
Remember me
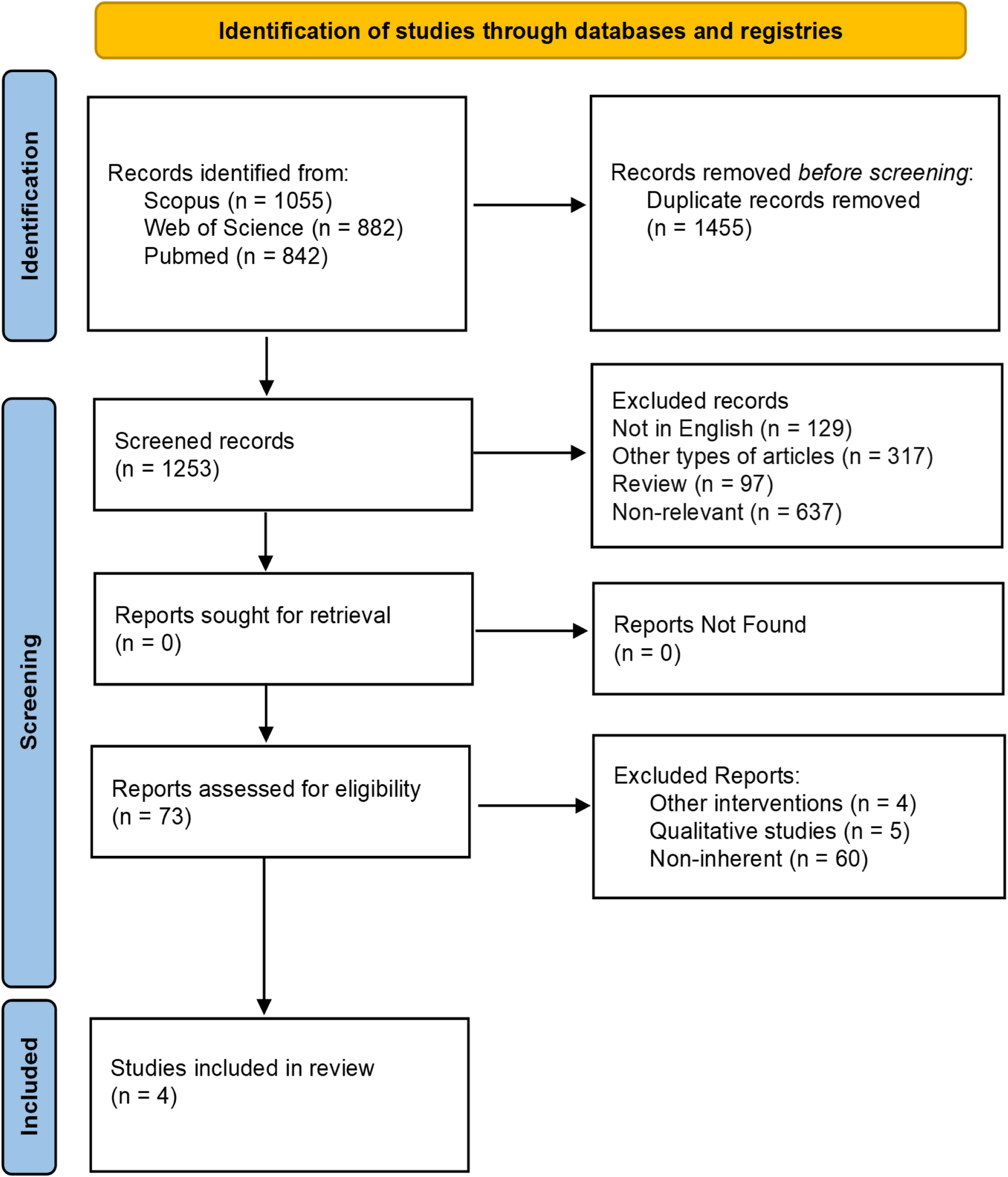
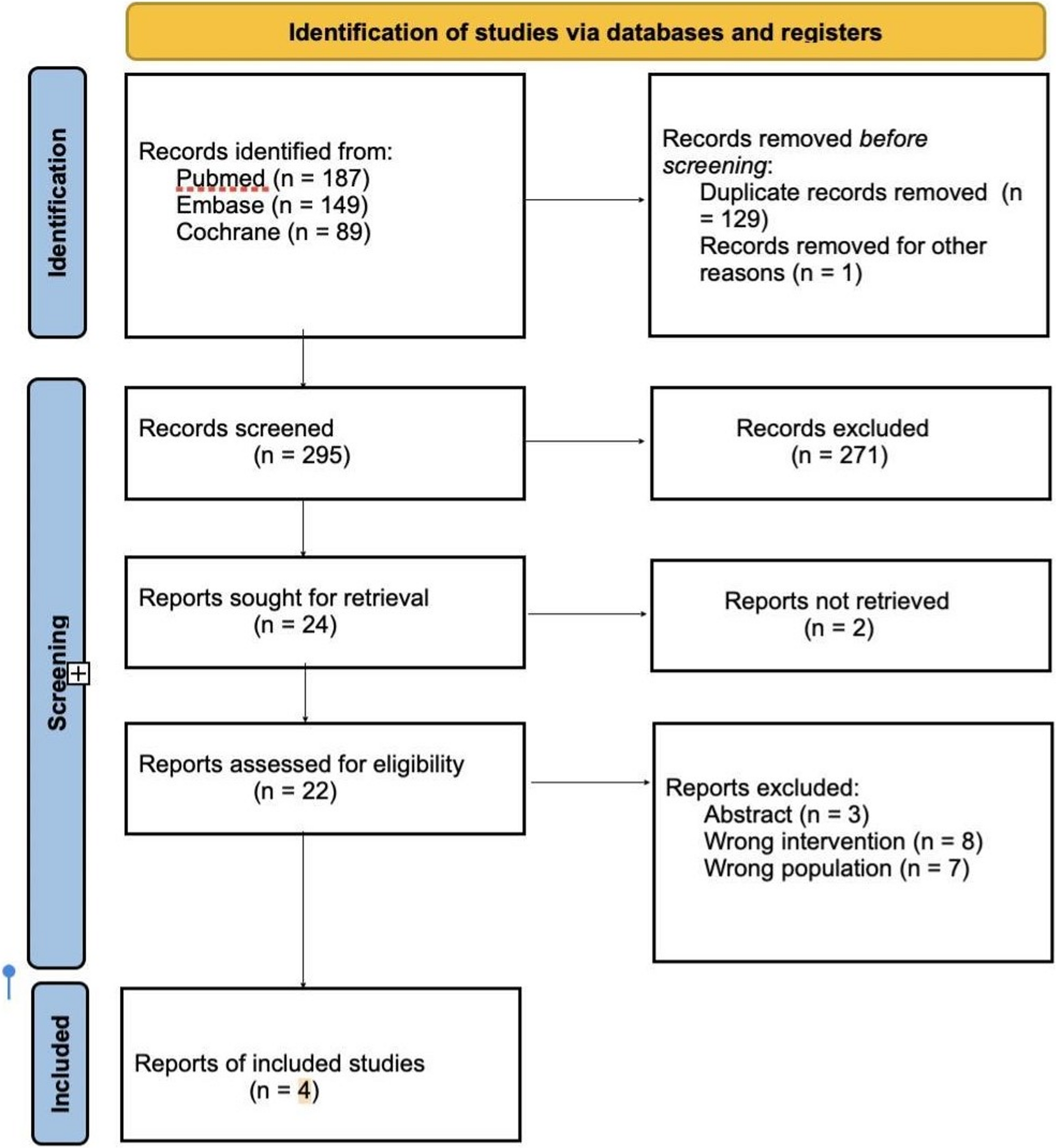
A total of 2,779 records were initially identified (Fig. 1). After removing duplicates, 1,253 records were screened. Based on inclusion and exclusion criteria, 73 full text-articles were assessed for eligibility. Of these, 69 were excluded, resulting in four articles being included in the review [28,29,30,31].
Fig. 1
Flowchart of the search strategy according to PRISMA 2020 guidelines
Studies FeaturesThe characteristics of the four included studies are summarized in Table 1, which presents three randomized controlled trials (RCTs) and one quasi-experimental study.
Table 1 Characteristics of the studies includedGarcía-Rodríguez et al. [28] included 66 patients (46 women and 20 men), evenly divided between control and intervention groups, with reported average ages of 39 and 42 years, respectively. Krishnasamy et al. [29] included 88 participants (77 women and 11 men), also equally divided, with a mean age of 38.04 years. Little et al. [30] involved 818 participants, allocated to three groups: a control group (279 patients), an intervention group with dual-meetings (269 patients), and an intervention group with telematic support (270 patients), with mean ages of 52.69, 53.70, and 54.74 years, respectively. Palmeira et al. [31] included 101 women (50 control and 51 in the intervention group), with an average age of 47.8 years (47.5 control, 48.1 intervention).
Follow-up periods varied: García-Rodríguez et al. [28] and Palmeira et al. [31] followed participants for 3 months, Krishnasamy et al. [29] for 16 weeks, and Little et al. [30] for 12 months. While Palmeira et al. [31] focused on weight and BMI reduction in a Brazilian female population, Little et al. [30] examined weight variation in English patients, and García-Rodríguez et al. [28] and Krishnasamy et al. [29] investigated weight and BMI changes in mixed-gender groups. The latter [29] recruited patients from urban areas of Puducherry, while the former [28] from Tenerife.
Quality AssessmentIn analysing the methodological quality of the included studies using the Downs and Black checklist, it was observed that all four articles achieved a moderate score. Specifically, García-Rodríguez et al. scored 16, Krishnasamy et al. scored 20, Little et al. scored 23, and Palmeira et al. scored 22 (Table 2) [28,29,30,31].
Table 2 Qualitative analysisTelemedicine Nursing InterventionThe four studies implemented various telemedicine nursing interventions (Table 1), including phone sessions, video meetings, web-based solutions, and hybrid programs that combined different technologies. A common approach across studies was the use of web-based interventions, involving emails and websites accessible to both patients and nurses. Additionally, all studies featured phone-based interventions, such as SMS and telephone coaching, with phone calls representing the primary telemedicine method used.
García-Rodríguez et al. [28] based their intervention on phone calls and emails, supplemented by a web portal providing infographics, videos, and links to relevant resources. The control group received standard nursing care from family care units.
In the study by Krishnasamy et al. [29], the intervention group received counselling and support through both telematic and in-person modalities provided by nurses. These included phone calls, video calls, SMS, home visits, and the use of Fitbit band devices. Additionally, the intervention group participated in group educational sessions on healthy eating and physical activity, featuring lectures, group discussions, posters, and displays on healthy foods during the first two weeks. The control group received only nursing basic care, along with Fitbit monitoring.
Little et al. [30] implemented the POWeR + program, designed to teach cognitive-behavioural self-regulation strategies for weight management through physical activity and dietary regimen. Initially, patients could choose between a low-calorie diet or low-carbohydrate diet, with the flexibility to switch. Two intervention groups received web-based support: the POWeR + R group had remote nursing support, while the POWeR + F group followed a hybrid approach, combining in-person and remote meetings. The control group received minimal dietary counselling and biannual nurse follow-ups, supported by printable materials and an informational website.
Palmeira et al. [31] provided the intervention group with remote phone-based monitoring in addition to routine consultations, whereas the control group received only routine care.
The results from these studies, except the one of Little et al., are summarized in Table 3. García-Rodríguez et al. [28] reported significant reductions in obesity within the intervention group achieved at follow-up. In contrast, the control group experienced increases in anthropometric measures, though these were not statistically significant, except for the mean BMI. Krishnasamy et al. [29] observed significant reductions in obesity within the intervention group. By the end of the intervention, there were significant differences between the intervention and control groups across all anthropometric variables. In the study conducted by Little et al. [30], weight was the only parameter measured continuously throughout the study. In general, all three groups experienced weight loss over the 12-month period (Supplementary Table 1). Patients in the control group maintained an average weight loss of approximately 3 kg. Patients in the POWeR + F group lost an additional 2.54 kg (p < 0.001) compared to the control group, while those in the POWeR + R group lost an extra 1.97 kg (p = 0.002) at the 6-month follow-up (Supplementary Table 2). However, at the 12-month follow-up, no significant changes were observed compared to the previous measurement. Overall, patients in the POWeR + F group lost an average of 1.49 kg (p = 0.001) more than the control group, while those in the POWeR + R group had an additional weight loss of 1.27 kg (p = 0.007) (Supplementary Table 2).
Table 3 Clinical outcomes evaluated pre and post treatmentIn the study conducted by Palmeira et al., a non-statistically significant decrease in BMI, weight, and WC in the intervention group was observed (Table 3). In contrast, the control group reported an increase in all variables, with only mean weight being statistically significant. However, it should also be noted that there was a loss of some participants in both groups during the follow-up.
Meta-AnalysisThe meta-analysis of weight includes 1012 patients, of whom 431 were in the intervention group. Initially, 1352 patients were enrolled in the pre-evaluation, but only those who completed the intervention were considered in the analysis. The total number of patients included in the meta-analyses of BMI and WC was 255, with 128 patients in the intervention group and 127 in the control group.
WeightFor measuring the impact of the protocols on weight loss, we first considered a model where all arms of the intervention of Little et al. [30] were included, as they were two independent, different treatments. The estimated common effect, using the classical two-level model, is -2.59 kg, supporting the effectiveness of the intervention in promoting weight loss. The 95% CI associated with the point estimate is [-3.09, -2.08]. The hypothesis of no difference between the treatment and the control groups is rejected both using standard methods (p < 0.001) and when considering correction methods for small study number (p = 0.001). The estimated variability due to between-study heterogeneity is 44% of the total variability (95% CI between 0 and 94.87), while the estimate of the variance between studies is 0.14, corresponding to standard deviation between the studies equal to ?=0.368 kg with 95% confidence interval in (0, 1.178). The Cochrane statistics test for heterogeneity results equal to Q (df = 3) = 4.987, p = 0.173. These results suggest that there is no evidence of marked heterogeneity. The large confidence intervals for the heterogeneity estimates are due to the small number of studies. The forest plot is reported in Fig. 2.
Fig. 2
Forest plot for the effect of the protocols on weight reduction
For this outcome, we also performed some sensitivity analysis, including in the pool of studies only one arm of the study of Little et al. [30] at a time. This is because the effect measure depends on a common control group, thus the assumption of independence of the two effect sizes is not satisfied. Under the two models with 4 studies, the effects are − 2.61 kg with 95% CI [-3.24, -1.97] and − 2.70 kg, with 95% CI [-3.24, -2.15], in agreement with the findings.
BMIWe fitted a two-level model considering the three available studies [28, 29, 31]. The estimated loss in BMI score obtained by the meta-analytic model was 1.05 kg/m2 (95% CI [-1.50, -0.60]). This result confirms that overall, the telenursing intervention reduced the BMI over that of patients in the treatment group. The p-value for the hypothesis of no difference of the two arms is < 0.001, which leads us to reject this hypothesis at the usual level. Using the Skovgaard method, for controlling the small number of studies, a p-value equal to 0.0338 was obtained, confirming the evidence of improvement. The \(\:^=\:67.07\:\%\) with 95% CI \(\:\left[0.00\%,\:99.10\%\right]\) indicates substantial heterogeneity between the studies’ estimates. The estimated value of \(\:^=0.1\), corresponding in the standard deviation scale to 0.32 points of BMI with 95% CI in [0, 2.36], suggests that the between study heterogeneity is in absolute terms negligible. The uncertainty around this estimate is due to the small number of studies. Although the decision to use a random-effects model was made a priori, the Cochran statistic supports this choice, Q (df = 2) = 6.392, p = 0.041. It is also worth noting that while the confidence intervals for the \(\:^\)and \(\:^\) statistics include values close to zero, these numbers are small but not exactly zero. The forest plot is reported in Fig. 3.
Fig. 3
Forest plot for the effect of the protocols on BMI reduction
Waist CircumferenceA two-level meta-analytic model was considered using data on the effect of the protocol on WC [28, 29, 31]. The model revealed an absence of heterogeneity among the studies, (\(\:^\)=0 and \(\:^\)=0, confidence intervals equal to the null set; Cochrane statistics Q (df = 2) = 0.034 with p = 0.983). Thus, a fixed effect model was fitted to the data. The meta-analysis yielded an estimated reduction in WC of -2.52 cm (95% CI: [-2.96, -2.09]). The hypothesis of no difference in WC between the two groups was rejected at the conventional significance level (p < 0.001). The p-value obtained with the Skovgaard method, which adjusts for the small number of studies, was 0.0121, confirming the significance of the intervention. Fig. 4 presents a forest plot for visualizing these results.
Fig. 4
Forest plot for the effect of the protocols on waist circumference
Comments (0)