
Remember me
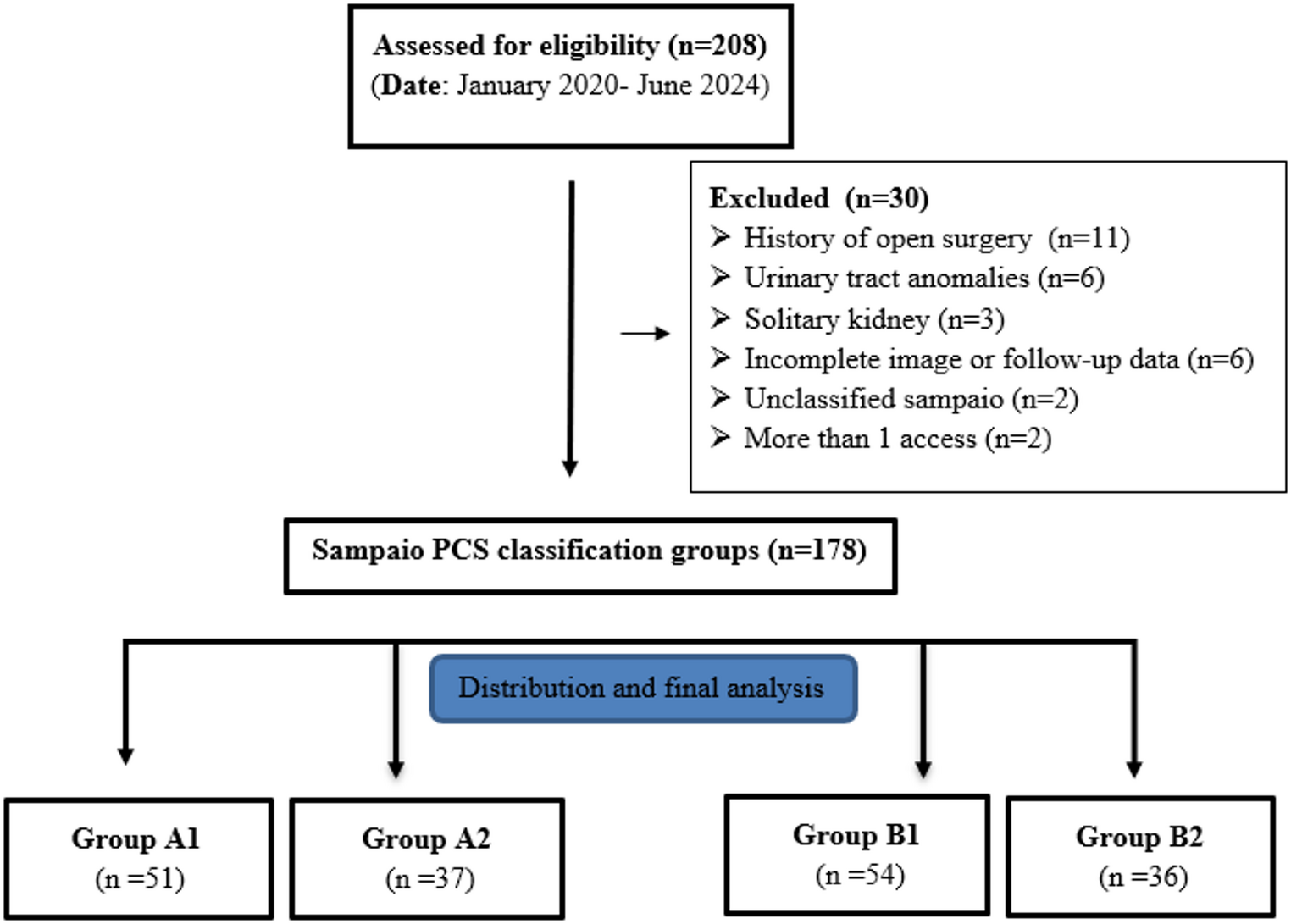
This study analyzed data from the NHANES, a nationally representative cross-sectional survey by the Centers for Disease Control and Prevention (CDC) assessing the health and nutritional status of the U.S. population. Detailed information regarding the survey’s design, methodology, and estimation data can be accessed at https://www.cdc.gov/nchs/nhanes/?CDC_AAref_Val=https://www.cdc.gov/nchs/nhanes/index.htm. The protocols of NHANES were approved by the NCHS Research Ethics Review Board, and all participants provided written informed consent. Participants aged 20 years and older from the 2007–2018 cycles were included. Participants aged 18–19 years were excluded to improve comparability with existing literature and focus on a more stable adult population. Individuals with missing data on FI, SII, all-cause mortality, or key covariates (e.g., age, race, smoking, drinking) were excluded, resulting in a final sample of 2,620 participants (Fig. 1). The assessment of kidney stone history was derived from the question: “Have you ever had kidney stones?”
Fig. 1
The participant screening process
Exposure: frailty index (FI)Frailty was assessed using a 49-item Frailty Index (FI) that measures deficits in cognitive function, dependency, depression, comorbidities, hospitalizations, general health, anthropometry, and laboratory results. Items were scored as (no deficit) or 1 (presence of deficit), and the FI was determined by dividing the total number of deficits by the total items assessed [13]. Based on existing literature [14], participants were classified into three categories: non-frailty (FI ≤ 0.10), pre-frailty (0.10 < FI ≤ 0.21), and frailty (FI > 0.21).
Outcome: all-cause mortalityMortality data were sourced from the National Death Index (NDI), a comprehensive database of U.S. death certificates. Follow-up duration, measured in months, spanned from the NHANES interview date to either the date of death or the end of the follow-up period on December 31, 2019. The main variable assessed was all-cause mortality.
Mediator: systemic immune-inflammation index (SII)SII, calculated as (Platelet count × Neutrophil count)/Lymphocyte count, serves as a composite biomarker of systemic inflammation and immune response, where elevated values denote increased inflammatory burden [15]. NHANES-based studies have validated SII’s association with metabolic and cardiovascular outcomes.
CovariatesTo reduce confounding effects, we identified key factors: age (< 60, ≥ 60 years), sex (male, female), ethnicity (Non-Hispanic White, Mexican American, Non-Hispanic Black, Other), marital status (married/living with partner, living alone), education (less than high school, high school or equivalent, above high school), family income, body mass index(BMI), smoking (never, former, current) [16], drinking (no, yes) [17], hypertension, and diabetes mellitus. Family income was categorized by the poverty income ratio (PIR): low (PIR ≤ 1.3), medium (PIR > 1.3 to 3.5), high (PIR ≥ 3.5). Chronic diseases were defined by self-reported diagnoses by healthcare professionals. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation [18]. Physical activity was classified by moderate-intensity exercise duration: “below” (< 150 min/week), “meet” (150–300 min/week), or “exceed” (≥ 300 min/week) according to established guidelines [19].
Statistical analysisThe normality of variables was assessed using histogram distribution, Q-Q plot, or Kolmogorov-Smirnov test. Normally distributed continuous variables were reported as mean ± SD, while skewed continuous variables were presented as median (interquartile range [IQR]). Categorical variables were expressed as frequencies (%). Group comparisons for continuous variables were conducted using independent samples Student’s t-test or Mann-Whitney U-test based on the distribution normality, and categorical data were compared using chi-square or Fisher’s exact test as applicable.
Hazard ratios (HRs) and 95% confidence intervals (CIs) were computed to analyze the association between the FI among kidney stone patients and All-Cause Mortality using Cox proportional hazards models. Both unadjusted and multivariate-adjusted models were employed, with participants who were lost to follow-up being censored at the specific time point. Kaplan-Meier survival analyses were utilized to examine the relationship between frailty status (categorized as non-frailty, pre-frailty, and frailty) and all-cause mortality. Survival probabilities were stratified based on frailty status over two temporal dimensions: follow-up duration (months) and age (years). Between-group differences in survival distributions were assessed using the log-rank test.
The FI was treated as a continuous variable (per 10-unit increase). Confounders were selected on their associations with the outcomes of interest or a change in effect estimate of more than 10%. Three models were constructed: Model 1 was unadjusted, Model 2 was adjusted for age, sex, and race, and Model 3 additionally adjusted for education level, marital status, family income, hypertension, diabetes, smoking status, drinking status, and BMI.
We conducted restricted cubic spline model to develop smooth curves to examine the possible nonlinear dose-response associations between FI among kidney stone patients and All-Cause Mortality. In this model, FI was used as a continuous variable. If a non-linear correlation was observed, a two-piecewise regression model was performed to calculate the threshold effect of FI on All-Cause Mortality in terms of the smoothing plot. The subgroup analyses were also performed. For continuous variable, we first converted it to a categorical variable according to the clinical cut point or tertile, and then performed an interaction test. Interaction across subgroups was tested using the likelihood ratio test. The calculated effect sizes and p values from all these models were reported and compared.
Besides, Mediation analysis was conducted to assess whether the impact of the frailty status of such patients on All-Cause Mortality could be elucidated by the SII, delineating the total, direct, and indirect effects. The proportion of the effect ascribed to the mediator was determined by dividing the indirect effect by the total effect. All analyses were performed using R Statistical Software (Version 4.2.2, http://www.R-project.org, The R Foundation) and Free Statistics analysis platform (Version 2.1.1, Beijing, China, http://www.clinicalscientists.cn/freestatistics). Free Statistics is a software package provides intuitive interfaces for most common analyses and data visualization. It uses R as the underlying statistical engine, and the graphical user interface (GUI) is written in Python. Most analyses can be done with just a few clicks. It is designed for reproducible analysis and interactive computing. A two-sided P value < 0.05 was considered statistically significant.
Comments (0)