
Remember me
This study included 10,631,427 individuals (Supplemental Figure S1), 30.2% of whom were aged 18–49 years, 18.0% were 50–64 years, and 51.7% were ≥ 65 years at start of follow-up (Table 1).
Table 1 Baseline demographics and clinical characteristics by age group and overallComorbidity and MultimorbidityMore than 7.8 million individuals had a high-risk condition (73.6% of the overall cohort) (Table 1). A single high-risk condition was found in 23.4%, 18.7%, and 9.7% of individuals aged 18–49, 50–64, and ≥ 65 years, respectively. Multimorbidity was characteristic of 27.2%, 56.2%, and 76.9% of individuals in those age groups, respectively. Other disorders of blood or blood-forming organs (6.1%) and prolonged use of corticosteroids or other immunosuppressive agents (2.7%) were the most common IC, and most of the individuals with IC had only one such problem (Supplemental Table S2). For the overall study population, heart conditions or chronic heart disease (CHD; 28.1%) was the most common HR-Conclusive condition, followed by cancer (21.5%), obesity (23.0%), and diabetes mellitus (DBT) (20.3%). Being overweight (12.2%) was the most common HR-Suggestive condition, and HTN (47.4%) was the most common Mixed Evidence condition.
The most frequently observed comorbid conditions in any evidence category were HTN (47.4%), obesity/overweight (31.9%), CHD (28.1%), and DBT (20.3%; Table 2). The most common multimorbidity combination was obesity with HTN (22.1%). The most frequent condition among the 18–49-year group was obesity/overweight (21.9%); HTN was the most common among the 50–64- (44.6%) and ≥ 65- (69.3%) year groups.
Table 2 High frequency comorbidities and multimorbidity by age group and overallComorbidity combinations were more common among the ≥ 65-year-olds (3.0–30.3%), followed by the 50–64-year-olds (1.3–24.7%) (Table 2). Obesity with HTN, obesity with CHD, and obesity with DBT were among the most frequent across all age groups. CHD with DBT, CHD with chronic pulmonary disease, and CHD with chronic kidney disease were noticeably more prevalent in the ≥ 65-year-old age group than either of the younger groups.
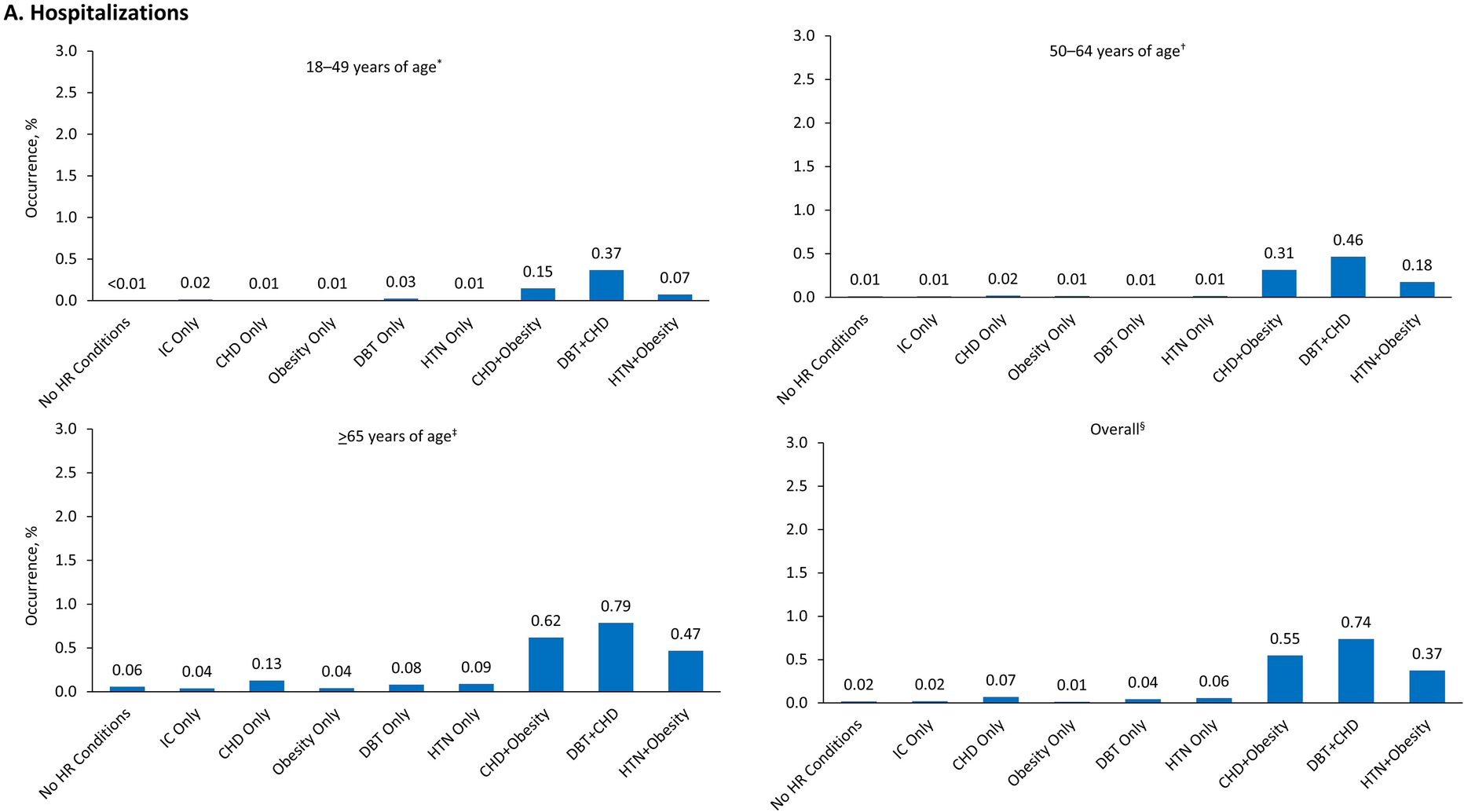
Outcomes by Comorbidities and MultimorbiditiesAcross all ages, poor COVID-19–related outcomes were most frequent among those with CHD and DBT, CHD and obesity, and HTN and obesity with predominance in ≥ 65-year-olds over both 18–49- and 50–64-year-olds (Fig. 1). Specifically, among individuals with CHD and DBT (n = 1,129,319), COVID-19–related hospitalizations occurred for 0.79% versus 0.37% and 0.46% of those aged ≥ 65 years, 18–49 years, and 50–64 years, respectively; ED/UC visits for 0.96% versus 0.80% and 0.77%; and outpatient visits for 2.70% versus 2.62% and 2.55%. Among those with CHD and obesity (n = 1,385,872), COVID-19–related hospitalizations occurred for 0.62% versus 0.15% and 0.31% of those aged ≥ 65 years, 18–49 years, and 50–64 years, respectively; ED/UC visits for 0.83% versus 0.49% and 0.62%; and outpatient visits for 2.73% versus 2.42% and 2.61%. Among those with HTN and obesity (n = 2,345,741), COVID-19–related hospitalizations occurred for 0.47% versus 0.07% and 0.18% of those aged ≥ 65 years, 18–49 years, and 50–64 years, respectively; ED/UC visits for 0.66% versus 0.30% and 0.41%; and outpatient visits for 2.48% versus 2.03% and 2.27%. Thus, older age was shown to be an additional risk factor for HCRU in addition to multimorbidity.
Fig. 1


COVID-19–related A Hospitalizations, B ED/UC visits, and C outpatient visits by age group and overall. *Sample sizes, 18–49 years of age: no HR conditions, 1,589,911; IC Only, 19,882; CHD only, 19,943; obesity only, 202,593; DBT only, 15,912; HTN only, 54,543; CHD + obesity, 68,906; DBT + CHD, 24,467; HTN + obesity, 206,695. †Sample sizes, 50–64 years of age: no HR conditions, 480,959; IC only, 9,262; CHD only, 15,417; obesity only, 80,793; DBT only, 15,658; HTN only, 89,210; CHD + obesity, 216,874; DBT + CHD, 139,850; HTN + obesity, 474,784. ‡Sample sizes, ≥ 65 years of age: no HR conditions, 737,338; IC only, 10,110; CHD only, 35,003; obesity only, 55,469; DBT only, 24,717; HTN only, 207,074; CHD + obesity, 1,100,092; DBT + CHD, 965,002; HTN + obesity, 1,664,262. §Sample sizes, Overall: no HR conditions, 2,808,208; IC only, 39,254; CHD only, 70,363; obesity only, 338,855; DBT only, 56,287; HTN only, 350,827; CHD + obesity, 1,385,872; DBT + CHD, 1,129,319; HTN + obesity, 2,345,741. CHD heart conditions/chronic heart disease, DBT diabetes mellitus, ED/UC emergency department/urgent care, HTN hypertension, HR high risk, IC Immunocompromising conditions
Risk Stacking: Clinical OutcomesCOVID-19–Related HospitalizationsOverall, individuals with IC plus any other HR conditions were at higher adjusted risk of hospitalization than those with only IC (aHzR, 10.96; 95% CI 5.48–21.93) (Fig. 2A), and this was consistent for all age groups (Supplemental Figures S2A, S3A, and S4A). Additionally, having ≥ 2 high-risk conditions increased the risk of hospitalization compared with individuals with only one condition within the risk categories and with IC individuals (Fig. 2A and Supplemental Figs. S2A, S3A, and S4A). HR-Conclusive conditions conferred greater risk of hospitalization (aHzR, 3.99; 95% CI 2.72–5.87) compared with IC, with or without other comorbidities, whereas HR-Suggestive conditions and Mixed Evidence were associated with somewhat lower incremental hospitalization risk (aHzRHR-Suggestive, 1.04; 95% CI 1.00–1.08; aHzRMixed Evidence, 1.06; 95% CI 0.97–1.15), which may be only marginally significant. IC combined with both HR-Conclusive and HR-Suggestive conditions (i.e., all 3 present; aHzR, 16.84; 95% CI 9.97–28.46) conferred the greatest risk compared with IC and each of the single categories. Close examination showed that the impact of a particular condition category (HR-Conclusive, HR-Suggestive, or Mixed Evidence) on risk was stronger for hospitalizations than for ED/UC visits and outpatient visits.
Fig. 2


Impact of multimorbidity risk stacking on the risk of A inpatient hospitalization, B ED/UC visits, and C outpatient visits: overall study population. aHzR adjusted hazard ratio, CI confidence interval, ED/UC emergency department/urgent care, HR high risk, IC immunocompromising conditions, HCRU healthcare resource utilization. Models were adjusted for continuous age and categorical sex (female or male), vaccination status ≥ 7 days prior to the start of HCRU assessment (vaccinated, yes or no), and time between prior vaccination and start of HCRU assessment (7–89 days, 90–179 days, and ≥ 180 days). The IC category was used as the baseline comparator category because clinical guidelines prioritize these individuals for COVID-19 vaccination and treatment [15, 16]
COVID-19–Related ED/UC VisitsIndividuals overall with IC plus any other HR conditions were at higher adjusted risk of ED/UC visits than those with only IC (aHzR, 4.07; 95% CI 3.03–5.48) (Fig. 2B) and this was consistent independent of age group (Supplemental Figures S2B, S3B, and S4B). Unlike the findings for hospitalizations overall, HR-Suggestive and Mixed Evidence conditions had similar risk of ED/UC visits as was found among those with IC (aHzR, 0.96; 95% CI 0.92–0.99; aHzR, 0.99; 95% CI 0.93–1.05, respectively). Similar to hospitalizations, the risk of ED/UC visits increased with having ≥ 2 high-risk conditions compared with having only one condition within the risk categories but also compared with HR Conclusive IC individuals (Figs. 2B and Supplemental Figures S2B, S3B, and S4B).
COVID-19–Related Outpatient VisitsIndividuals with IC plus any other HR conditions were at higher adjusted risk of COVID-19–related outpatient visits than those with only IC (aHzR, 1.42; 95%, CI 1.31–1.54) (Fig. 2C). As with hospitalizations and ED/UC visits, having ≥ 2 high-risk conditions increased the risk of outpatient visits compared with having only one condition within the risk categories. Also like hospitalizations, HR-Conclusive conditions elevated the risk of outpatient visits (aHzR, 1.23; 95% CI 1.16–1.31); however, HR-Suggestive and Mixed Evidence conditions did not confer widely different outpatient visit risk compared with IC (aHzR, 0.95; 95% CI 0.93–0.97; and aHzR, 0.91; 95% CI 0.89–0.93, respectively). IC combined with both non-IC HR-Conclusive and HR-Suggestive conditions (i.e., all 3 present; aHzR, 1.72; 95% CI 1.60–1.84) conferred the greatest risk of outpatient visits compared with single categories (Fig. 2C and Supplemental Figures S2C, S3C, and S4C).
Outcomes in Younger Multimorbid Individuals Versus Age ≥ 65 Years Without HR ConditionsIndividuals with IC who were aged 18–49 or 50–64 years had greater risk of COVID-19–related hospitalization than those aged ≥ 65 years without HR conditions, as demonstrated by hazard ratios comparing with those without HR conditions: aHzRAge18–49 was 46.60 (95% CI 33.67–64.48), aHzRAge50–64 was31.23 (95% CI 23.62–41.30), and aHzRAge≥65 was 15.05 (95% CI 13.63–16.62) (Supplemental Table S3). Furthermore, younger individuals with IC were also at greater risk than their counterparts without HR conditions with respect to ED/UC visits (aHzRAge18–49, 6.27; 95% CI 5.63–6.98; aHzRAge50–64, 8.46; 95% CI 7.50–9.54) and outpatient visits (aHzRAge18–49, 2.76; 95% CI 2.65–2.88, aHzRAge50–64, 2.83; 95% CI 2.72–2.95). Additionally, HR-Conclusive conditions were sometimes shown to confer higher risk than IC among individuals < 65 years. For instance, compared with IC individuals, those with non-IC HR-Conclusive conditions who were aged 50–64 years were more at risk of hospitalization than those aged ≥ 65 years (aHzRAge50–64, 6.06; 95% CI 1.95–18.81 versus aHzRAge≥65, 4.17; 95% CI 2.63–6.63) (Supplemental Figures S3A and S4A). For ED/UC visits and outpatient visits, there was still greater risk for individuals with multiple HR conditions than for those who had only one (Supplemental Figures S2B, S2C, S3B, S3C, S4B, and S4C), although not always equal to or higher than for age ≥ 65 years.
Comments (0)