische St*rung* “OR psychopath* OR psycholog* OR mental* OR Depress* OR $ngst* OR Verhalten* OR internalisierend* OR externalisierend*))) AND (Kinder* OR Jugendliche*) AND ((Deutschland OR deutsch* OR “BRD” OR Bundesrepublik) OR Baden-W*rttemberg OR Bayern OR Berlin OR Brandenburg OR Bremen OR Hamburg OR Hessen OR Mecklenburg-Vorpommern OR Niedersachsen OR Nordrhein-Westfalen OR Rheinland-Pfalz OR Saarland OR Sachsen-Anhalt OR Sachsen OR Schleswig-Holstein OR Th*ringen).
For the search in Google Scholar the first 1,000 search results for the English and German search words were retrieved via “Harzing’s Publish or Perish” tool (58). English search words for Google Scholar were: outpatient, psychotherapy, care, children, adolescents, Germany. The equivalent German search terms were: ambulant, Psychotherapie, Versorgung, Kinder, Jugendliche, Deutschland. If available at the respective databases, we used automatic filters as follows: The search terms named above had to appear in the title and/or abstract of the papers and the papers had to be published between January 2018 and December 2023.
We identified additional studies via the ancestry approach by examining reference lists of studies included in this review and of reviews and meta-analyses on the same topic. The first author and a research assistant manually screened the identified studies multiple times based on titles and abstracts. Eligible studies were then textually reviewed, and the results were summarised in tables. The second author confirmed the literature search and inclusion process.
Results were filtered further using the following inclusion criteria: The publications should be written in the German or English language. They should include either epidemiological data on the mental health or data on the psychotherapeutic care of children and adolescents in Germany (i.e., administrative data, reports from psychotherapists or patients on demand, use and accessibility of psychotherapeutic care). They should further present quantitative primary data of community samples of children and adolescents.
Publications on data from other countries but Germany, data from only adult populations, clinical samples, or other specific subsamples of children and adolescents (e.g., children and adolescents of parents with mental or behavioural disorders, children and adolescents with migration history) were excluded. Further exclusion criteria comprised publications focusing solely on psychiatric, paediatric, or other medical care, healthcare cost analyses, analyses of care pathways and treatment quality, and studies reporting only on attitudes towards mental healthcare. Research evaluating specific intervention programmes and methods was also excluded. Additionally, epidemiological studies on specific symptoms or syndromes not matching an ICD-10 mental or behavioural disorder diagnosis or studies in which prevalence of mental health problems was only a secondary outcome met exclusion criteria. Opinion papers, statements, comments, reviews, and meta-analyses without original primary data were not included. If data was both analysed on the state and federal level, state reports were excluded if their data was included in a federal report (e.g., “DAK Gesundheitsreport”). If multiple publications reported on the same data (e.g., studies published in English and in German), they were regarded as one publication but all versions were cited.
The process of study selection is depicted in Figure 1.
Figure 1. Process and results of literature research. Adapted from Page et al. (118).
2.2 Synthesis of resultsIn order to critically examine the suitability and investigated constructs of different methods to assess the state of the outpatient psychotherapeutic care for children and adolescents, the included studies were sorted into four categories according to data source or research focus: epidemiological studies, administrative studies, psychotherapists’ reports, and patients’ reports. The latter could include assessments of the psychotherapeutic care by the potential patients themselves (i.e., children and adolescents) or their caregivers. If a study reported on both mental health problems and psychotherapeutic care from the point of view of children, adolescents, and/or caregivers, it was listed in both categories, epidemiological studies and patient reports. Epidemiological studies were specifically sought to answer the first research question. All data sources were assessed to answer the second and third research question. If applicable, data on epidemiology of mental and behavioural disorders and on the provision of psychotherapeutic care was summarised separately for each data source. We sorted epidemiological studies by the age of the assessed children and adolescents (<six years, six–12 years, > 12 years) to account for age effects in the prevalence and incidence of mental and behavioural disorder diagnoses and symptoms. As the COVID-19 pandemic led to both a disruption of the healthcare system and an increase of mental distress in children and adolescents, data on the epidemiology of mental and behavioural disorder diagnoses and symptoms and on the provision of mental healthcare from before (i.e., until 2020) and during the COVID-19 pandemic (i.e., from 2020) were analysed separately.
3 Results 3.1 Overview of included studiesIn total, we included 41 studies, published between April 2018 and November 2023. The included studies were summarised in four tables: Table 1 displays the 18 epidemiological studies. Table 2 depicts the 15 publications on administrative data. Table 3 includes the seven studies on psychotherapists’ reports and Table 4 summarises the remaining four studies on patient reports. Three studies were listed in two categories (59–61) because they contained information on both epidemiology and mental healthcare provision from the patients’ perspective.
Table 1. Overview of epidemiological studies.
Table 2. Overview of administrative data.
Table 3. Overview of psychotherapist reports.
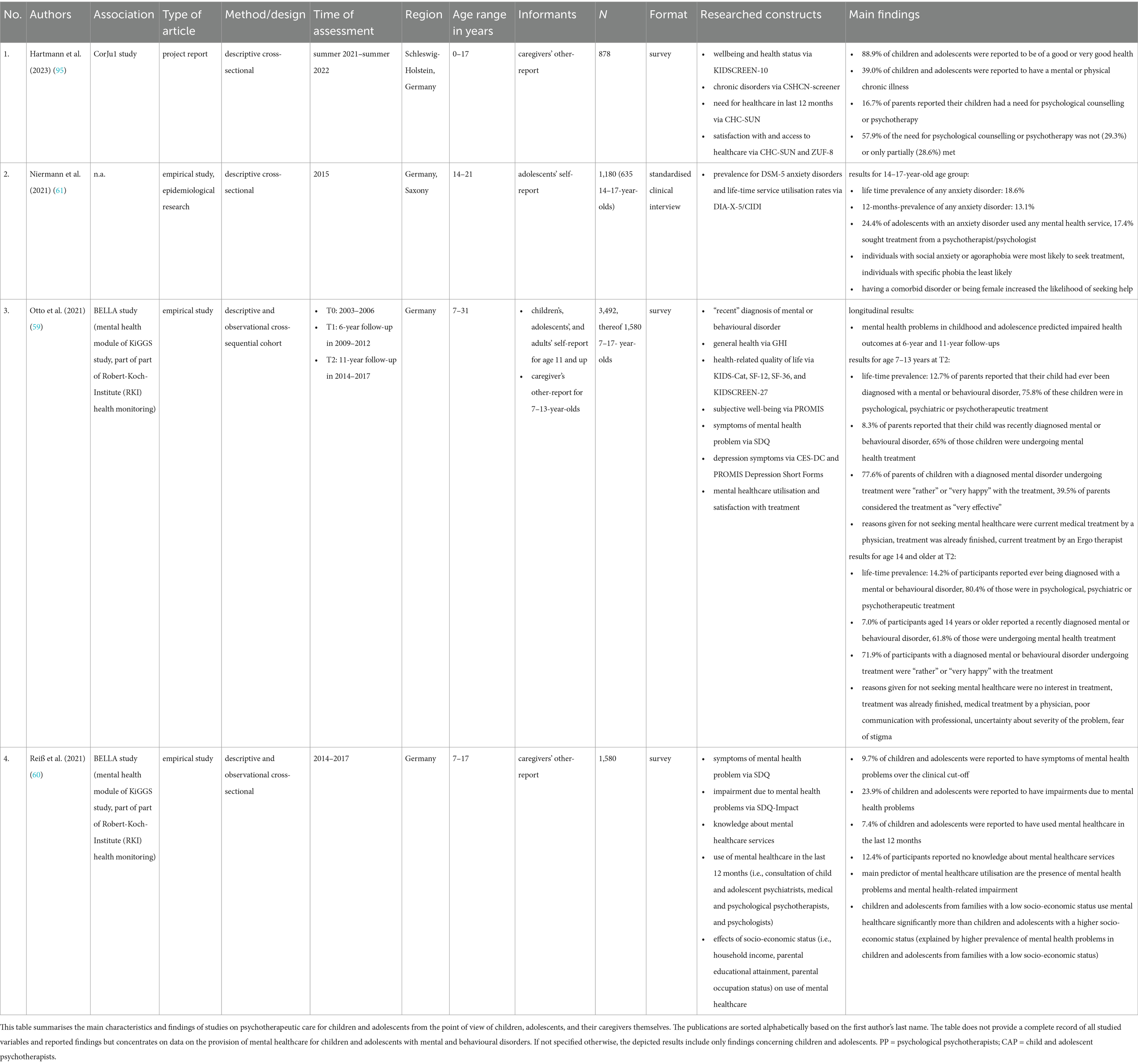
Table 4. Overview of patient reports.
3.2 Epidemiological studiesEighteen epidemiological studies on the prevalence of mental or behavioural disorder diagnoses and/or symptoms in German children and adolescents were identified. Ten of these studies had multiple waves of assessment, while eight only had one. Nine studies were last conducted during the COVID-19 pandemic (i.e., between 2020 and 2022) (21, 62–70). The remaining studies were last conducted between 2014 and 2018 (59–61, 71–76). Ten papers are based on the KiGGS- (71, 73), BELLA- (59, 60, 70), or COPSY-study (21, 59, 65–70), which are three interconnected study projects. Therefore, these studies partially report on the same samples.
Three studies cover an age range from one to three until 18 years (62, 63, 73). Only two studies concentrate on younger children between 1 and 6 years (64, 72), while eight studies include older children and adolescents aged seven to 18 years (21, 60, 65–70), and five studies focus only on adolescents aged 11–17 years (61, 71, 74–76).
Only two studies investigate the prevalence of mental or behavioural disorder diagnoses (59, 61), while the rest of the studies investigate a multitude of symptoms of mental or behavioural disorders. One study used in-person structured clinical interviews (61), two studies used standardised telephone interviews (74, 76), and the remaining 15 studies used standardised online or paper-pencil questionnaires to assess symptoms of mental and behavioural disorders. Twelve studies used children’s or adolescents’ self-report (21, 59, 61, 65–71, 74–76), whereas 14 studies used caregiver-reports (21, 59, 60, 62–73).
The detailed prevalence data for the different age groups is presented in Table 5. The data suggests a sharp increase in a variety mental health problems and symptoms of mental and behavioural disorders in the first year of the COVID-19 pandemic, followed by a decrease in prevalence after 2020 (21, 65–70). The latest studies from 2020 to 2022 suggest that every third to every fourth German child and adolescent suffers from clinically relevant mental health problems (21, 59, 60, 64–70). However, the high variance in methodology, included age groups, and researched outcomes between studies, as well as small numbers of studies investigating the same symptom complex or disorder, do not allow for further conclusions.
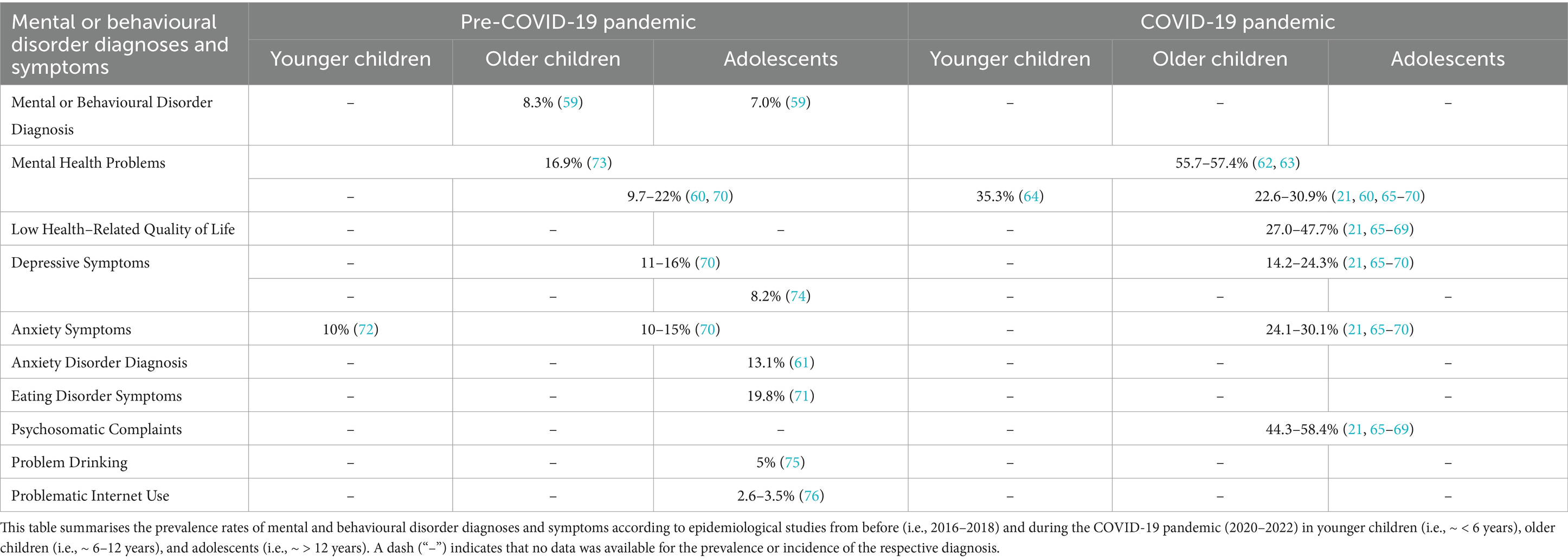
Table 5. Overview of epidemiological prevalence rates of mental or behavioural disorder diagnoses and symptoms.
3.3 Administrative dataWe found 15 publications reporting on administrative data on the prevalence and incidence of mental and behavioural disorder diagnoses in children and adolescents in routine practice and on the use of SHI-funded mental healthcare in Germany. Most of these publications reported on broad age ranges from zero to 19 years. Many included data collected over a span of multiple years, five using data from 2009 until 2019 (50, 55, 77–79), three using data from until 2022 (80–82), and the remaining seven being conducted between 2015 and 2020 (51, 55, 83–87).
Eight of these reports were provided by individual German SHI agencies (DAK, BARMER, AOK), with six belonging to the “DAK Gesundheitsreport” series (51, 79–81, 83–86). Five more studies were conducted in association with the German Central Institute for SHI Physicians (50, 55, 77, 82, 88). One study used data from the German Pharmaco-Epidemiological Research Database which combines billing data of four SHI agencies (78). One study analysed records from psychotherapist practices in Germany (87).
3.3.1 Prevalence and incidence rates of mental and behavioural disorder diagnosesTen publications report on prevalence or incidence rates of mental or behavioural disorders according to SHI billing data. Most of these papers define a case of a mental or behavioural disorder as the presence of an ICD-10 F-diagnosis (F0–F99), which was at least once coded in the billing data by a practitioner (e.g., paediatrician, psychotherapist, psychiatrist) for a patient in a respective time. The studies consistently report that 26–28% of children were diagnosed with a mental or behavioural disorder both before and during the COVID-19 pandemic (51, 81, 83–85). Around half of these diagnoses are developmental disorders (ICD-10 F8), one third are behavioural and emotional disorders with onset in childhood and adolescence (ICD-10 F9), 10% are anxiety, dissociative, stress-related, somatoform, and other nonpsychotic mental disorders (ICD-10 F4), and 2% mood disorders (ICD-10 F3) (50, 51, 83–85). The prevalence and incidence of specific ICD-10 diagnoses before and during the COVID-19 pandemic are displayed in Table 6.
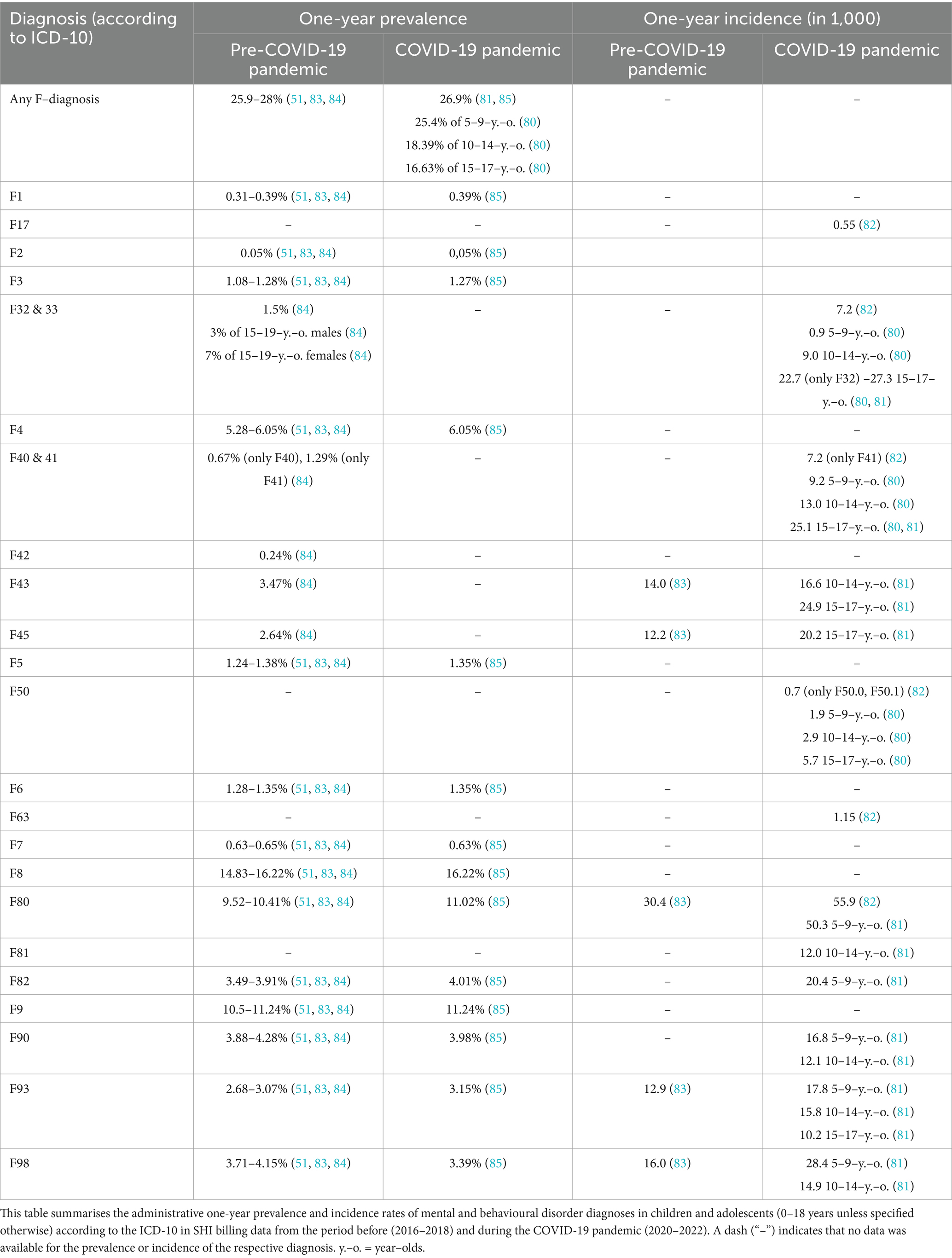
Table 6. Overview of administrative prevalence rates of mental or behavioural disorder diagnoses in SHI billing data.
The publications indicate a small but steady increase of mental and behavioural disorder diagnoses before the COVID-19 pandemic, which was followed by a general decrease in use of healthcare services and incidence numbers of most mental and behavioural disorders during the pandemic (80, 81, 83). However, while the incidence of behavioural disorders seemed to stay constant or decrease, multiple papers report a disproportionate increase in incidence numbers of depressive, anxiety, and eating disorders among female adolescents during the pandemic (80–82).
Over the lifespan, data conclusively shows a linear increase in prevalence of mental or behavioural disorders until age five, followed by a steady linear decrease in prevalence (50, 51, 84). While male children and adolescents are more often diagnosed with a mental or behavioural disorder than female children and adolescents until age 15, from age 15 more female than male adolescents are diagnosed (50, 51, 82, 84–86). In childhood, mental and behavioural disorder diagnoses are dominated by developmental and behavioural disorders (ICD-10 F8 & F9); in adolescence the most prevalent disorders are mood and anxiety disorders (ICD-10 F3 & F4) (53, 58, 59, 61–63). Specifically, the highest prevalence rates of developmental and behavioural disorders (ICD-10 F8 & F9) are found in male children, whereas prevalence rates of substance use, anxiety, eating, and personality disorders (ICD-10 F1, F3, F4, F5 & F6) are highest among female adolescents (50, 51, 82, 84–86).
3.3.2 Use and provision of statutory health insurance funded mental healthcareTwelve publications provide data on access and use of SHI-funded outpatient mental healthcare (i.e., any medical or psychological treatment of a mental or behavioural disorder provided by a physician, psychologist, or psychotherapist), some of them also more specifically on psychotherapeutic care. However, the papers differ greatly in their definitions of psychotherapeutic services/psychotherapeutic care, which leads to variance in the provided data.
Nonetheless, the data conclusively shows that there is a general increase in the use of psychotherapeutic care from age five: While less than 1% of under 5-year-olds are in psychotherapeutic care, around 6% of 5–9-year-olds and 11% of 10–19-year-olds receive psychotherapeutic treatment (55, 79, 84, 86, 88). Consistent with gender differences in prevalence of mental and behavioural disorders, more male than female children use psychotherapeutic care in late childhood, whereas more female than male adolescents receive psychotherapeutic care in adolescence (50, 79, 84, 86).
In the years shortly before the COVID-19 pandemic (i.e., 2017–2019) the publications indicate that between 5 to 7% of all children and adolescents used outpatient mental healthcare services in the broader sense (i.e., psychotherapeutic/psychiatric consultations, medical coordination, verbal interventions, functional developmental therapy, probationary sessions, guideline-based psychotherapy provided by a paediatrician, psychiatrist, medical, psychological, or child and adolescent psychotherapist) (84, 88). 0.2–2% of all children and adolescents were reported to receive psychotherapeutic care in the narrower sense in a year (i.e., guideline-based psychotherapy provided by a medical, psychological, or child and adolescent psychotherapist) (55, 79, 86). Over a span of 10 years, 10% of all children and adolescents were recorded to have accessed guideline-based psychotherapy (50, 79). Of those children and adolescents who were newly diagnosed with a mental or behavioural disorder, nearly half received only initial consultations and no further treatment, and only one in ten of those children and adolescents received guideline-based psychotherapy (50, 86).
Data further reveals that 97% of children and adolescents with a mental or behavioural disorder sought treatment from a general practitioner or a paediatrician, while only half sought treatment from a psychiatrist or psychotherapist (50). However, the prevalence of cases treated by psychotherapists increased over the years before the COVID-19 pandemic (86). Most patients receiving psychotherapeutic care in the broader sense were treated by a psychiatrist, whereas the most frequent providers of guideline-based psychotherapy were child and adolescent psychotherapists (55, 88).
Information on waiting times between the initial consultation and the start of guideline-based psychotherapy is scarce in the included publications but indicates that half of patients got initially diagnosed and started guideline psychotherapy in the same quarter of the year, while on average patients had to wait 22 weeks between the initial consultation and the start of guideline-based psychotherapy (79, 87).
Diagnoses most frequently treated in psychotherapeutic outpatient care included anxiety, compulsive and stress-related disorders (ICD-10 F40, F41, F42 & F43), depressive disorders (ICD-10 F32 & F33), hyperkinetic disorders (ICD-10 F90), and emotional disorders with onset in childhood (ICD-10 F93) (55, 79, 84, 88). However, there is strong variance in the reported proportions of these diagnoses in outpatient psychotherapeutic care between different publications.
During the COVID-19 pandemic, the reports recorded a general decrease in use of healthcare services, including visits to paediatricians, psychiatrists, and psychotherapists, particularly during the first lockdown in spring 2020 (81, 84, 85). Consequently, administrative incidence rates of most mental and behavioural diagnoses initially dropped. After the first lockdown the amount of contacts surpassed the pre-pandemic level (85). Two years into the pandemic, data shows that significantly less younger children and significantly more adolescents receive outpatient psychotherapeutic care than before the pandemic (80).
3.4 Psychotherapists’ reportsSeven studies assessed the state of psychotherapeutic care for children and adolescents, particularly waiting times and provided services, from the perspective of psychotherapists. Two of these studies were conducted in 2017 to 2018 during the introduction of the obligatory initial psychotherapeutic consultation. The rest of the studies were conducted between 2020 and 2022.
It was shown that the introduction of the obligatory initial psychotherapeutic consultation in 2017 led to an increase in patients accessing care, however, at the same time also to an increase of waiting time for guideline-based psychotherapy (44, 89). During the pandemic, psychotherapists consistently reported a growing demand and need for psychotherapy due to pandemic-related increases in mental disorders and deterioration of existing mental health problems (48, 90–93).
The studies concordantly report that psychotherapists received five to six requests for an initial appointment per week, of which only one third could be offered an appointment during the pandemic (45, 46, 48, 89, 94). Waiting times for an initial psychotherapeutic consultation seem to have increased from approximately 5–6 weeks before the pandemic to 6–10 weeks during the pandemic (44–46, 48, 89, 94). After the initial consultation, patients had to wait another 4 months before the pandemic and 3–7 months during the pandemic to start guideline-based psychotherapy (44–46, 48, 89, 94). Roughly every second child or adolescent had to wait over a month for a consultation after receiving an appointment and more than 6 months for the start of guideline-based psychotherapy during the pandemic (45, 46). However, multiple studies found high variance in waiting times between individual practices and between regions (44–46, 89). Furthermore, psychotherapists stated that they found it very difficult or even impossible to refer patients to other therapists before and during the pandemic (44, 94).
3.5 Patients’ reportsFour included studies investigated the provision psychotherapeutic care for children and adolescents from the perspective of the patients’ or their families themselves. Three of these studies were conducted between 2014 to 2017 before the introduction of the obligatory initial psychotherapeutic consultation, while one study was conducted during the COVID-19 pandemic in 2021 and 2022.
The studies show that approximately 7% of the general population children and adolescents reported using mental healthcare in the broader sense (i.e., at least one consultation at a psychiatrist, psychotherapist or psychologist) before the pandemic (60). In a sample of children and adolescents with a diagnosed mental or behavioural disorder, about two thirds to three quarters of those children and adolescents were reported to received such care (59). During the COVID-19 pandemic, circa 17% of caregivers stated that their child was in need of mental healthcare, while this need was not or only partially met in the majority of cases (95). Reasons for the discrepancy between the perceived and actual need for psychotherapeutic treatment and the care received include a lack of awareness about mental healthcare services, treatment by other professionals, fear of stigma, and other factors. Socio-economic status, the severity of mental health problems and related impairment, the specific diagnosis and comorbidities, and gender moderated the likelihood of seeking help for mental health problems (60, 61, 95).
4 DiscussionWorldwide, increasing numbers of children and adolescents are affected by mental or behavioural disorders requiring psychotherapeutic treatment, but often face barriers to accessing outpatient psychotherapeutic care. Here, we present a scoping literature review on the state of outpatient psychotherapeutic care for children and adolescents in Germany and its assessment. In Germany, mental healthcare is predominantly funded by statutory health insurance (SHI) and offers high treatment capacities in the inpatient sector, but reportedly lacks sufficient treatment capacities in the outpatient sector in comparison to other high-resource countries. Comprehensive, systematic, and multimodal analyses of psychotherapeutic care provision, necessary for empirically-based demand planning, are lacking. This review was conducted according to PRISMA-ScR guidelines (57). We included 41 papers based on epidemiological studies, administrative data, and provider and patient reports and published between April 2018 and November 2023. Our assessment focussed on the prevalence and incidence rates of mental and behavioural disorder symptoms and diagnoses, as well as the demand and need for, the provision and use, and the availability and accessibility of outpatient psychotherapeutic care in German children and adolescents. Additionally, we examined the suitability of different data sources for adequately assessing outpatient psychotherapeutic care.
4.1 Prevalence of mental and behavioural disorder diagnoses and symptoms in German children and adolescentsBased on epidemiological studies, we aimed to address the first research question concerning the prevalence of mental and behavioural disorder symptoms and diagnoses in children and adolescents in Germany in recent years. Unfortunately, we found very few studies using systematic and standardised clinical interviews to estimate disorder prevalence rates. There seems to be a lack of epidemiological data on mental and behavioural disorders in German children and adolescents, in particular in younger children. Older national and international reviews and meta-analyses estimated the prevalence of mental and behavioural disorders in childhood and adolescence to range between 10 and 25%, with significant variance in the time of assessment, case definition, and methodology (1–3, 96, 97). A promising and more recent Austrian study from 2016 assessed the prevalence of mental and behavioural disorders according to the DSM-5 in 10–18-year-olds with both clinical questionnaires and a structured interview and showed that 23.9% of children and adolescents met the criteria of a mental or behavioural disorder (98). When comparing these studies, it is important to note that only one exclusively reported on children and adolescents in Germany (96). Additionally, some of the reviews include data dating back to the 1970s, with one study even reaching back to the 1950s. Although epidemiological estimates are generally considered to be more stable and less time-sensitive, it is likely that the prevalence rates of mental and behavioural disorders in children and adolescents have changed over the last decades due to shifts in their environments (e.g., political and societal developments, exposure to global crises, digitalization). Moreover, the conceptualization and diagnostic criteria for mental and behavioural disorders have evolved over time, which is likely to influence epidemiological data. However, the impact of these changes cannot be estimated based on the current research, as recent epidemiological data on German children and adolescents is lacking.
Nevertheless, we found several studies using clinical questionnaires to assess the prevalence of self- or caregiver-reported mental health problems or psychopathological symptoms as an estimate of child and adolescent mental health, especially during the COVID-19 pandemic. This data suggests a general increase in mental health problems from before the pandemic to during the pandemic, followed by a slow decrease after the initial year of the pandemic in 2020 (21, 60, 65–70). Studies conducted between 2020 and 2022 indicate that at least every third to every fourth child and adolescent was affected by mental health problems during the pandemic (21, 65–70). However, the high variance in methods, researched constructs, and included age groups limits the synthesis of these studies’ results. Questionnaire data alone also does not allow for conclusions on disorder prevalence rates. Furthermore, studies on the mental health of children and adolescents conducted after 2022 are still lacking.
Consequently, the first research question “What is the current prevalence of the most common mental and behavioural disorder diagnoses and symptoms in childhood and adolescence in Germany?” cannot be sufficiently answered in light of the current database due to a lack of recent, systematic, standardised, and longitudinal epidemiological data. This underscores the urgent need for standardised, systematic, and longitudinal assessments of child and adolescent mental health in Germany beyond mere questionnaire measures.
4.2 Current state of outpatient psychotherapyWe attempted to evaluate the current state of outpatient psychotherapeutic care by examining both epidemiological and administrative data, alongside reports from psychotherapists, as well as children, adolescents, and their families as potential patients. Specifically, we aimed to estimate the need and demand for, the use and provision of, and the accessibility and availability of psychotherapeutic care to address our second research question.
4.2.1 Need and demand for psychotherapeutic careAs discussed above, there is a lack of studies estimating the prevalence of mental and behavioural disorders indicating psychotherapeutic treatment in children and adolescents in Germany. Consequently, it is difficult to estimate the objective need for psychotherapeutic treatment based on recent epidemiological data.
Recent data from the statutory healthcare system indicates that the prevalence rates of mental and behavioural disorders among children and adolescents are slightly higher than those reported in older epidemiological studies, now ranging between 26 and 28% (51, 81, 83–85). However, these administrative numbers do not reflect the objective need for psychotherapy but merely the number of billed diagnoses in routine care, which usually have lower validity than diagnoses derived from epidemiological studies. Although most mental and behavioural disorders can be treated with psychotherapy, certain disorders are not primarily an indication for psychotherapy, e.g., intellectual disabilities (ICD-10 F7) or developmental disorders (ICD-10 F8). As these disorders are usually included in the general administrative estimate of mental and behavioural disorders, these estimates do not equal the need for psychotherapy. In fact, roughly half of all mental and behavioural disorder diagnoses in routine care are developmental disorders (50, 51, 83–85). Thus, according to administrative data, it can be cautiously estimated that only 13–14% of all children and adolescents have a diagnosis a mental or behavioural disorder that can be primarily treated with psychotherapy (e.g., emotional and behavioural disorders with onset in childhood and adolescence [ICD-10 F9], anxiety, compulsive and stress-related disorders [ICD-10 F4], mood disorders [ICD-10 F3]). However, this number does not include children and adolescents who might fulfil the criteria of a mental or behavioural disorder but have not yet been diagnosed in routine care. At the same time, it may include a significant number of false-positive diagnoses, as the diagnostic quality is not accounted for in routine data, leading to concerns about the validity of these diagnoses.
Regarding the subjective need or demand for psychotherapy, we again did not find many studies examining children’s and adolescents’ self-assessed or caregiver-assessed need or wish for treatment. One study reported that during the COVID-19 pandemic, around 17% of caregivers stated that their child was in need of mental healthcare and that this need was not or only partially met in the majority of cases (95). Taken together with the data from epidemiological and administrative data, it can be cautiously summarised that roughly every sixth to seventh child and adolescent in Germany is in need of psychotherapeutic treatment. This equates to approximately three million children and adolescents (99).
4.2.2 Use and provision of psychotherapeutic careIt is important to note that the publications we reviewed vary in their definitions of mental or psychotherapeutic healthcare and frequently do not provide data specifically on psychotherapeutic care. These inconsistencies contribute to significant variance in data and, at times, result in contradictory findings.
Administrative data suggests that nearly all families with children and adolescents with a mental or behavioural disorder initially consult a paediatrician or general practitioner regarding the child’s or adolescent’s mental health problems (50). Only half of them come into contact with a mental health specialist, e.g., a psychiatrist or psychotherapist (50). Other publications suggest that only 5–7% of all children and adolescents, and therefore only a quarter to a third of children and adolescents with a mental or behavioural disorder, receive mental healthcare in the broader sense (84, 88). This includes services provided not only by a medical, psychological, or child and adolescent psychotherapist but also by a general practitioner, paediatrician, or psychiatrist in connection to a mental or behavioural disorder diagnosis. Only 0.2–2% of all children and adolescents receive guideline-based psychotherapy, translating to up to 10% of children and adolescents with a mental or behavioural disorder (55, 79, 86).
Regarding age and gender differences in the use of mental healthcare, administrative data suggests a peak in diagnosis prevalence at age five, as most developmental disorders are diagnosed at this age (50, 51, 84). Until age 15, more male than female children and adolescents are diagnosed; afterwards, more female than male adolescents receive a diagnosis (50, 51, 82, 84–86). This aligns with gender differences in the type of diagnosis: while male children and adolescents are more frequently diagnosed with developmental and behavioural disorders, typically occurring first in early childhood, female children and adolescents are more often diagnosed with mood, anxiety, eating, personality, and substance abuse disorders, which typically only start in late childhood or adolescence (50, 51, 82, 84–86). These trends are also reflected in age and gender differences in the use of mental healthcare (50, 79, 84, 86). However, psychotherapy is mostly used by older children and adolescents and less by younger children (55, 79, 84, 86, 88).
Considering changes over time, it seems that an increasing number of children and adolescents are treated by psychotherapists, while fewer cases are only treated by a paediatrician or general practitioner (50). This coincides with the introduction of the obligatory initial psychotherapeutic consultation in 2017, which every SHI-accredited psychotherapist in private practice is required to provide. This initial consultation serves as a preliminary diagnostic assessment and treatment recommendation, as well as a first step in accessing psychotherapeutic care. However, an appointment for an initial consultation often does not result in a therapy place at the respective practice. Data shows that due to this reform, significantly more patients access psychotherapeutic care, while waiting times for guideline-based psychotherapy further increase (44, 87, 89). This is because the required number of initial consultations a practice must provide reduce the capacity for guideline-based psychotherapy sessions. The COVID-19 pandemic put a heavy strain on the healthcare system in general and therefore also affected the provision of psychotherapeutic care. Administrative data indicates a general decrease in psychotherapeutic service provision and administrative incidence rates at the start of the pandemic in 2020 (81, 83, 85). However, following the first lockdown, an increase in the administrative incidence of certain mental and behavioural disorders, surpassing pre-pandemic levels, was recorded (80, 85). Psychotherapists also reported a heightened demand for psychotherapy and pandemic-associated deteriorations in mental health (48, 90–93).
4.2.3 Availability and accessibility of psychotherapeutic careWaiting times for treatment are often used as a marker of the availability of care. In the studies we reviewed, we found high variance in waiting times for an initial consultation and guideline-based therapy both between regions and between individual practices. This disparity is concerning in a healthcare system founded on the principle of solidarity, which aims to ensure equal access to care nationwide. Furthermore, chances of even receiving an appointment are unacceptably low, with waiting times reported to be excessively long and having doubled during the COVID-19 pandemic (45, 46, 48, 94). Psychotherapists reported receiving five to six requests for an initial appointment per week, of which only one-third resulted in an appointment (45, 46, 94). Half of the patients waited longer than 4 weeks for an initial consultation and more than 6 months for the start of guideline-based psychotherapy (45, 46). Given the time-sensitive development of children and adolescents, these difficulties in obtaining an appointment, followed by extensive waiting times, can lead to an exacerbation of symptoms, impaired psychosocial development, and damage to social participation. Additionally, they can result in reduced trust in the healthcare system and decreased motivation to seek professional help.
Research on individual barriers to accessing psychotherapeutic care for children and adolescents is still lacking. Nevertheless, we found indications that limited knowledge about mental health and mental healthcare services, fear of stigma, and negative experiences in the healthcare system are associated with a reduced likelihood of attempting to access psychotherapeutic care (59). Gender, socio-economic status, specific diagnoses, and severity of mental health problems and related impairment seem to moderate the motivation to seek care (60, 61).
Taken together, considering the second research question “What is the state of outpatient psychotherapy regarding need and demand, use and provision, and availability and accessibility of care according to the current database?,” we found a wide range of data on psychotherapeutic care for children and adolescents in Germany, allowing for some conclusions about the need and demand, service use and provision, and availability and access to care. It seems that the number of children and adolescents receiving psychotherapeutic treatment is far smaller than the number estimated to have an objective or subjective need for this treatment. While the demand for psychotherapeutic care appears to be rising—likely due to factors such as increased awareness, de-stigmatisation, and the effects of global crises—the capacities of psychotherapeutic care have not been adequately adjusted, leading to impaired access to care and long waiting times. However, these conclusions should be interpreted with caution, as we had to compare results from different data sources which vary greatly in their content, methodology, and study purposes. The current database is very fragmented, and the data available on specific constructs is often very limited. Systematic, multimodal, comprehensive, and longitudinal assessments are necessary to reliably assess the state of the psychotherapeutic care system, which unfortunately do not exist. Thus, this question remains partially answered but requires m
Comments (0)