
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Remember me
Hemodynamic monitoring consists of the assessment of physiological variables to evaluate the performance of the cardiovascular system in ensuring effective blood flow. Among these variables, cardiac ejection parameters such as stroke volume and cardiac output are recognized as particularly relevant and are monitored routinely in clinical settings (Recco et al 2022). Hemodynamic monitoring also plays a central role in preclinical research, particularly in the fields of cardiovascular physiology, cardiovascular disease modeling, and cardiovascular safety pharmacology assessment (Sarazan et al 2011, Jia et al 2020).
In preclinical research, the choice of an animal model is guided not only by the specific scientific objective of the study, but also by the ethical considerations associated with it (Mukherjee et al 2022). The rat is a particularly valuable model for cardiovascular research (Farag et al 2023). Therefore, several hemodynamic monitoring approaches, including invasive and non-invasive techniques, have been developed to assess cardiovascular performance in this animal species.
Invasive approaches such as flow probes (Wen et al 1996, Berthonneche et al 2005), thermodilution (Osborn et al 1986, Kelm et al 2010) and pressure-volume (PV) conductance catheter (Pacher et al 2004), provide precise and repeatable measurements of hemodynamic variables, but require vascular puncture or surgical intervention, confine the animal to physiologically constrained conditions, and usually provide only snapshot assessments. Telemetric implants (Miranda-Silva et al 2022, Van Daele et al 2022) enable continuous monitoring of hemodynamic variables in free moving animals. However, the implantation of the sensors requires major surgery. Similarly, echocardiography (Zacchigna et al 2021, Billig et al 2023), impedance cardiography (Buyukakilli et al 2014, Barlaz US et al 2024) and cardiovascular magnetic resonance imaging (Li et al 2020) although providing non-invasive alternatives, require burdensome interventions, most often under general anesthesia, and complex setups. In addition, these techniques are highly operator dependent, and their use in longitudinal protocols is limited by their strong physiological impact.
Inductive plethysmography (IP) is a non-invasive technique commonly employed to assess ventilatory function in humans (Grossman et al 2010). This technology allows instantaneous variations in trunk cross-sectional area resulting from both respiratory and cardiac activity to be recorded (Aliverti et al 2010). The IP signal comprises therefore a respiratory component, whose amplitude is proportional to the tidal volume, and a cardiac component referred to as cardiogenic oscillations (COS) (Ayappa et al 1999). Other techniques, such as monitoring suprasternal and esophageal pressures, have also been shown to effectively detect COS oscillations in humans. However, to our knowledge, these approaches have not yet been applied to small animals for cardiac activity monitoring (Cerina et al 2024). While respiratory monitoring using IP typically employs two inductive bands placed around the thorax and abdomen, the monitoring of COS utilizes a single band positioned at the mid-thorax, a configuration referred to as thoracocardiography (TCG), which has been described in humans since the early 1990s (Sackner et al 1991b).
The amplitude of the COS signal in TCG is proportional to the volume of blood ejected from the thorax during cardiac systole, providing an estimate of stroke volume. The relationship between COS and stroke volume has been validated in humans using several reference techniques, including thermodilution (Sackner et al 1991a, Bucklar et al 2003), impedance cardiography (Sackner et al 1991b, Fontecave-Jallon et al 2013), and echocardiography (Bloch et al 1998). In these studies, the reference methods were used to calibrate the TCG output into absolute volume units (liters), enabling direct comparison with clinical standards.
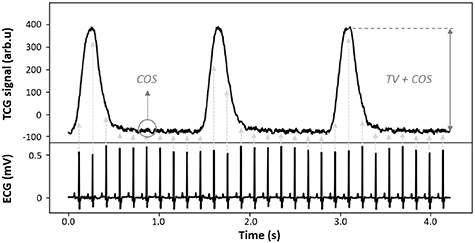
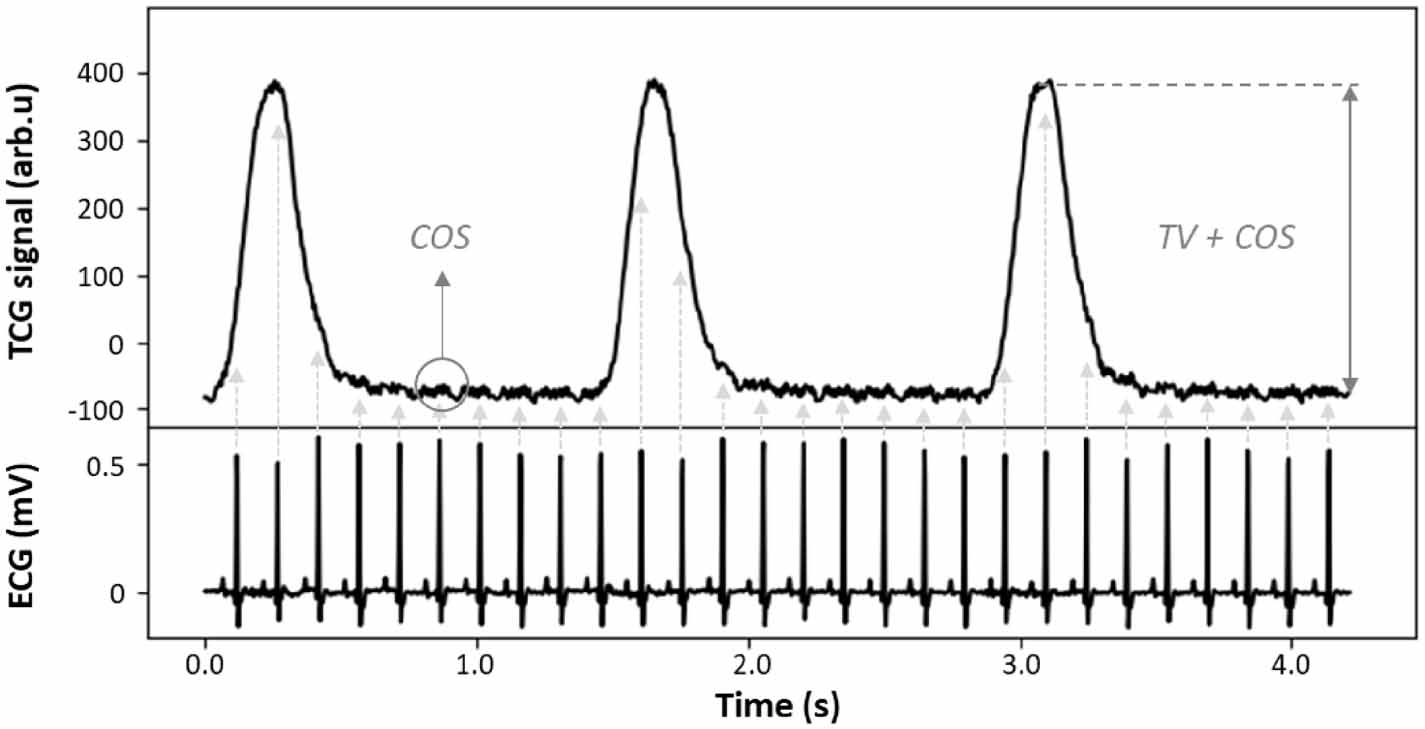
Starting in 2017, the IP technology was extended to preclinical applications (Baconnier et al 2017), which enabled the development of a high-resolution jacketed telemetry device (DECRO® Etisense, Lyon, France) designed for use in small laboratory mammals. This device has been validated for ventilatory assessment in natural locomotion or constrained exercise (Flénet et al 2017, Fares et al 2022, Fares and Champéroux 2023, Tanguy et al 2025). In addition, despite the considerable leap in scale between humans and rats in terms of heart rate and blood volumes exchanged between the trunk and the periphery, COS remain present in the TCG signal (figure 1), synchronized with the electrocardiogram (ECG). A proof of concept demonstrating the feasibility of COS recording and extraction from IP signals in anesthetized rats has already been established (Fontecave-Jallon et al 2018). However, the extraction was limited to experimentally induced apnea phases that were free from ventilatory artifacts.
Figure 1. Synchrony between ECG and TCG signals on a single rat from the pharmacological protocol of the present study. The TCG signal (upper panel) comprises a respiratory component (proportional to the TV) and a cardiac component (COS) occurring after each QRS complex, as shown in the synchronized ECG signal (lower panel). TCG = thoracocardiography; COS = cardiogenic oscillations; TV = tidal volume.
Download figure:
Standard image High-resolution imageThe main obstacle to the exploitable use of COS, particularly in small animals without ventilatory support, lies to the difficulty of extracting them from the overall TCG signal because of their very low amplitude and because they are generally drowned out by noise from both instrumental and physiological origins. Moreover, ventilatory and motion artifacts exhibit non-stationary and non-linear characteristics, as well as complex dynamics that depend on the state, behavior and physiological conditions of the animal (Scarciglia et al 2024). These characteristics make classical signal filtering insufficient for extracting COS from TCG signals.
Signal averaging techniques are widely used in biomedical signal processing (Jarrett et al 1991). Among temporal approaches, ensemble averaging (EA) aligns repeated, time-locked responses to a fiducial marker and averages them, reducing uncorrelated noise and enhancing the consistent pattern. Coherent averaging (CA) follows the same principle but additionally aligning specific internal signal features, either extracted directly from the waveform or obtained from another simultaneous measurement (Hurwitz et al 1990, Gareis et al 2017). These techniques rely on key assumptions about the averaged signal. First, the signal must be quasi-periodic. Second, it must maintain consistent synchrony with a triggering event. Finally, if noise is present, it must be uncorrelated, stationary, and Gaussian (Craelius et al 1986, Jarrett et al 1991). If these assumptions are verified, the noise root mean square is reduced by a factor of  , where N is the number of COS waveforms that are time-aligned and averaged. With a physiological trigger, a jitter corresponding to a random time shift between signals must be taken into account. On average, jitter acts as a convolution of the signal with the probability density function of its time shifts. It causes signal blurring (Rompelman and Ros 1986a, Strackee and Peper 1992), and an additional random component variability that adds to previously inventoried noises.
, where N is the number of COS waveforms that are time-aligned and averaged. With a physiological trigger, a jitter corresponding to a random time shift between signals must be taken into account. On average, jitter acts as a convolution of the signal with the probability density function of its time shifts. It causes signal blurring (Rompelman and Ros 1986a, Strackee and Peper 1992), and an additional random component variability that adds to previously inventoried noises.
Since COS in TCG signals do not exhibit the clearly defined cardiac features required for CA, and no simultaneous measurement capable of accessing those features was available in this study, the use of EA, that has been implemented in human studies (Sackner et al 1991a, 1991b, Bloch et al 1994, 1998, 1999), appears to offer a more practical approach for enhancing signal quality in the context of this study.
The assumptions underlying the EA technique may not apply to TCG and ECG signals. Thus, this study aimed to develop and evaluate an algorithm that applies EA to TCG signals using the ECG R-peak as a consistent temporal reference. The goal was to enable continuous extraction of COS using the DECRO jacketed telemetry device, estimating stroke volume from COS amplitude (SVTCG) and estimating cardiac output as SVTCG × HR (COTCG). As a first step, a metrological characterization of the IP device was performed using a mechanical test bench, in order to verify the linear relationship between cross-sectional area variations and the output of the IP signal within the physiological range relevant to rat COS. Then, the algorithm parametrization, specifically the choice of N, was evaluated under conditions of use, within the context of a pharmacological challenge in anesthetized rats without ventilatory support. Finally, the ability of the algorithm to deliver relevant physiological information during the pharmacological hemodynamic test was assessed.
2.1. IP jacketed telemetry deviceThe DECRO system is a jacketed telemetry device available for rodents and other species, that gives access to synchronous acquisition of trunk cross-sectional area variations and ECG. Cross-sectional area variations are acquired using thoracic and abdominal IP sensors sewn in the jacket and with a sampling frequency (fs) of 200 Hz (Eynard et al 2024). The present study was based on the TCG approach and therefore only the thoracic band was used. ECG signals were acquired using two surface electrodes, placed under the jacket in a lead I configuration, with a fs of 500 Hz. All signals were transmitted via Bluetooth Low Energy to an acquisition unit executing a dedicated software.
2.2. Principle of IP measurementIP measures thoracic cross-sectional area changes using a conductive coil encircling the trunk, where changes in the self-inductance ( ) of the loop are related to cross-sectional area variations (
) of the loop are related to cross-sectional area variations ( ) it encloses. This relationship is approximately linear when
) it encloses. This relationship is approximately linear when  remains small, as previously validated in humans (Martinot-Lagarde et al 1988, Watson et al 1988, Zhang et al 2012), and can be expressed as:
remains small, as previously validated in humans (Martinot-Lagarde et al 1988, Watson et al 1988, Zhang et al 2012), and can be expressed as:

where k is a constant determined by the geometry and electromagnetic properties of the coil, and  the nominal cross-sectional area enclosed by it.
the nominal cross-sectional area enclosed by it.
Assuming a cylindrical thoracic geometry with an effective height of 25–30 mm and typical tidal volumes ranging from 2.5 to 3.5 ml in adult Wistar rats weighing 300–400 g (Gross 2009), the corresponding cross-sectional area changes are estimated to be 83–140 mm2. For a nominal thoracic area of approximately 1260 mm2, this yields a relative area change  between 6.6% and 11.1%, which lies within the linear range (⩽10%–15%) established in prior human validations, where inductance is proportional to surface changes. Stroke volume in rats (100–200 μl) corresponds to even smaller cross-sectional area changes—estimated between 3.3 and 8.0 mm2—and thus remains entirely within this linear range as well. Inductance is measured by tracking the resonant frequency of an LC circuit, where the inductive element is formed by the IP band itself. A small variation in inductance (
between 6.6% and 11.1%, which lies within the linear range (⩽10%–15%) established in prior human validations, where inductance is proportional to surface changes. Stroke volume in rats (100–200 μl) corresponds to even smaller cross-sectional area changes—estimated between 3.3 and 8.0 mm2—and thus remains entirely within this linear range as well. Inductance is measured by tracking the resonant frequency of an LC circuit, where the inductive element is formed by the IP band itself. A small variation in inductance ( ) produces a corresponding change in frequency (
) produces a corresponding change in frequency ( ). The system does not directly report
). The system does not directly report  , but instead outputs the resulting frequency deviation, which is scaled and processed to reflect relative changes. These are defined here as
, but instead outputs the resulting frequency deviation, which is scaled and processed to reflect relative changes. These are defined here as  and expressed in arbitrary units (arb.u), being linearly proportional to
and expressed in arbitrary units (arb.u), being linearly proportional to  and consequently to
and consequently to  , provided the assumption of small surface variations is valid.
, provided the assumption of small surface variations is valid.
To verify the linear relationship between  and
and  , a dedicated metrological validation was performed using a mechanical test bench, as described in section 2.5. This procedure was used exclusively to verify the physical assumption that IP signal variations are linearly proportional to surface changes within the expected physiological range.
, a dedicated metrological validation was performed using a mechanical test bench, as described in section 2.5. This procedure was used exclusively to verify the physical assumption that IP signal variations are linearly proportional to surface changes within the expected physiological range.
Physiological data were analyzed and reported in arb.u, as calibration into absolute volume units would require subject-specific reference measurements, which were not available in this study. Moreover, the objective was to assess relative variations rather than absolute values, making calibration unnecessary for the intended analysis.
2.4. Proposed algorithm for cardiogenic oscillation extraction by EAAn EA algorithm was developed to extract an averaged COS waveform ( ), where N instances of COS are aligned and averaged using the R-peak of the ECG as a consistent temporal triggering event, resulting in a representative waveform. An overview of this algorithm is shown in the figure 2.
), where N instances of COS are aligned and averaged using the R-peak of the ECG as a consistent temporal triggering event, resulting in a representative waveform. An overview of this algorithm is shown in the figure 2.
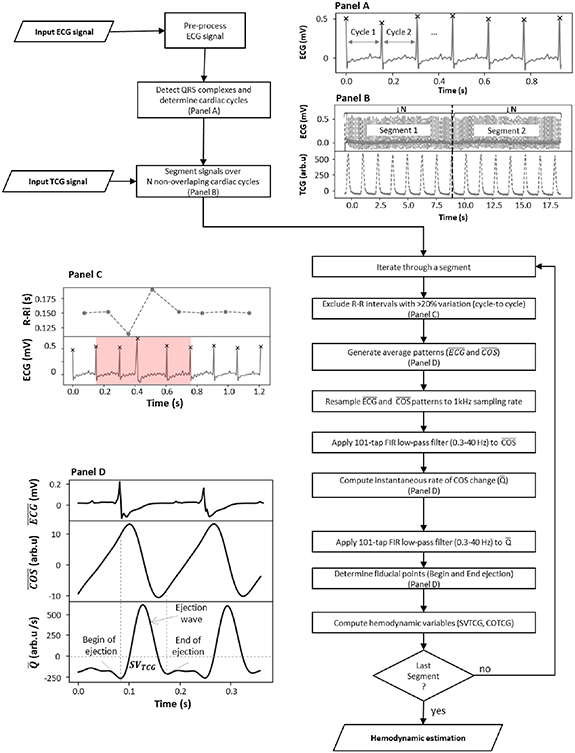
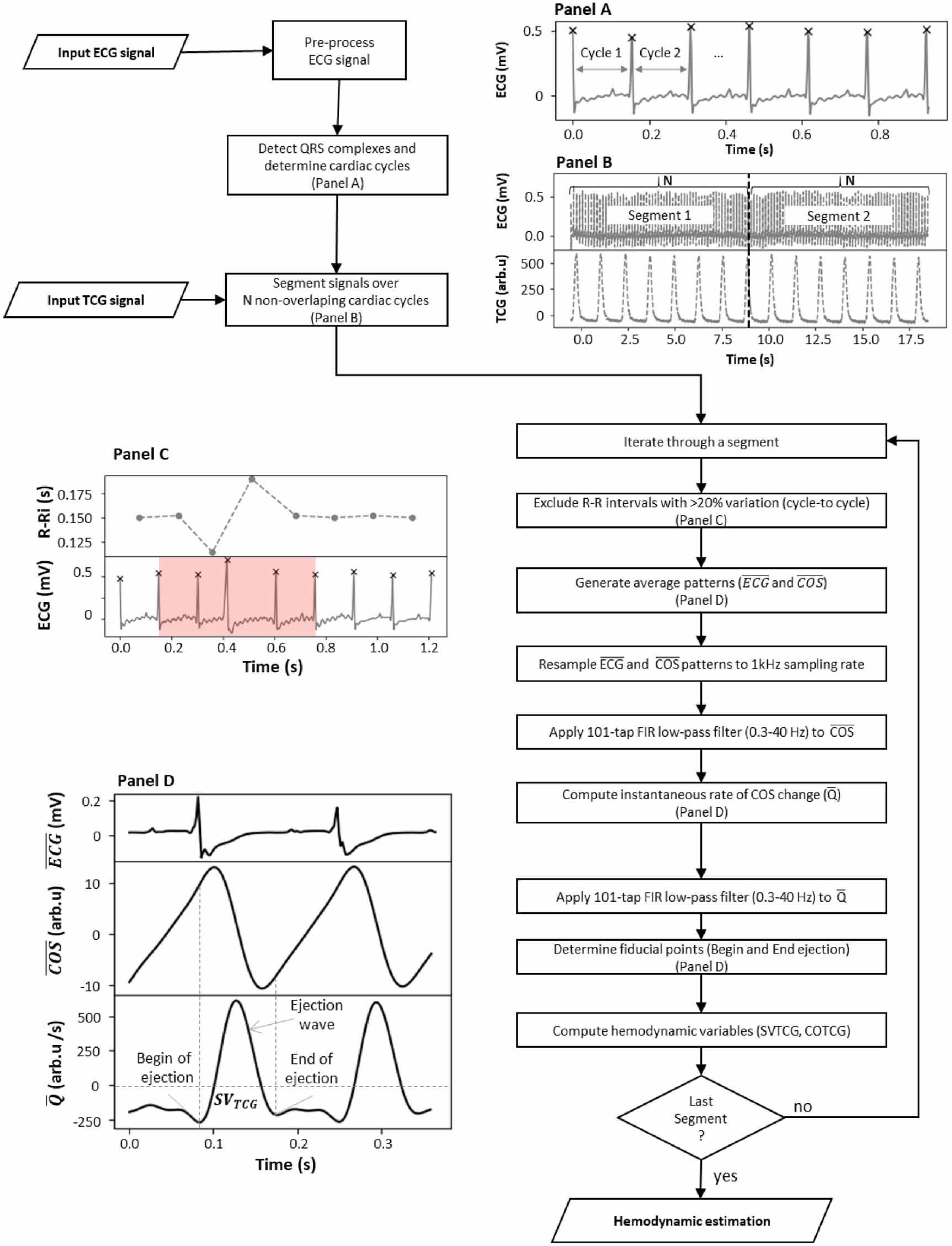
Figure 2. Flowchart of the developed algorithm based on the ensemble averaging technique to extract COS from TCG signals. (A) The ECG signal is first pre-processed to detect R-peaks. (B) Both ECG and TCG signals are then segmented into N non-overlapping cardiac cycles. (C) A percentage-based criterion is applied to the R–R intervals to exclude segments with poorly detected or missing R-peaks. (D) Valid cycles are used to generate the EA waveforms. After resampling and filtering, fiducial points are identified, and hemodynamic variables are computed.
Download figure:
Standard image High-resolution image 2.4.1. ECG signal processingThe ECG signal underwent preprocessing to detect R-peaks. Baseline wandering was removed by applying a locally weighted scatterplot smoothing algorithm (Cleveland 1979). Power line interference was removed using a zero-phase infinite impulse response (IIR) notch filter centered at 50 Hz, designed with a quality factor of 50 to ensure narrowband attenuation allowing minimal phase distortion. R-peaks were detected using a localized template correlation-based algorithm, with the template automatically defined from the ECG signal using physiological and statistical information. The cardiac cycle was defined as the interval between two consecutive R-peaks in the ECG signal (figure 2(A)). These are referred to as R-peakn and R-peakn+1, corresponding to the start and end of the cycle, respectively.
2.4.2. Signal segmentation and cycle selectionBoth ECG and TCG signals were divided into non-overlapping segments, each containing N consecutive cardiac cycles (figure 2(B)). To facilitate the determination of fiducial points, the averaged waveform was computed over TCG cardiac cycles, extended by 0.5% of the mean R–R interval before R-peakn and 0.7% after R-peakn+1. Since cardiac TCG cycles were matched with the corresponding R-peaks for EA, all cycles with poorly detected or absent R-peaks, due to rhythm disturbances or detection artifacts, were excluded (figure 2(C)). This was achieved using a percentage-based criterion on the R–R intervals: a cycle was excluded if its R–R interval differed by more than 20% from the preceding or following interval (Karey et al 2019). A score associated with each segment was then calculated as the percentage of remaining valid cycles (after selection) relative to the total N cycles previously defined for the generation of EA waveforms.
2.4.3. EA waveform generation and inherent errorsAfter signal segmentation and cycle selection, the remaining ECG and TCG cycles were aligned at R-peakn and averaged to generate the averaged ECG waveform ( ) and the averaged COS waveform (
) and the averaged COS waveform ( ), respectively, which were then resampled on a same sampling grid at 1 kHz. A 101-tap finite impulse response (FIR) low-pass (LP) filter (40 Hz) was applied to attenuate high-frequency and non-stationary noise not eliminated by averaging. The raw instantaneous flow of
), respectively, which were then resampled on a same sampling grid at 1 kHz. A 101-tap finite impulse response (FIR) low-pass (LP) filter (40 Hz) was applied to attenuate high-frequency and non-stationary noise not eliminated by averaging. The raw instantaneous flow of  (
( ) was estimated as the first derivative (difference between two consecutive points) of the
) was estimated as the first derivative (difference between two consecutive points) of the  waveform and inverted (multiplied by −1) so that positive deflections indicate systolic forward flow. The resulting waveform was then filtered with the same 101-tap FIR LP filter (40 Hz), defined as
waveform and inverted (multiplied by −1) so that positive deflections indicate systolic forward flow. The resulting waveform was then filtered with the same 101-tap FIR LP filter (40 Hz), defined as  (figure 2(D)).
(figure 2(D)).
EA reduces non–phase-locked noise, but errors arise from physiological trigger jitter—beat-to-beat variability in electromechanical delay. First, a persistent bias arises because misaligned beats make the EA equal to the true waveform convolved with the jitter distribution, smoothing high-curvature features (e.g. the systolic upstroke); this corresponds to the classic ‘equivalent-filter/temporal blur’ view and has been demonstrated in biomedical time-CA (Rompelman and Ros 1986a, Strackee and Peper 1992, Alegria 2025). Second, in addition to this persistent bias, the EA contains a random component expected to shrink with N. Since only an averaged waveform (rather than beat-to-beat) is available, the jitter distribution cannot be identified and as it is likely non-stationary (protocol-dependent). Its impact cannot be reliably modeled, making experimental validation against a reference the most appropriate approach.
2.4.4. Fiducial point detection and hemodynamic variable computationFiducial points were detected around the first R-peak (figure 2(D)), while the second R-peak was included to support more accurate detection of these points. Two key points were identified on the  waveform: the begin and end of ejection defined as the first valley before the ejection wave and the second valley after the ejection wave, respectively. Hemodynamic variables were then computed: stroke volume estimated by thoracocardiography (SVTCG) was defined as the area under the
waveform: the begin and end of ejection defined as the first valley before the ejection wave and the second valley after the ejection wave, respectively. Hemodynamic variables were then computed: stroke volume estimated by thoracocardiography (SVTCG) was defined as the area under the  curve between the start and the end of ejection, and cardiac output estimated by thoracocardiography (COTCG) was calculated as the product of SVTCG and the average HR over the segment. These variables are expressed in arbitrary units (arb.u) and arb.u/min, respectively.
curve between the start and the end of ejection, and cardiac output estimated by thoracocardiography (COTCG) was calculated as the product of SVTCG and the average HR over the segment. These variables are expressed in arbitrary units (arb.u) and arb.u/min, respectively.
A mechanical test bench designed based on a cylindrical model representing the trunk of a 350 g rat, with a radius of 20 mm, was used to evaluate the performance of the sensor under controlled conditions. To simulate thoracic volume variations proportional to changes in  , the bench is composed of two juxtaposed half-cylinders: one fixed and the other actuated by a stepper motor capable of a minimal displacement (d) of 0.781 μm, corresponding to a minimum variation in cross-sectional area variations of
, the bench is composed of two juxtaposed half-cylinders: one fixed and the other actuated by a stepper motor capable of a minimal displacement (d) of 0.781 μm, corresponding to a minimum variation in cross-sectional area variations of  mm2.
mm2.  are simulated by adjusting the distance between the half-cylinders. This adjustment is digitally controlled by an input signal sent to the bench and recorded by the IP telemetry jacket placed on the bench.
are simulated by adjusting the distance between the half-cylinders. This adjustment is digitally controlled by an input signal sent to the bench and recorded by the IP telemetry jacket placed on the bench.
A protocol was developed to assess sensitivity, linearity, repeatability, and resolution. It involved sending a sinusoidal input signal ( Hz) at a constant frequency of 6 Hz to simulate the resting HR of a rat. This signal consisted of successive recording segments, each comprising 60 sinusoidal cycles, with amplitudes ranging from 8.325 μm to 108.325 μm, in discrete increments of 0.833 μm, resulting in
Hz) at a constant frequency of 6 Hz to simulate the resting HR of a rat. This signal consisted of successive recording segments, each comprising 60 sinusoidal cycles, with amplitudes ranging from 8.325 μm to 108.325 μm, in discrete increments of 0.833 μm, resulting in  from 0.333 to 4.333 mm2 in 0.033 mm2 steps. These amplitudes were chosen to simulate cross-sectional area changes within the physiological range for a 350 g rat with a typical stroke volume of approximately 100 μl. For each segment, an EA average waveform was generated over the 60 cycles, and the amplitude (peak-to-valley) was calculated. This process was repeated eight times.
from 0.333 to 4.333 mm2 in 0.033 mm2 steps. These amplitudes were chosen to simulate cross-sectional area changes within the physiological range for a 350 g rat with a typical stroke volume of approximately 100 μl. For each segment, an EA average waveform was generated over the 60 cycles, and the amplitude (peak-to-valley) was calculated. This process was repeated eight times.
To estimate sensitivity, a linear model without intercept was fitted between the  values recorded by the IP device and the corresponding
values recorded by the IP device and the corresponding  imposed by the test bench, enabling calibration from arb.u to mm2. The linearity of the device was quantified using the Pearson correlation coefficient (r). In addition, agreement between the calibrated measurements and the reference values from the test bench was assessed using a Bland–Altman (B&A) analysis (Bland and Altman 1986). Repeatability and numerical resolution were evaluated using the minimal detectable change (MDC), calculated as:
imposed by the test bench, enabling calibration from arb.u to mm2. The linearity of the device was quantified using the Pearson correlation coefficient (r). In addition, agreement between the calibrated measurements and the reference values from the test bench was assessed using a Bland–Altman (B&A) analysis (Bland and Altman 1986). Repeatability and numerical resolution were evaluated using the minimal detectable change (MDC), calculated as:
where MSE is the mean square error from the ANOVA residuals, and n is the number of repetitions of the protocol.
2.6. In vivo validation in anesthetized rats2.6.1. EthicsExperiments were conducted following the guidelines of European (L276-33 2010/63/EU) and French (AGRG1231951D) regulations concerning the protection and use of laboratory animals and with the recommendations of Helsinki declaration. This study was approved by the ethics committee #12 (Grenoble Alpes University) accredited by the French Ministry of Higher Education and Research (Agreement: APAFIS#31355-2021042918003831).
2.6.2. AnimalsMale Wistar rats (n = 10, aged 9–10 weeks, 300–350 g, from Charles River, Lyon, France) were housed in pairs in conventional cages (Techniplast, Louvier, France) placed in controlled animal facility (Pressure = 1.0 ± 0.5 bar, T = 20–24 °C, hygrometry = 40% to 70%, day/night cycle = 12 h/12 h), changed twice a week, with free access to water and food. Animals were marked for identification (ink marks on the tail), and provided with various types of enrichment, including nesting materials, gnawing objects, and cardboard tunnels (Comptoir des sciures, Meyzieu, France). Animals were acclimatized to the study housing conditions for at least 7 d before the start of study.
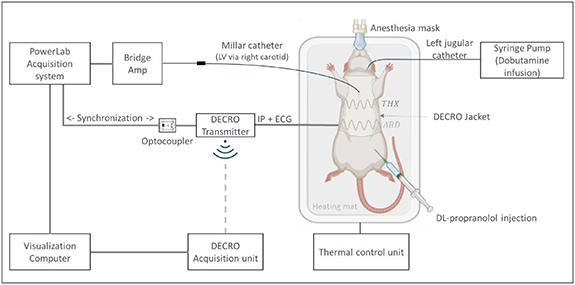
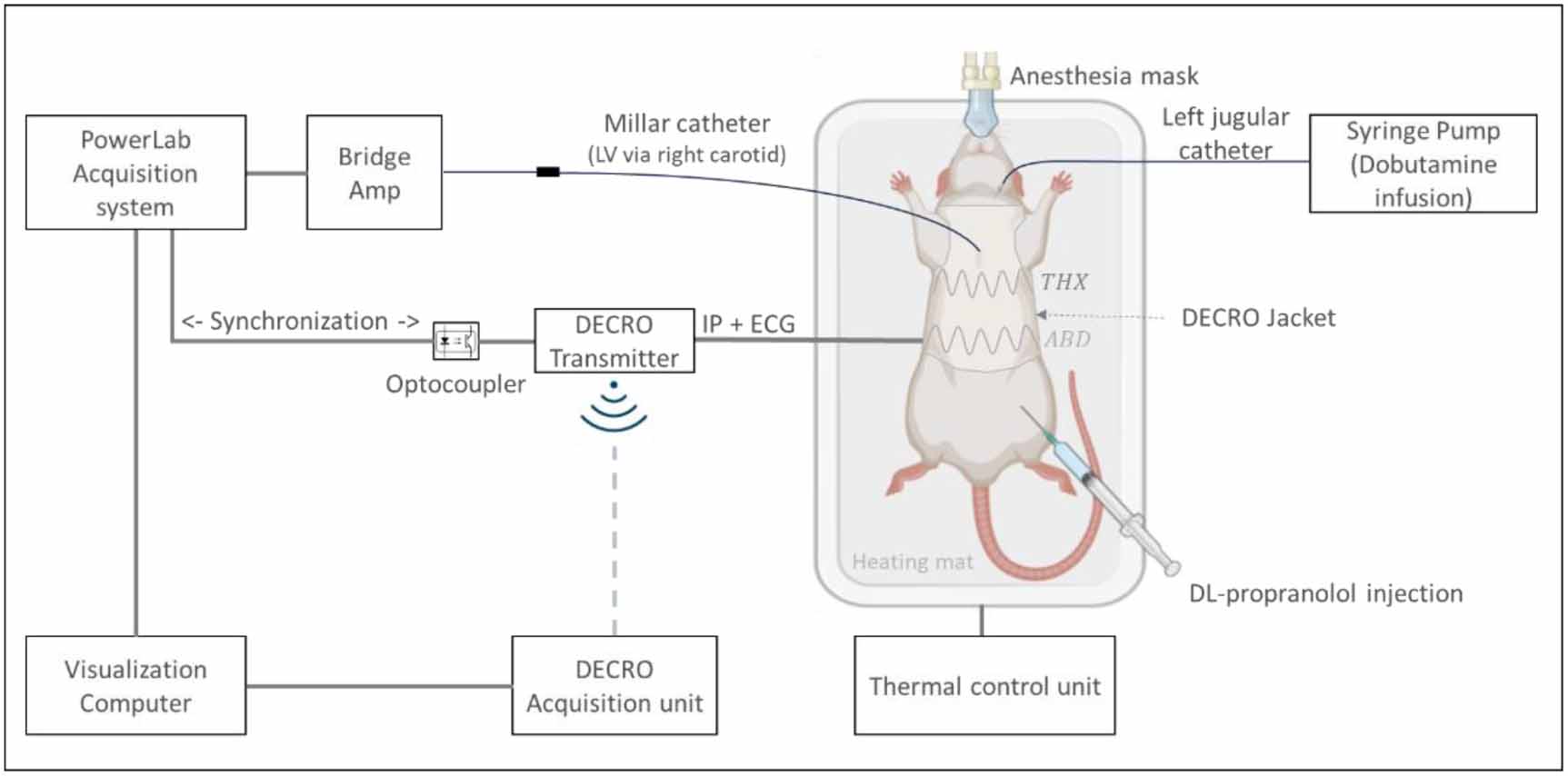
2.6.3. Experimental setupAll procedures involving animals were performed under anesthesia throughout the duration of the protocol, which lasted a maximum of 120 min. Volatile anesthesia consisted of an induction phase in a closed box at 5% isoflurane, followed by a maintenance phase under a mask delivering 2.0%–2.5% isoflurane. Surface ECG electrodes were placed to the shaved dorsal skin between the first and fourth rib on both sides of the spine, in a lead I configuration. The animals were then fitted with the jacketed telemetry DECRO device with the transmitter placed laterally in this setup to accommodate the animal’s dorsal recumbency on the heating mat (figure 3).
Figure 3. Experimental setup: signals were recorded simultaneously with the jacketed telemetry device and with the Millar pressure probe.
Download figure:
Standard image High-resolution imageAfter the animal was fitted with the telemetry device, a Millar Mikro-Tip® catheter (SPR-407 2F, Millar Inc., Houston, TX, USA) was inserted into the left ventricle (LV) via the right carotid artery. Additionally, the left external jugular vein was catheterized with a polyethylene catheter for dobutamine infusion. The Millar pressure probe was connected to a PowerLab® (26 Series, ADInstruments, Bella Vista, New South Wales, Australia) via a non-isolated bridge amplifier (Quad Bridge Amp®, ADInstruments, Bella Vista, New South Wales, Australia) to allow left ventricular pressure (LVP) monitoring. Acquisition devices (DECRO and PowerLab) were synchronized and launched simultaneously.
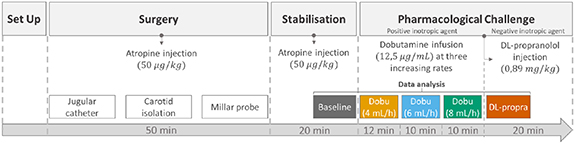
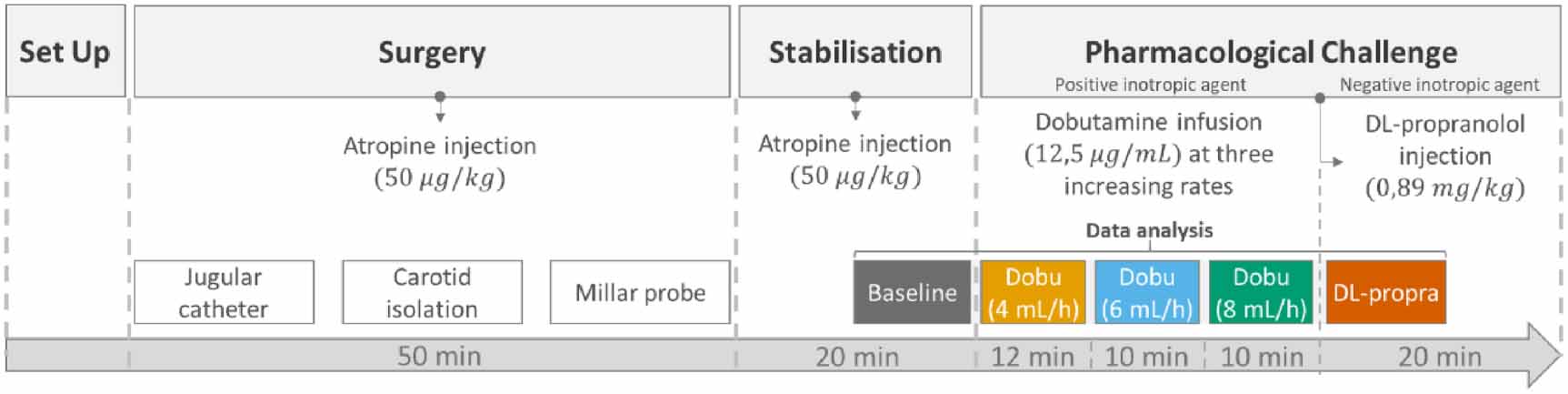
2.6.4. Experimental protocolAfter a 20 min stabilization period, a pharmacological challenge was performed (figure 4). A continuous intravenous infusion of dobutamine (12.5 mg ml−1, i.v., Dobutamine hydrochloride PANPHARMA, France), was administered in three successive phases, at infusion rates of 4 ml h−1, 6 ml h−1 and 8 ml h−1, for 12 min in the first phase and for 10 min for the second and third phases, respectively. At the end of the last phase of dobutamine infusion, a bolus of DL-propranolol 0.89 mg kg−1 (1 ml kg−1, i.v., DL-propranolol hydrochloride, Sigma, France) was administered through the saphenous vein.
Figure 4. Experimental protocol. After equipment and animal preparation (set up), the surgery phase was conducted (50 min), followed by a 20 min stabilization period. Then the pharmacological challenge was started with dobutamine infusion at three different rates (4 ml h−1, 6 ml h−1, and 8 ml h−1), followed by DL-propranolol injection. Dobu = dobutamine infusion (12.5 mg ml−1, i.v.); DL-propra = DL-propranolol injection (0.89 mg kg−1, i.v.).
Download figure:
Standard image High-resolution imageBefore carotid isolation and at the beginning of the stabilization period, a bolus of atropine (50 μg kg−1, 250 μl kg−1; i.m.) was injected to prevent the effects of vagal stimulation related to carotid denervation and pharmacological hemodynamic stress. All animals were euthanized with an injection of sodium pentobarbital (120 mg kg−1; i.v.), 20 min after the DL-propranolol injection.
2.6.5. Data analysis and statisticsHemodynamic variables assessed. HR, SVTCG and COTCG were obtained from the IP device, whereas left ventricular developed pressure (LVDevP) was calculated from the LVP signal, as the difference between systolic and end-diastolic pressures, measured with the intracardiac Millar probe. All variables were obtained using the same EA approach.
Plateau identification. For each animal, plateaus were individually identified for HR and SVTCG at each phase of the protocol. Baseline was defined as the value of the plateau phase of the stabilization period preceding the first phase of dobutamine infusion. All subsequent analyses were limited to these plateau periods.
Adjustment relative to baseline.At the time of surgery, the weight of the animals included in the study was uniform (362 ± 10 g; range: 348–382 g). For this reason, the measured values were not normalized in relation to body weight. To take into account the inter-subject variability, data were expressed as relative changes from the baseline values for each animal. The suitability of this approach was evaluated by calculating, for each animal, the coefficient of variation (CV) of baseline SVTCG, defined as the standard deviation (SD) divided by the mean, and expressed as a percentage; a CV of ⩽25% was considered acceptable for baseline stability.
Influence of N on the results. The influence of N on the results was evaluated in four analyses. In the first analysis, the impact of N on SVTCG amplitude and variability was assessed, using the baseline data, varying N from 10 to 200 in increments of 10. For each value of N, the mean and SD of SVTCG were calculated across the entire population. A non-linear model was then fitted to the SD values and compared to the theoretical noise reduction curve defined as  .
.
For the subsequent analyses, three representative values of N were selected: 30, 60, and 200. In the second analysis, the sensitivity index (SI) was calculated on the SVTCG variable for each rat of the experimental protocol. This index represents a standardized measure of the magnitude of the effect. It is used to quantify the effectiveness with which a variable distinguishes between two physiological states (e.g. treatment vs baseline), and was based on the definition of Cohen’s d’ for independent samples (Cohen 1977, Bland and Altman 1986, Ellis 2010). It is defined as:
where  mean represents the difference between the mean SVTCG of each phase of the protocol (dobutamine and DL-propranolol) and the mean SVTCG of the baseline. Pooled SD represents the variability of SVTCG before adjustment relative to baseline from both treatment and baseline, and is defined as:
mean represents the difference between the mean SVTCG of each phase of the protocol (dobutamine and DL-propranolol) and the mean SVTCG of the baseline. Pooled SD represents the variability of SVTCG before adjustment relative to baseline from both treatment and baseline, and is defined as:

where n represents the number of data points within each plateau phase, and n–1 corresponds to the degrees of freedom in estimating variance from sample data, thus ensuring an unbiased estimate of variability. Population-level results of SI were reported as mean ± standard error of the mean (SEM), representing the precision of the group mean across rats. Statistical significance was assessed using a one-sample t-test against baseline.
In the third analysis, the frequency of occurrence of the EA output was determined by the HR/N ratio, corresponding to one data point every N heart beats. This corresponds to a frequency of HR/N occurrences per minute. The mean and SD of the score–defined as the percentage of cardiac cycles used for EA computation–were then calculated across all protocol phases for each value of N.
In the last analysis of the influence of N, a qualitative analysis was performed on the average waveform for different values of N.
Physiological effects. To validate the correct extraction of COS from the TCG signal, the evolution of the  waveforms was analyzed throughout the pharmacological protocol using a waterfall plot for each rat. Each
waveforms was analyzed throughout the pharmacological protocol using a waterfall plot for each rat. Each  waveform was time-aligned to the corresponding R-peak and started at time zero, with its duration determined by the corresponding HR. This plot served as a qualitative tool to visually assess waveform consistency and stationarity across protocol phases.
waveform was time-aligned to the corresponding R-peak and started at time zero, with its duration determined by the corresponding HR. This plot served as a qualitative tool to visually assess waveform consistency and stationarity across protocol phases.
Physiological effects at the population level were then evaluated across the protocol phases for the selected N. The mean of the plateau was calculated for each rat. A Friedman test was performed to identify mean differences between protocol phases, followed by Wilcoxon signed-rank post hoc tests to assess pairwise differences from baseline. p < 0.05 was taken as the limit of statistical difference.
The algorithm was developed in Python (version 3.7.0). All statistical analyses were performed using the R language (RStudio 2023.06.1).
The main objective of this study was to evaluate the ability of an algorithm based on the EA technique to continuously extract COS from the TCG signal acquired using the DECRO jacketed telemetry device in anesthetized rats without ventilatory support. At first, a mechanical test bench was used to evaluate the performance of the sensor. Next, the optimal parametrization of the algorithm was determined under realistic conditions of use in a pharmacological test performed in ten anesthetized rats with a passive mask. Finally, changes in stroke volume and cardiac output were determined using the algorithm during the different phases of the pharmacological hemodynamic challenge.
4.1. Metrological qualificationAs the DECRO jacketed telemetry device gives access to  by measuring changes in resonant frequency, its output is scaled, processed and expressed in arbitrary units. Since the aim of this study was to evaluate relative changes, and calibration into volume units would require subject-specific reference measurements, physiological results were kept in arbitrary units, which is commonly used in physiology and pharmacology when absolute calibration is not feasible.
by measuring changes in resonant frequency, its output is scaled, processed and expressed in arbitrary units. Since the aim of this study was to evaluate relative changes, and calibration into volume units would require subject-specific reference measurements, physiological results were kept in arbitrary units, which is commonly used in physiology and pharmacology when absolute calibration is not feasible.
The relationship between  and
and  can be considered linear if
can be considered linear if  remains low relative to the nominal surface area, as previously verified in humans (Martinot-Lagarde et al 1988, Watson et al 1988, Zhang et al 2012). Despite the differences in scale between humans and rats, the evaluation performed using a mechanical test bench showed that the system remains linear within the target range of use, with a high degree of linearity (
remains low relative to the nominal surface area, as previously verified in humans (Martinot-Lagarde et al 1988, Watson et al 1988, Zhang et al 2012). Despite the differences in scale between humans and rats, the evaluation performed using a mechanical test bench showed that the system remains linear within the target range of use, with a high degree of linearity ( ) between cross-sectional variations measured in arbitrary units with the IP device and those imposed by the test bench in mm2. Furthermore, the system showed no systematic bias between measurements, according to the B&A analysis presented in the figure 5(b), achieving an agreement of
) between cross-sectional variations measured in arbitrary units with the IP device and those imposed by the test bench in mm2. Furthermore, the system showed no systematic bias between measurements, according to the B&A analysis presented in the figure 5(b), achieving an agreement of  and
and
Comments (0)