
Remember me

Semaglutide, approved for the treatment of obesity in 2021, is a GLP-1RA—a class of peptide-based drugs that mimic the effects of the endogenous incretin hormone glucagon-like peptide-1 (GLP-1) [9, 28].
Endogenous GLP-1 is secreted by L-cells in the small intestine in response to food intake. Upon release, it binds selectively to GLP-1 receptors, which are widely distributed throughout the body, including the GI tract, pancreas, brainstem, hypothalamus, and vagal afferent nerves [27,28,29,30]. By binding to these receptors, GLP-1 enhances insulin secretion from pancreatic β-cells and suppresses glucagon secretion in a glucose-dependent manner, slows gastric emptying, and regulates appetite by increasing satiety and promoting a sense of fullness through its action on the hypothalamus [27, 28, 31,32,33].
The US Food and Drug Administration and the European Medicine Agency approve semaglutide under three distinct formulations. The specific indications, preparations, and dosing regimens for each formulation must be carefully considered in clinical practice. Given this complexity, it is essential to understand the unique features and approved uses of each brand, as well as current patterns of off-label prescribing. Table 1 provides a detailed comparison of the different forms of semaglutide, outlining their intended uses, approved patient groups, dosage instructions, notable features, and supporting clinical trials [34].
Table 1 Overview of FDA-approved semaglutide formulationsMechanism of Action, Safety, and EfficacySemaglutide exerts its effects through both central and peripheral pathways, replicating and enhancing the physiological actions of endogenous GLP-1 [35]. Semaglutide is a long-acting human GLP-1 analogue that shares 94% structural homology with native GLP-1. However, compared with native GLP-1, which is rapidly degraded and has a short half-life of approximately 2 min, semaglutide has been structurally modified by the addition of a hydrophilic spacer and a fatty acid side chain, allowing reversible binding to albumin [36]. These modifications significantly prolong its half-life, enabling convenient once-weekly subcutaneous administration [27, 36]. Semaglutide was initially developed for the management of T2D but has also demonstrated substantial efficacy in weight management by mimicking the effects of endogenous GLP-1. Through activation of the GLP-1 receptor, it enhances insulin secretion, suppresses glucagon release, delays gastric emptying, and reduces food intake via central appetite regulation. These mechanisms not only support glycaemic control and metabolic improvements but also contribute to weight loss by increasing satiety, reducing appetite and food cravings, lowering the preference for high-fat and energy-dense foods, and improving overall eating behaviour (Fig. 1) [9, 28, 29, 35,36,37].
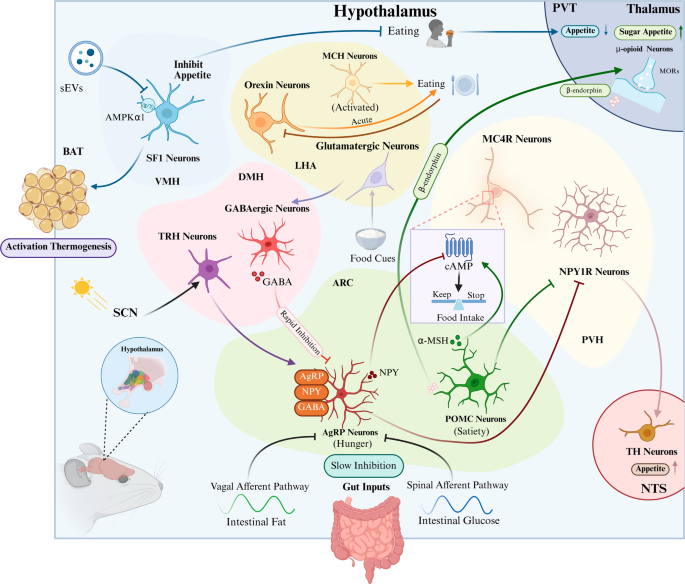
Fig. 1
Effects of semaglutide. Semaglutide mediates physiological effects through GLP-1 receptor activation, including appetite suppression and increased satiety via central pathways, delayed gastric emptying, and enhanced pancreatic insulin secretion accompanied by decreased glucagon release. Abbreviations: GLP-1, glucagon-like peptide-1
The clinical development programme named ‘Semaglutide Treatment Effect in People with obesity (STEP)’ was designed to provide an extensive evaluation of semaglutide for weight management in different patient populations and treatment settings. This series of phase 3, randomised, double-blind, placebo-controlled clinical trials involved more than 25,000 individuals with overweight or obesity and has extensively demonstrated the efficacy of once-weekly subcutaneous semaglutide 2.4 mg in promoting weight loss [13, 38,39,40,41,42,43,44,45,46]. In addition, the STEP trials examined the impact of semaglutide on weight-related complications and potential benefits beyond weight loss.
Table 2 summarises the first 10 STEP trials.
Table 2 Summary of key efficacy and safety outcomes in the STEP programme based on the trial product estimandThe STEP trials assessed the efficacy and safety of semaglutide 2.4 mg in individuals with overweight (BMI ≥ 27.0 kg/m² with at least one weight-related comorbidity) or obesity (BMI ≥ 30.0 kg/m²), both with and without T2D or prediabetes. With the exception of STEP 5 [40] and STEP 10 [42], which differed in trial duration, and STEP 8 [46], which included an active comparator (liraglutide), all trials followed a standardised 68-week treatment period. Participants in all studies received semaglutide or placebo in conjunction with structured lifestyle interventions, including caloric restriction and increased physical activity.
Across the STEP trials, semaglutide 2.4 mg consistently demonstrated statistically and clinically significant weight loss compared with placebo [13, 38,39,40,41,42,43,44,45,46]. Mean percentage reductions in BW with semaglutide 2.4 mg ranged from − 10.6% to − 18.2%, while changes in the placebo groups ranged from − 5.2% to − 0.6%. Clinically meaningful weight loss, defined as a reduction of ≥ 5% in baseline BW, was achieved by 73.2%–92.4% of semaglutide-treated participants, compared with 21.4%–50.0% in the placebo arms [13, 38,39,40,41,42,43,44,45,46]. Notably, the STEP TEENS trial showed that semaglutide 2.4 mg, administered once weekly via subcutaneous injection, can be used in individuals aged 12 years and older, as adolescents with obesity treated with semaglutide experienced a significant reduction in BMI compared with placebo, along with improvements in several cardiometabolic risk factors [47].
Overall, the efficacy of semaglutide in weight reduction was demonstrated in patients both with concomitant T2D—specifically in STEP 2 [39], which included only patients with T2D, as well as in STEP 6, 7, and 10, which included both patients with and without T2D [41,42,43]—and without diabetes (STEP 1, 3, 4, 5, 8, and 9) [13, 38, 40, 44,45,46].
STEP 10 [42] was the first phase 3 trial designed to assess the efficacy of semaglutide 2.4 mg specifically in individuals with obesity and prediabetes. The trial included reversion to normoglycaemia as its primary endpoint and demonstrated that semaglutide significantly increased the rate of glycaemic normalisation compared with placebo, alongside substantial reductions in BW.
Sustained weight loss was maintained over extended treatment durations of up to 104 weeks in STEP 5 [40], while efficacy was also consistent across ethnically diverse populations, as demonstrated in STEP 6 [41] and STEP 7 [43]. Moreover, in STEP 8 [46], semaglutide 2.4 mg exhibited superior efficacy compared with liraglutide 3.0 mg, achieving a mean reduction in BW of more than 10%. In trials with secondary endpoints, such as STEP 9 [38], semaglutide also resulted in significant improvements in obesity-related comorbidities, including osteoarthritis-related pain and rates of reversion to normoglycaemia, further underscoring its broad clinical utility.
Beyond weight reduction and glycaemic control, semaglutide 2.4 mg has demonstrated significant cardiovascular benefits. The SELECT trial (Semaglutide Effects on Heart Disease and Stroke in Patients With Overweight or Obesity), a phase 3 study involving 17,604 adults with overweight or obesity and pre-existing CVD but no diabetes, revealed that once-weekly subcutaneous semaglutide 2.4 mg reduced the risk of major adverse cardiovascular events by 20% compared with placebo over a mean follow-up of 39.8 months, including cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke [48].
Semaglutide 2.4 mg has also shown efficacy in treating obesity-related heart failure with preserved ejection fraction (HFpEF), as demonstrated in the STEP-HFpEF and STEP-HFpEF DM trials evaluating individuals with a BMI ≥ 30.0 kg/m², both with and without T2D. In a prespecified pooled analysis, semaglutide was superior to placebo in improving heart failure-related symptoms and physical limitations, enhancing exercise tolerance, and promoting significant weight loss, underscoring its potential to address both metabolic and functional deficits in obesity-related HFpEF [49].
Additionally, interim findings from the ongoing phase 3 ESSENCE trial suggest that semaglutide 2.4 mg may have a disease-modifying role in metabolic dysfunction-associated steatohepatitis (MASH). After 72 weeks of treatment, participants reported higher rates of histological resolution of steatohepatitis and improvement in liver fibrosis those who received placebo, alongside substantial weight reduction [50, 51].
Regarding the safety profile of semaglutide 2.4 mg, the STEP programme highlighted an AE incidence ranging between 84.3% and 96.1% among treated participants, compared with 75.0%–96.1% in placebo groups [13, 38,39,40,41,42,43,44,45,46]. While overall AE rates were generally comparable between treatment arms, GI AEs were notably more frequent among participants treated with semaglutide, occurring in 41.9%–84.1% of cases, compared with 26.1%–63.2% in placebo groups. The occurrence of GI AEs has led some clinicians to question whether the weight loss observed with semaglutide treatment may be primarily a result of these side effects [52]. However, post hoc and pooled analyses of clinical studies investigating semaglutide in both obesity and T2D have shown that GI AEs—such as nausea, vomiting, and diarrhoea—contribute minimally to overall weight reduction. Data from the STEP [52] and SUSTAIN [53, 54] trials consistently demonstrate that the substantial weight loss achieved with semaglutide at doses of 0.5 mg, 1.0 mg, and 2.4 mg is largely independent of these symptoms, with less than 1% of the total weight loss benefit attributable to GI AEs. This supports the conclusion that semaglutide-induced weight loss is predominantly mediated by mechanisms unrelated to GI side effects [52].
Sex-related Response Patterns To SemaglutideUnderstanding the impact of patient sex on treatment response is critical to optimising obesity therapies [55]. Emerging evidence suggests that sex may significantly influence weight loss outcomes with GLP-1 RAs, highlighting the need to consider sex-specific factors when evaluating the efficacy and tailoring the use of semaglutide [55].
A recent meta-analysis highlighted that females generally achieve greater weight loss than males when treated with GLP-1 RAs [
Comments (0)