
Remember me
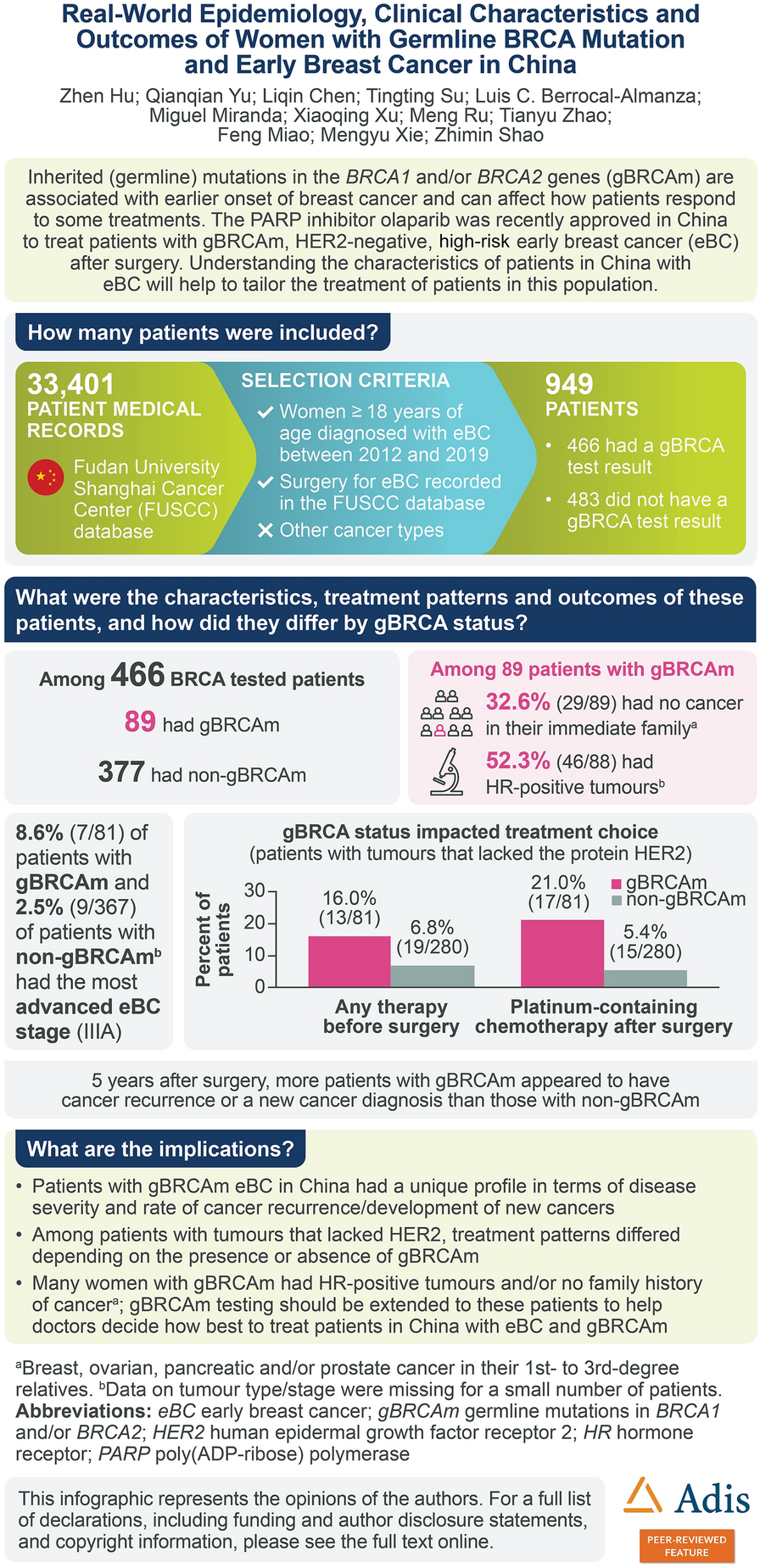

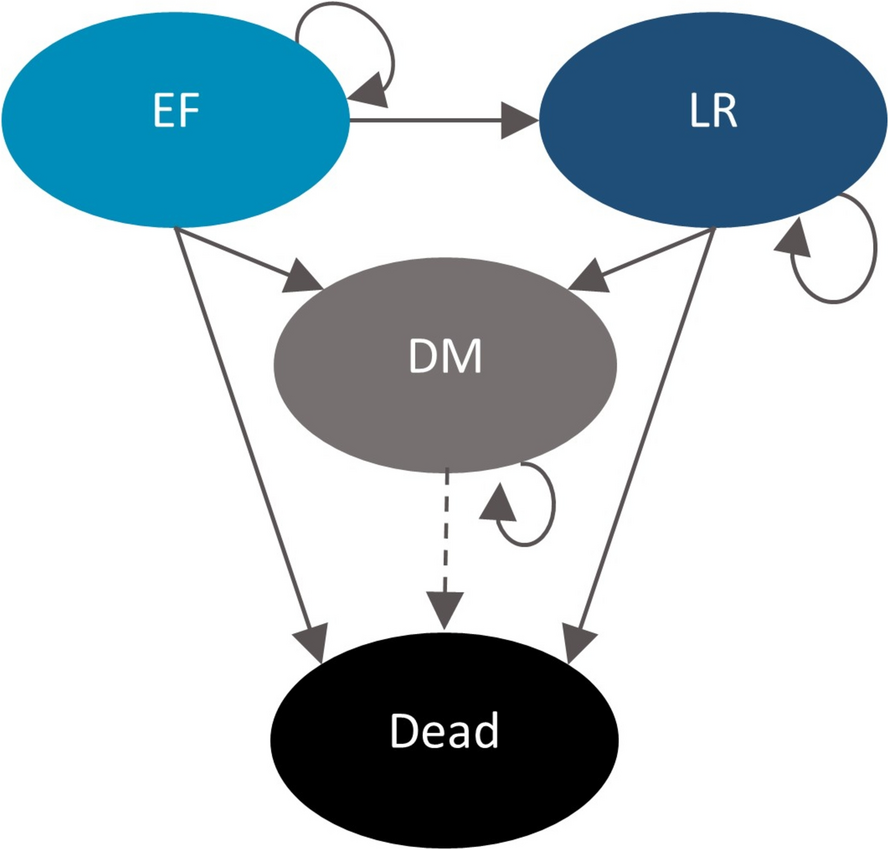
A semi-Markov cohort model (Fig. 1) was developed using Microsoft Excel to estimate and compare the economic and health outcomes of patients with resectable stage IB-IIIA nmNSCLC [5] treated with neoadjuvant nivolumab + PDC and other relevant treatment options used in the UK. The Markovian approach, which is well suited to capturing recurrent risks over time, fits well to nmNSCLC, where patients are at ongoing risk of disease progression. Further, unlike the partitioned survival analyses that are typically used in later-stage oncology models, a Markovian approach supports the incorporation of additional data sources to estimate post-progression survival, which can be particularly useful given that OS matures quite slowly in early-stage oncology.
Fig. 1
This diagram illustrates patient flow through the model. Possible state transitions are indicated using the arrows. The dotted line from DM to death represents the ‘one-off’ approach; these patients are not explicitly tracked in the model although their survival, quality of life, and cost outcomes are considered in the model outputs. DM distant metastasis, EF event-free, LR locoregional recurrence
Because the model was ultimately designed to support the NICE submission for nivolumab + PDC as neoadjuvant treatment of resectable nmNSCLC, it was informed by previous NICE submissions available at the time of initial model development (i.e., in 2021). As there were no prior models for neoadjuvant or adjuvant NSCLC at the time of the search, the review focused on other solid-tumor cancers where surgery combined with neoadjuvant or adjuvant treatment was part of the treatment pathway. Specifically, these cancers included breast, colorectal, pancreatic, kidney, and prostate (all non-metastatic). Additionally, shortly after the search was conducted, the submission for osimertinib as adjuvant treatment of fully resected epidermal growth factor receptor (EGFR) mutation-positive nmNSCLC became available; it was also considered when conceptualising the model design.
In total, seven submissions were reviewed (see supplementary Table 11). Every model reviewed adopted a Markov approach; all but one included more than one post-progression health state. In four out of seven models, patients could experience more than one type of progression from the initial health state, and in six out of seven models, multiple health states in the metastatic setting allowed for explicit tracking of metastatic survival, costs, and other outcomes.
The model used four mutually exclusive health states to track the disease course of patients over time: event-free (EF), locoregional recurrence (LR), distant metastasis (DM), and death. These health states were designed to capture the natural history of resectable nmNSCLC and the key endpoints of the CheckMate-816 trial; the use of more than one post-progression health state was also broadly supported by the HTA review described above. Distinguishing between LR and DM allows the model to explicitly consider the differences in cost and health outcomes between progression types. The model adopted a 3-week cycle length (aligned with the cycle length for neoadjuvant nivolumab and most PDCs) and in the base case assessed results over a lifetime time horizon, defined as 35 years, when less than 1% of patients were predicted to be alive for all model comparators. EF was defined as time without recurrence or death. The patients’ initial health state (EF) reflects the status of the patients enrolled in the CheckMate-816 study. From the EF health state, patients may progress to the LR or DM health states. Patients in the LR health state may experience further progression and transition to the DM health state. Patients could die in any health state. Those with LR could receive any combination of PDC, radiotherapy, and salvage surgery or no treatment at all. Patients in the DM health state were assigned to a distribution of treatments reflecting first-line metastatic NSCLC treatment patterns in the UK (Supplementary Table 3). Notably, if patients’ disease progressed within 6 months of completing the neoadjuvant nivolumab regimen (roughly 15% of patients in CheckMate-816) then retreatment with an immuno-oncology (IO) agent was not allowed, in line with “Blueteq” prescription guidelines for metastatic NSCLC treatments in the UK.
To avoid multiple distant metastatic health states, the DM health state was programmed as an absorbing health state with 'one-off' outcomes applied to patients with new metastases in the economic model (patients who enter DM from EF or LR health states) on the basis of prior first-line metastatic NSCLC NICE appraisals. In other words, DM outcomes are not explicitly calculated in our model but instead leverage outputs from existing economic models, similar to an approach used to support the NICE submission for dabrafenib + trametinib in completely resected adjuvant melanoma [9]. One-off outcomes were applied at the time of entry to the DM state and comprised estimated costs, life-years (LYs), and quality-adjusted life-years (QALYs) from the time of DM through death.
The transition rates from the EF health state to progression health states (LR and DM) were specific to each comparator. Secondary progressions and mortality (i.e., transitions from LR to DM and from each health state to death) were assumed to be the same across comparators.
A half-cycle correction was applied to relevant costs and all model utilities. All outcomes were discounted by 3.5% per annum in the base case, consistent with the NICE reference case [10].
Model outcomes included costs (total and by category), LYs, and QALYs. Based on these outcomes, incremental cost-effectiveness ratios (ICERs) per LY and per QALY were calculated between neoadjuvant nivolumab + PDC and other comparators.
Intervention and ComparatorsThe intervention of interest in the model was neoadjuvant nivolumab + PDC. The model included neoadjuvant chemoradiotherapy (CRT), adjuvant PDC, and surgery only as comparators, in alignment with the final scope issued by NICE [11]. These are also aligned with the final scope for the analyses submitted to the SMC and NCPE. Although neoadjuvant PDC was the comparator in CheckMate-816 and served as an anchor to inform indirect comparisons of neoadjuvant nivolumab + PDC to other treatment strategies for nmNSCLC, it is outside the final scope issued by NICE and was therefore not included in the cost-effectiveness analysis.
All modelled comparators and interventions are defined by the decision made at time zero in the model. Therefore, patients who receive neoadjuvant treatment strategies may receive subsequent adjuvant treatment after surgery. This aligns with the design of CheckMate-816, in which adjuvant treatment could be given at the discretion of the treating physician.
The dose and administration schedule for neoadjuvant nivolumab + PDC followed that of the CheckMate-816 study. Patients could receive up to three cycles of nivolumab (360 mg per dose); each cycle of nivolumab was administered in combination with a cycle of PDC.
Comparator dosing and administration schedules followed trial schedules and guidelines. Specifically, patients given the neoadjuvant CRT comparator received radiotherapy (45 Gy in 3 weeks) in addition to three cycles of neoadjuvant PDC. Patients given the adjuvant PDC comparator immediately received surgical resection followed by three cycles of adjuvant PDC. The distribution of treatment options for the neoadjuvant PDC component of neoadjuvant CRT and adjuvant PDC were assumed to be equivalent to those in the control arm of CheckMate-816. Patients given the surgery-only comparator immediately received surgical resection and did not receive any adjuvant PDC.
Model InputsTransition ProbabilitiesThe estimates of the time-dependent transition probabilities characterising the time to LR (TTLR) and time to progression (TTP) outcomes as well as the time to death from each health state were based on data collected from the CheckMate-816 trial and an indirect treatment comparison.
Standard parametric survival analyses using the exponential, Weibull, Gompertz, log-logistic, log-normal, gamma, and generalised gamma distributions were conducted to extrapolate the TTLR and TTP outcomes for both treatment arms from the CheckMate-816 trial over a lifetime time horizon (Supplementary Fig. 1). Extrapolations used in the base-case analysis were chosen according to visual and statistical (i.e., Akaike information criterion and Bayesian information criterion) assessments, feedback from clinical experts, and extensive external validation using the published literature, following guidance from NICE Technical Support Document 14 [12]. Flexible spline models were fitted and assessed in cases in which none of the standard parametric extrapolations provided reasonable fit to the data. Standard parametric analyses were conducted using the flexsurv package in R, and the STPM2 package in STATA was used to fit splines.
TTP, TTLR, and TTDMTTP and TTLR were both jointly fitted with treatment as a predictor to the neoadjuvant nivolumab + PDC and neoadjuvant PDC arms on the basis of evidence suggesting that the proportional hazards (PH) assumption holds. Specifically, the log–log plot, Schoenfeld residuals plot, and QQ-plots all support the PH assumption; these are included in the Supplementary Material (Supplementary Fig. 10 and Supplementary Fig. 11). Any qualifying event (i.e., death or, in the case of TTLR, non-locoregional progression) was treated as a censoring event to account for competing risks in the model. The log-normal distribution was determined to be the best fit for both TTP and TTLR outcomes on the basis of a statistical assessment and validation with external data and clinical experts.
The immaturity of the time to DM (TTDM) data from the first interim analysis of the CheckMate-816 trial prevented the development of reliable parametric fittings and long-term extrapolations of this outcome. Therefore, TTDM was estimated as the difference in the hazard rates of TTP and TTLR extrapolations; this approach was validated by clinical experts in an advisory board.
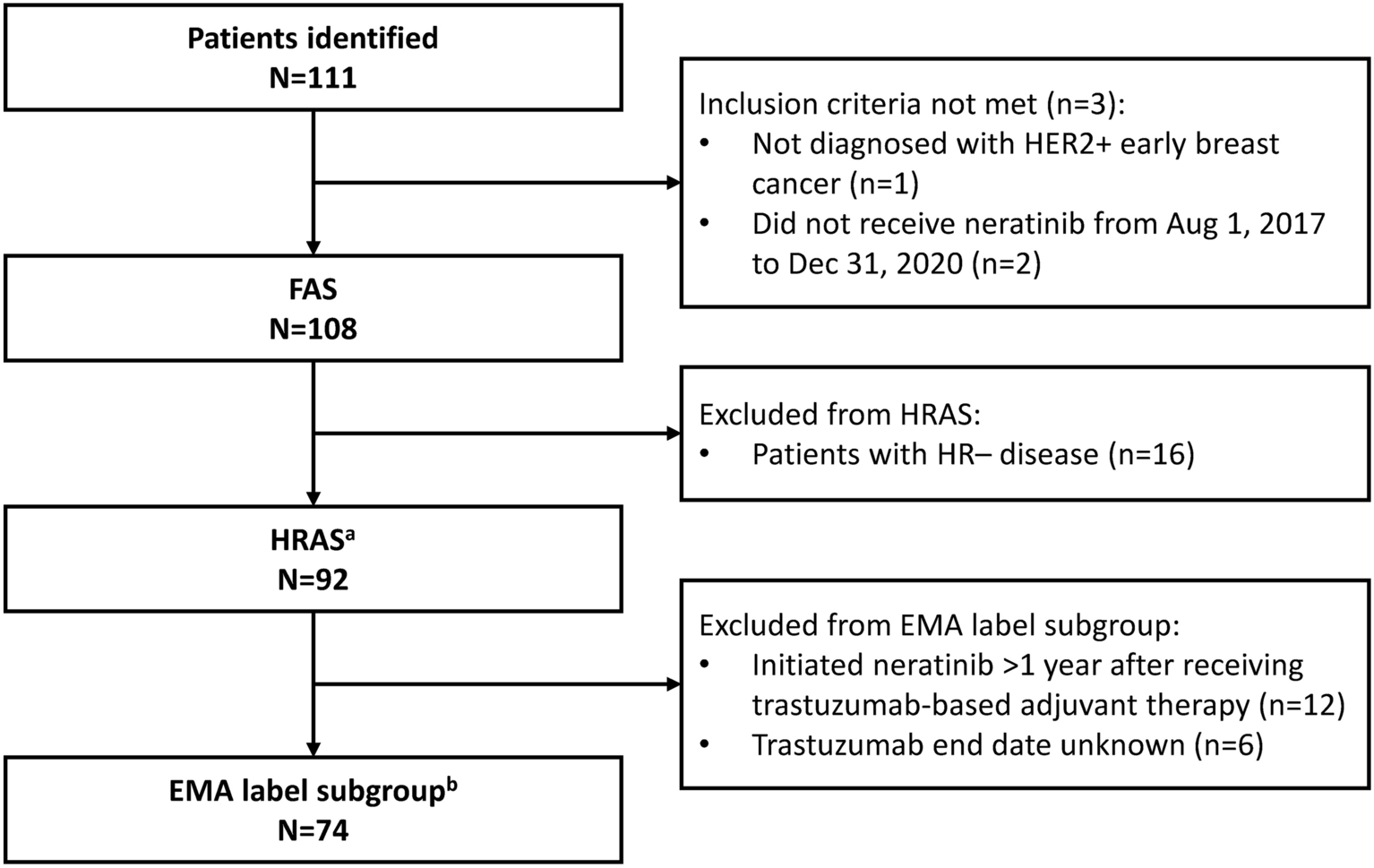
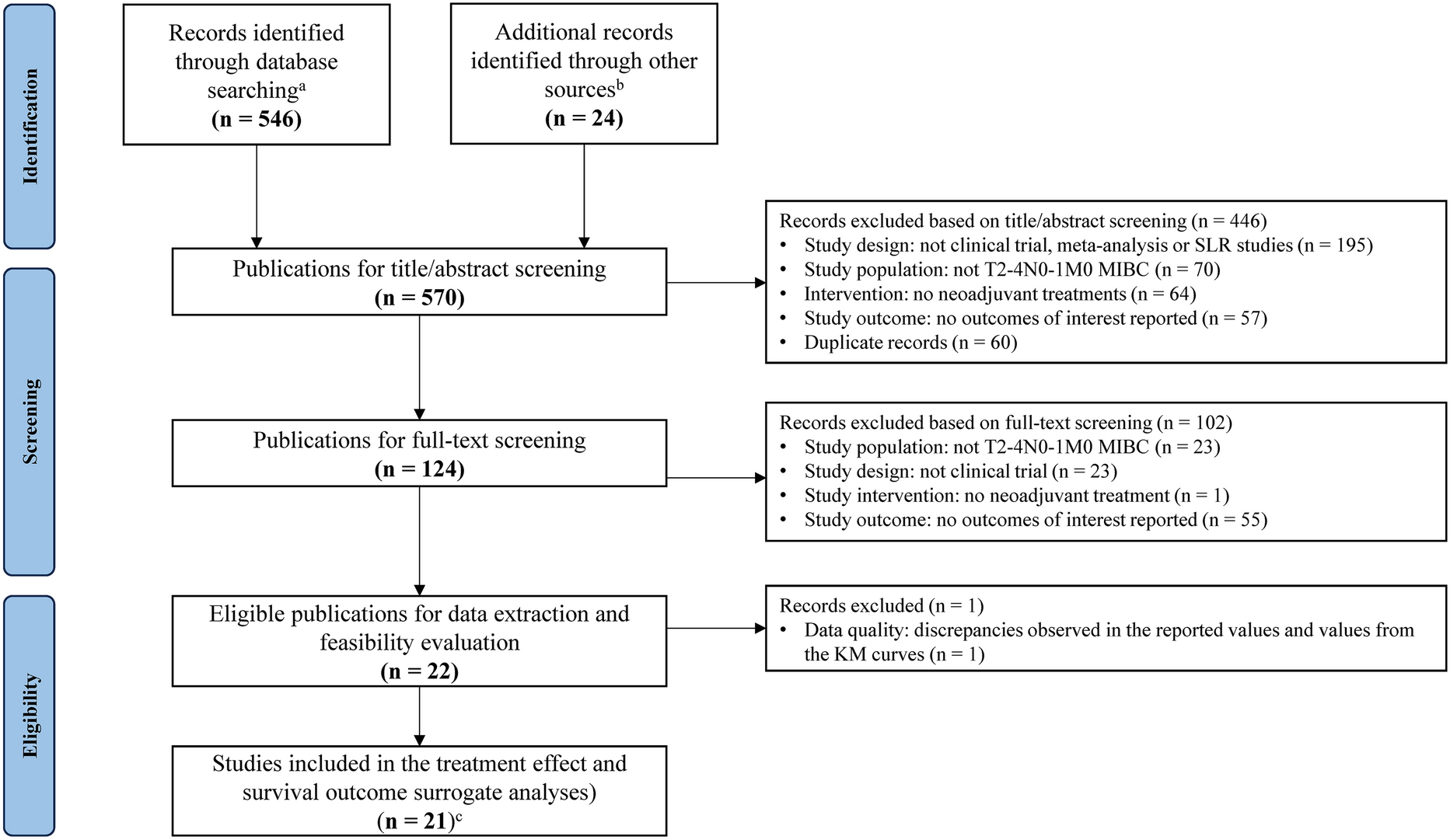
Hazard ratios obtained from a network meta-analysis (NMA) [13] were applied to the neoadjuvant PDC extrapolations of TTLR and TTDM to estimate transition probabilities for neoadjuvant CRT, adjuvant PDC, and surgery only. While published meta-analysis by Girard et al. does not include the specific HRs for TTLR and TTDM, these are derived from the same SLR and presented in Table 1. To reflect (a) the curative intent of treatment for resectable nmNSCLC [18], (b) input from clinical experts, and (c) the inclusion of a cure assumption in prior nmNSCLC models submitted to NICE [17, 19], the transitions from the EF state were adjusted to account for the potential for cure. Cured patients were no longer considered at risk of disease progression and were no longer subject to disease-specific mortality. The model assumed, on the basis of clinical feedback, that cure began at year 5. The proportion of cured patients increased linearly from years 5 to 7 until 95% of the patients in the EF state remained cured. The time to event curves used to estimate TTLR and TTDM for all comparators are shown in Figs. 2 and 3, respectively.
Table 1 Key model inputsFig. 2
This plot shows the survival curves used to estimate transition probabilities governing patient movement from the event-free to the locoregional recurrence state. The solid lines indicate Kaplan–Meier survival data, while the dotted lines show the parametric extrapolations. CRT chemoradiotherapy, KM Kaplan–Meier, PDC platinum doublet chemotherapy
Fig. 3
This plot shows the survival curves used to estimate transition probabilities governing patient movement from the event-free to the distant metastasis state. CRT chemoradiotherapy, PDC platinum doublet chemotherapy
LR to DM TransitionThe CheckMate-816 trial captured only the first progression event; hence, no data informing the time to DM progression from LR were available from the trial. Thus, we sought external sources to inform this input. In the base-case analysis, an average estimate of 20% of patients per year was considered on the basis of advice from clinical experts. An estimate of 7.7% of patients per year, estimated from findings of the LuCaBIS study [20], was tested in a scenario analysis.
DM Health StateThe one-off outcomes of patients entering the DM health state were intended to be informed by the NICE external assessment group-preferred model results (i.e., estimated LYs, QALYs, and total costs) from NICE Technology Appraisals associated with metastatic NSCLC treatments. However, the required results were consistently redacted in the published NICE documents. Thus, outcomes in the DM state were based instead on external assessment group-preferred estimates obtained from a metastatic NSCLC model previously developed by BMS (TA724; “Nivolumab with ipilimumab and chemotherapy for untreated metastatic NSCLC”) [17]. However, two relevant subsequent treatments were not included in this submission: pembrolizumab + carboplatin + paclitaxel for squamous NSCLC, and atezolizumab monotherapy. DM state inputs for the former were obtained from the nivolumab + ipilimumab submission for untreated advanced NSCLC to the SMC [19], and DM state inputs for the latter were assumed to be equal to those for pembrolizumab monotherapy per TA724 [17]. Finally, expert feedback suggested that 25% of patients eligible for first-line metastatic NSCLC treatment receive best supportive care (BSC; i.e., palliative care) only. On the basis of clinical expert input, an HR of 0.9 was applied to PDC outcomes in metastatic NSCLC to generate the LY and QALY input values for BSC. BSC was assumed to incur no cost.
BMS market research data were used to estimate the percentage of patients in the DM state receiving each treatment option. For patients who received neoadjuvant nivolumab + PDC, the distribution of treatments in DM was adjusted to consider England NHS guidance as described in “Blueteq” prescribing information for metastatic NSCLC treatments in the UK. Specifically, this guidance recommended that patients who had progressed on or within 6 months of progression with an IO agent should not receive further IO treatment. This translated to 15.1% of patients who had received neoadjuvant nivolumab + PDC based on CheckMate-816 data in the base-case analysis. The total LY, QALY, and costs applied for patients entering the DM state are included in Table 1. The disaggregated inputs are shown in the Supplementary Material.
MortalityAn analysis of CheckMate-816 data was conducted to estimate mortality for EF patients and patients who had LR. Differences in treatment-specific mortality among patients based on these immature estimates were not statistically significant. Therefore, data from both treatment arms of the CheckMate-816 trial were pooled, and parametric survival analyses of mortality in EF and LR were conducted. Compared with treatment-specific analyses, pooling patients in both treatment arms generated more observations, increasing the reliability of mortality extrapolations. A notable implication of this approach in terms of the model outcome is that any LY benefit observed is implicitly linked to the time patients spend in the EF state.
In the model base case, extrapolations of mortality in the EF and LR states were modeled using an exponential distribution and a spline model with three knots, respectively, on the basis of statistical assessment and validation via comparison against survival estimates from the placebo arm of the PACIFIC study [21] and for stage IIIA and IIIB from the IASLC database [22]. To ensure the plausibility of the extrapolations, the probability of death was not allowed to fall below the estimated rate in the general age- and sex-matched population (obtained from UK life tables) at any time [23]. Selected base-case extrapolations are depicted in the Supplementary Material, as well as diagnostic plots assessing the PH and AFT assumptions. The patient-level data from the CheckMate-816 trial used to inform the transition from LR to death incorporate the use of treatment for LR and any related impact on progression and survival. Therefore, no explicit survival adjustments related to subsequent treatment were applied to LR to death transitions.
SafetyThe model considered the impact of grade 3 or 4 adverse events (AEs) occurring in at least 5% of the study participants in any comparator arm. AE data were derived from the CheckMate-816 trial, except for data pertaining to AEs associated with adjuvant PDC, which were collected by conducting a systematic literature review (SLR). AEs for neoadjuvant CRT were assumed to be equal to those of neoadjuvant PDC from CheckMate-816; this constitutes a conservative assumption given that some additional AEs related to radiotherapy could be expected. The percentages of patients experiencing each AE are presented in Supplementary Table 5. Notably, fewer patients receiving neoadjuvant nivolumab + PDC experienced grade 3 or 4 treatment-related AEs compared to neoadjuvant chemotherapy alone in CheckMate-816.
UtilitiesHealth utility values stratified by health state (but not by treatment) were determined by applying UK tariffs to EQ-5D-3L health questionnaire data from the CheckMate-816 trial.
The estimated EF utility among patients included in the CheckMate-816 trial was higher than age-matched UK population norms. This was considered clinically implausible; therefore, the modeled EF utility value was decreased to be equal to the UK population norm of 0.833, as reported by Hernández Alava et al. [24]. The LR utility estimate obtained from the CheckMate-816 trial (and the upper/lower 95% CIs) was decreased by the same amount as the utilities in the EF state. In addition to the health-state utilities described above, a one-off QALY decrement was applied to patients in the first model cycle to reflect the impact of AEs on patient quality of life (QoL) adjusted for duration of impact. Disutilities are were calculated from the AE profile for each comparator and data collected in Nafees et al. [25].
The health utility values and QALY decrements related to AE are presented in Table 1. Details on the disutility for each AE are included in the Supplementary Material. The utility values were adjusted during the simulation to account for decreasing QoL among patients as they age, according to ISPOR Good Practices recommendations [26].
CostsAll costs in the base-case analyses reflect the English NHS perspective but are broadly representative of costs in the UK and Ireland (UK&I). The costs in the model are identical to those used in NICE submission TA876 [11]; therefore, they are expressed in 2022 British pounds (GBP). Any costs retrieved from prior years were inflated to 2022 GBP. The detailed cost inputs are presented in the Supplementary Material.
The model considered the costs of drug acquisition, drug administration, radiotherapy, surgery, subsequent adjuvant treatment (for neoadjuvant nivolumab + PDC and neoadjuvant CRT), treatment for LR disease, treatment for DM disease, healthcare resource use (HCRU) and monitoring, AE management, and end-of-life care.
The overall cost of neoadjuvant treatment was based on the distribution of PDC treatment regimens given in the CheckMate-816 trial (Supplementary Table 3) and relevant unit costs. PDC regimens in adjuvant PDC and neoadjuvant CRT reflected input from UK clinicians.
The costs of surgery reflected relevant unit costs along with the distribution of procedures received and percentage of patients receiving surgery. For all treatments, the distribution of surgery types was based on the outcomes of CheckMate-816. Neoadjuvant CRT, adjuvant PDC, and surgery only were assumed to have the same distribution as neoadjuvant PDC in the CheckMate-816 study. The percentage of patients receiving surgery was based on CheckMate-816 for neoadjuvant nivolumab + PDC and neoadjuvant CRT, and neoadjuvant CRT was assumed to be equal to neoadjuvant PDC in CheckMate-816. The percentage of patients receiving surgery in the adjuvant PDC and surgery-only comparators was based on the NATCH study [16].
For patients who initially received neoadjuvant treatment and then continued to receive adjuvant treatment after surgery, the costs applied account for the proportion of patients receiving adjuvant treatment, the type of treatment received, and the number of treatment cycles received, which were all informed by data from the CheckMate-816 trial (Table 1 and Supplementary Table 5).
All drug costs in the model were based on prices retrieved from the drugs and pharmaceutical electronic market information tool (eMIT) or, if unavailable, the Monthly Index of Medical Specialities (MIMS) drug database. The surgery, HCRU, and monitoring inputs were based on the National Schedule of NHS Costs, Year 2019–2020, inflated to 2021/2022 values [15] (Supplementary Table 4 and Supplementary Table 8).
AE management costs were applied as a one-off total at the time of treatment initiation, and the cost of each event was based on data obtained from the schedule of NHS costs.
The end-of-life costs applied in the model were based on the costs reported in Hoverman et al. [27] and account for the type of end-of-life care (hospital, hospice, or home).
ValidationThe model and the selection of base-case inputs were thoroughly validated.
First, the face validity of the model’s structure, inputs, assumptions, and survival projections were confirmed by a team of clinicians in an advisory board held in April 2022.
Second, the model was subjected to rigorous technical validation to ensure that it was free from any logic or computational errors. Two rounds of validation were undertaken, and both were conducted by programmers who had not otherwise been previously involved in model development. The second round of validation identified and resolved one error, ensuring that the model is technically sound.
Finally, the long-term survival outcomes for the neoadjuvant PDC arm were compared with external sources with large sample sizes and long-term follow-up. Specifically, those sources were a patient-level meta-analysis that pooled outcomes from large randomised clinical trials conducted between 1991 and 2017 (unpublished observations), and Goldstraw et al. [22], which considered a database of 94,708 cases of NSCLC from 35 sources across 16 countries, with approximately 20,000 patients with stage IB-IIIA NSCLC. The long-term OS outcomes for neoadjuvant PDC estimated in the model were found to be similar to those reported in external sources. Notably, the model was somewhat more optimistic than the external sources in early years but then aligned closely to external sources in the long-term. The model produced slightly more optimistic survival results for neoadjuvant PDC compared with those observed in the trial, so any resulting bias was not in favor of neoadjuvant nivolumab + PDC.
More details, including a graphical comparison of the model and external data OS curves, are provided in the Supplementary Material, External Validation.
Model AnalysesMirroring the NICE guidelines that were used to inform the submission, we present all results as pairwise comparisons given that nivolumab + PDC is expected to replace the individual comparators.
In addition to the deterministic base-case analysis, we also conducted multiple sensitivity and scenario analyses.
A one-way, deterministic sensitivity analysis (DSA) was performed using the 95% CIs of each parameter. For those parameters lacking a published or known CI, values reflecting the base-case input ± 20% were tested.
A probabilistic sensitivity analysis (PSA) with 1000 iterations was also performed to assess the impact of joint uncertainty in all parameters. The parameter samples in each PSA iteration were obtained by randomly sampling a distribution of values reflecting the parameter mean and 95% CIs. If 95% CIs were unavailable, standard errors were assumed to be 20% of the mean values, and the CIs were derived accordingly. The distributions used for varying parameters in the PSA are summarised in Supplementary Table 9.
Non-parametric uncertainty was assessed in scenario analyses using alternative selection of parametric extrapolations, alternative cure assumptions, and a 12-month retreatment restriction for IO during metastatic disease.
Comments (0)