
Remember me


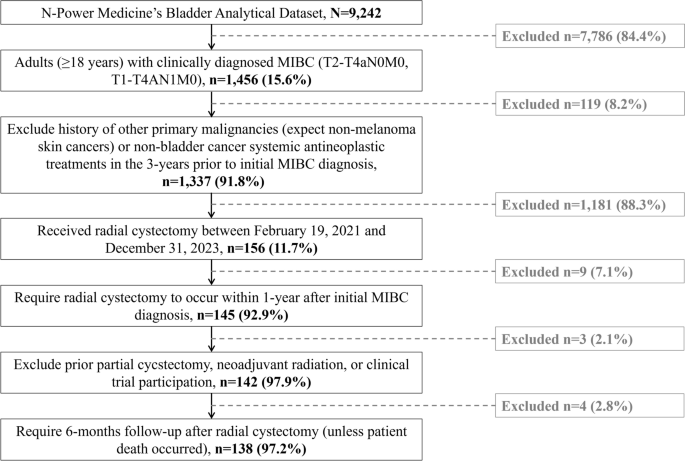





The PRISMA flow diagram (Fig. 1) provides an overview of the literature search process. After removing duplicates using Covidence software, the search across various databases yielded 1317 articles. A manual search of relevant review articles and reference lists identified an additional article. The remaining articles underwent title and abstract screening, excluding 238 articles deemed irrelevant to the research questions. This left 493 articles for full-text review to assess eligibility. Of these, 238 articles were excluded for the reasons outlined in Fig. 1. Ultimately, 17 studies were included in the systematic review for qualitative synthesis.
Fig. 1
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram of the study selection process
Overview of Included StudiesTable 1 presents a comprehensive overview of the 17 included studies [17, 31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46], which represent a diverse geographical distribution, including Europe, Asia, and North America. The studies employed various designs, including randomized controlled trials (RCTs), cohort studies, cross-sectional studies, and mixed-method approaches. A total of 20,045 patients were recruited in the 17 included studies. Individual study sample sizes varied significantly, ranging from 6 participants in qualitative investigations [32] to 17,774 in large nationwide cohort studies [33]. The participants’ ages ranged widely, with mean values primarily between 63 and 74 years across studies. Most studies reported mean ages of around 70 years, with some indicating a median age of approximately 70 years (interquartile range [IQR]: 63–80). The age range spanned from 37 years to 94 years. A subset of studies categorized participants, showing that the majority were aged ≥ 70 years, while smaller proportions fell below this age threshold. The majority of participants across studies were male, with representation ranging from 55% in one study [37] to 90.1% in another study. Some studies reported a predominantly male cohort (e.g., ≥ 86% male) [35, 41], while others included more limited proportions of female participants, ranging from 9.9% to 24% [33, 41]. Although the lower end of this range reflects underrepresentation, proportions around 20–25% are consistent with the known epidemiology of NMIBC. In one study, all participants were male [39].
Table 1 Detailed characteristics of studies included in the reviewTreatment Modalities and Study FocusThe studies primarily focused on intravesical therapies, with the majority emphasizing BCG treatment. Although some included chemotherapy instillations, BCG remained the central therapy. For BCG, the treatment protocol commonly involved a 6-week induction phase followed by a maintenance phase. Maintenance therapy schedules and adherence were key areas of comparison, with limited studies [42, 43] focusing on optimizing treatment schedules to balance efficacy and tolerability. Maintenance schedules varied, ranging from tri-weekly to monthly instillations, typically lasting between 1 year and 3 years, depending on the protocol used. The protocols generally adhered to international guidelines such as the National Comprehensive Cancer Network (NCCN), AUA, and EAU [27, 47, 48]. In addition to BCG, chemotherapy agents such as mitomycin C (MMC) and gemcitabine were also used in certain cases. A single instillation of MMC is commonly administered immediately after TURBT to reduce recurrence risk. Alternative intravesical chemotherapy regimens, including gemcitabine, mitomycin, or a combination of gemcitabine and docetaxel, are being investigated as potential replacements for BCG, particularly in response to BCG shortages or contraindications. Notably, the combination of gemcitabine and docetaxel is currently being studied in the BRIDGE trial (reg. no. ECOG-ACRIN EA8212), a phase 3 randomized trial evaluating its effectiveness compared with BCG in BCG-naïve patients with high-grade NMIBC [11].
Several studies also described reduced-dose regimens or alternative strategies during BCG shortages, which influenced treatment administration.
Frequency and DurationThe induction phase generally involved weekly BCG instillations for 6–8 weeks, aimed at eradicating cancerous cells and priming the bladder for maintenance. After induction, patients typically underwent maintenance therapy, which often consisted of three weekly instillations at 3, 6, and 12 months. This schedule could vary on the basis of protocol. For example, some involved 3-weekly treatments during the first year, and then every 6 months in subsequent years [46]. Limited studies also indicated that some patients experienced reduced maintenance frequency owing to toxicity or patient preference [34]. A reduced-frequency arm (e.g., 9 instillations instead of 15) was sometimes explored to assess the efficacy versus standard protocols [43].
Delivery MethodTreatment was predominantly delivered in outpatient clinic settings, often managed by nurses. Specialist Urology Nurses or Clinical Nurse Specialists typically oversaw instillation procedures and follow-up care [31]. During BCG instillations, patients were generally instructed to retain the bladder solution for 30 min to 2 h to ensure sufficient mucosal exposure. One study mentioned inpatient care in certain cases [44], particularly for initial cycles or patients with complex comorbidities.
OutcomesQuality of Life and Patient-Centered OutcomesQoL was assessed in multiple studies using validated tools such as the EORTC QLQ-C30 [35,36,37, 39, 43, 45], EORTC QLQ-NMIBC24 [37], and FACT-BL [39]. Key domains included physical functioning, emotional burden, treatment inconvenience, and symptoms scales. In studies, Gontero et al. and Koga et al. examined urinary symptoms, fatigue, and emotional distress, showing how these factors influenced patients’ patient-reported QoL outcomes [35, 36]. Frequent hospital visits, logistical challenges, and time commitment were also common complaints [40]. In one study, 60% of patients who discontinued treatment cited persistent mild discomfort affecting social life, and toxicity severity did not always correlate with treatment efficacy [41].
Adherence and Treatment ExperiencesObservational studies such as Alcorn et al. [31] and qualitative investigations such as Alcorn et al. [32] and Vo et al. [44] explored patient experiences, adherence patterns, and treatment-related challenges. Alcorn et al. reported a 90% BCG withdrawal rate, with many patients discontinuing owing to toxicity. The most frequently reported adverse effects included urinary frequency (39%), pain (31%), and cystitis (28%), as well as catheterization difficulties, which collectively contributed to high discontinuation rates [31]. These findings underscore patients’ physical challenges, which may contribute to dissatisfaction and nonadherence. Alcorn et al. found that patients aged ≥ 70 years were significantly more likely to discontinue BCG early (log-rank 17.34, p = 0.001), with 46% withdrawing within 1 year. Side effects were also significantly associated with early withdrawal (log-rank 7.27, p = 0.007) [31]. These findings emphasize the need for age-specific support strategies to help older adults tolerate therapy. Factors such as travel, wait times, and healthcare access also influenced adherence [40]. Garg et al. noted that rural patients [34] reported long commutes and urologist shortages, leading to care delays and reduced treatment confidence. BCG shortages further complicated treatment delivery, with some patients receiving alternative agents or reduced dosages [34].
Survival and Recurrence OutcomesSeveral studies assessed recurrence-free survival (RFS), progression-free survival (PFS), cancer-specific survival (CSS), radical cystectomy-free survival (RCFS), and overall survival (OS) [36, 42, 43]. Subiela et al. showed that BCG-unresponsive patients (inadequate response within 6 months of BCG therapy) had worse oncological outcomes: lower PFS (hazard ratio [HR] = 3.40, p < 0.001), lower CSS (HR = 4.42, p < 0.001), lower RCFS (HR = 3.52, p < 0.001), and no significant OS difference (p = 0.28) [42].
Koga et al. found improved RFS rate in the maintenance group (95.8% versus 74.1%), although not statistically significant (p = 0.078) [36]. The NIMBUS trial demonstrated that reduced-frequency BCG (with fewer instillations) was associated with significantly higher recurrence (42%) compared with standard-frequency arm (27%) at 1 year (HR = 1.95, p = 0.02) [43]. These results highlight potential risks in modifying standard regimens.
QoL Impact of Frequent InstillationsUrinary symptoms were commonly reported side effects across multiple studies. Gontero et al. found persistent urinary symptoms despite treatment. BCG instillations, in particular, were frequently associated with immune-mediated bladder wall irritation, leading to detrusor overactivity, cystitis, and symptoms such as urgency, frequency, and nocturia [33, 34, 39, 46]. Miyake et al. specifically noted that increased nocturia and urgency negatively affected sleep quality [39].
These symptoms significantly impacted patients’ QoL, often disrupting daily activities and emotional well-being. One study found that patients undergoing frequent or repeated intravesical instillations such as those receiving maintenance therapy or multiple TURBTs followed by further instillations experienced exacerbated urinary symptoms, leading to a fourfold increase in the use of bladder-relaxing medications and antibiotics [33].
Repeated treatments were associated with cumulative bladder irritation and chronic discomfort. One participant highlighted this burden: “If people heard my story, all they would hear is cancer, but what I went through—the chronic pain—was much worse.” Both BCG and intravesical chemotherapy (e.g., MMC) were linked to urinary frequency, urgency, and bladder discomfort, which patients described as distressing and disruptive to their routines [33, 44]. Additionally, some patients experienced technical and emotional challenges related to self-catheterization, which was sometimes required owing to urinary retention or complications following BCG treatment, not for BCG administration itself, which is typically performed by clinical staff [32]. One individual shared, “I had a problem just putting the catheter in. I have a problem with not relaxing, you know, and that’s why it doesn’t go into whatever… yes it makes you a little bit sore down there, but it just makes you a bit depressed. It’s hard to explain really” [32]. Common side effects reported by patients using self-catheterization included urinary frequency (39%), cystitis (28%), generalized pain (31%), and catheterization difficulties (20%) [31]. While not directly linked to the frequency of intravesical instillations, these experiences highlight the broader physical and psychological burdens that can accompany bladder cancer treatment, especially in those who develop complications requiring catheter use.
Severe fatigue was a prevalent side effect, affecting 52–55% of patients undergoing frequent BCG therapy [38, 46]. This fatigue was largely attributed to the combined physical strain of the treatment and its disruption of daily activities. Notably, patients undergoing maintenance therapy reported a further increase in fatigue complaints [46]. Across studies, fatigue has remained a consistent concern, with Gontero et al. documenting treatment-related fatigue [35], while Kuperus et al. identified it as a common side effect [38].
BCG instillations significantly affect the emotional well-being of patients with NMIBC, contributing to anxiety, depression, and emotional distress, especially during the maintenance phase. The repetitive nature of BCG therapy amplifies these psychological challenges [32, 34, 44, 46].
Alcorn et al. highlighted that the emotional strain of BCG treatments led to patients feeling disconnected from their bodies: “Mentally I thought, if this is what it does, I don’t think my body would take it.” This reflects the psychological toll of the treatment’s side effects [32]. Vo et al. further noted that many patients struggled with the emotional burden during the more frequent maintenance phases, with one participant saying, “It was like being stuck in a constant state of worry, unsure if the treatment would even work” [44]. Fear of death, tied to the treatment itself, was also evident. One participant expressed, “Oh dear, what if I should have them [BCG instillations], I might die from what happens from them; if I don’t have them, I might die…” [34]. This illustrates the heightened emotional distress caused by uncertainty regarding treatment outcomes.
Treatment Adherence and WithdrawalOne study found a high withdrawal rate of 90%, with only 10% of patients completing the full 3-year BCG treatment protocol [31]. Withdrawal was the most common during the induction phase, when 39% of patients stopped treatment within the first 42 days, a period marked by weekly instillations. Additionally, 46% of patients discontinued treatment within the first year [31].
The main reasons for withdrawal were treatment-related side effects, which were reported in 67% of those who discontinued. The most common side effects included urinary frequency (39%), cystitis (28%), and generalized pain (31%). Patients who experienced side effects were 5.44 times more likely to withdraw from treatment.
Older age was another significant factor, as patients aged 70 years or older were less likely to adhere to the treatment regimen compared with younger patients [31].
Patients who experienced severe side effects, such as persistent urinary symptoms, fatigue, and emotional distress, were more likely to discontinue intravesical therapy. Other contributing factors included fear of side effects, limited knowledge about their disease, lack of family or social support, and unrealistic expectations about treatment outcomes. Younger patients (ages 40–59 years) reported the highest levels of distress, often due to work-related challenges and caregiving responsibilities, although this was not directly linked to treatment discontinuation [46].
Emotional support and clear communication from healthcare providers were critical in promoting adherence. Some patients preferred written information over verbal explanations from nurses, which in certain cases was associated with earlier withdrawal from therapy. Patients frequently expressed concerns about the effectiveness of the treatment and its side effects. For example, one patient asked, “I could not retain the bladder instillation for 60 min; does this mean that the cancer will come back?” [46]. This emphasizes the importance of addressing patients’ fears and providing clear, reassuring communication throughout the treatment process.
Benefits of Reduced FrequencyInitial hypothesis suggested that reducing the frequency of BCG instillations could preserve efficacy while improving patients’ QoL by decreasing treatment burden and side effects [36]. However, the phase III NIMBUS trial, a key study in this area demonstrated that a reduced schedule of BCG instillations (standard dose but fewer administrations) resulted in significantly higher recurrence rates compared with the standard schedule [43]. The trial was halted early after interim analysis showed unacceptable inferiority in recurrence-free survival in the reduced-frequency arm [49].
Although reduced-frequency regimens were associated with fewer adverse events such as hematuria, dysuria, and fatigue, this did not consistently translate into improved overall QoL. In one study, patients reported lower symptom burden and emotional distress, with improved scores on specific QoL measures (e.g., EORTC QLQ-C30). However, other trials found no significant differences in mean QoL scores between treatment arms over time. For example, one study noted a lower incidence of urgency and general malaise in the reduced-frequency group at specific time points, but these findings did not result in a statistically significant improvement in overall QoL.
One study highlighted strong patient preferences for alternative intravesical therapy delivery, with 72% open to in-home therapy [40]. Many patients felt that it would be less disruptive (54%) and reduce anxiety (27%) [40]. However, there were also 11% of patients who expressed safety concerns, and 37% preferred the reassurance of clinic-based treatments [40].
Patients also emphasized the importance of clear communication regarding treatment expectations and potential side effects [44]. Peer support was also valued, especially for gender-specific needs, including open discussions on sexual function [44].
Results of the Quality Assessment of Included StudiesQualitative Studies (CASP Analysis)The four studies [32, 34, 37, 44] demonstrated strong methodology, with clear aims, appropriate qualitative approaches, and ethical rigor. They provided valuable insights into patient experiences and unmet needs in bladder cancer care [
Comments (0)