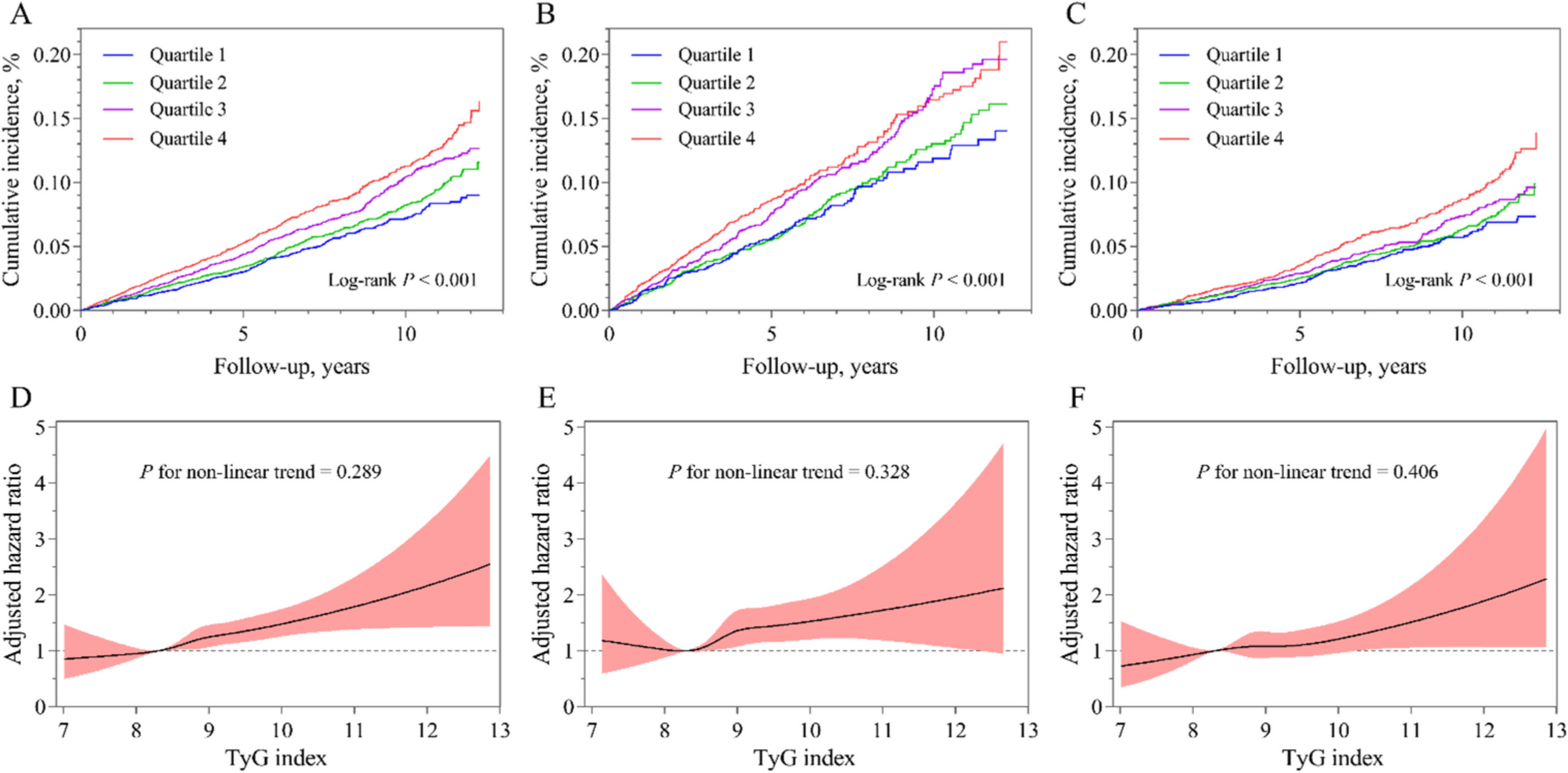
From the perspective of PPPM, clarifying the relationship between metabolic dysfunction (captured by the TyG index and its derivatives) and postpartum CVD is essential for early prediction of individual risk trajectories, targeted prevention focused on modifiable metabolic pathways, and personalized interventions aligned with patient-specific risk profiles [30, 31]. In this longitudinal cohort of 1,642 women with a history of HDP from the UK Biobank, our findings advance each of these objectives: (1) all TyG indices were significantly higher in women who developed postpartum CVD, with the highest tertiles associated with markedly increased risk (adjusted HRs: 1.31–1.39); (2) RCS analyses demonstrated linear dose–response relationships between TyG indices and postpartum CVD risk; and (3) these associations remained robust across strata defined by age, obesity status, and baseline hypertension. To our knowledge, this is the first study to systematically integrate observational and genetic evidence, identifying TyG indices as both predictive biomarkers and potential causal mediators of postpartum CVD risk in this high-risk group and thereby providing a foundation for PPPM-guided postpartum cardiovascular care.
The interplay among insulin resistance, visceral adiposity, and CVD risk in women with prior HDP is an area of increasing mechanistic and clinical interest. Multiple studies have explored these associations [2, 23, 32], with Tschiderer et al. [33] employing Mendelian randomization to demonstrate that genetic susceptibility to HDP correlates with unfavorable cardiovascular profiles, while Groenhof et al. [34] documented heightened risk of developing hypertension later in life among women with prior HDP. While previous work has established HDP as an important marker of future hypertension and CVD [23, 31, 34], our study extends this paradigm by demonstrating that TyG indices, which jointly reflect insulin resistance and adverse adiposity, serve as quantifiable, potentially modifiable risk factors spanning the continuum from pregnancy to long-term cardiovascular health. By documenting robust temporal associations between baseline TyG indices and incident CVD events years after delivery, our results offer new PPPM-aligned insights for risk prediction and targeted prevention. Notably, the predictive effect of the TyG index was particularly prominent in subgroups typically considered clinically low-risk, including younger women, individuals with normal baseline blood pressure, and non-obese subjects. This pattern suggests that the TyG index may capture early compensatory metabolic dysfunction, characterized by adverse visceral fat distribution and subclinical inflammation, even before overt obesity or hypertension becomes apparent. This phenomenon aligns closely with the "insulin resistance (IR) visceral obesity" axis [35], where insulin resistance impairs endothelial nitric oxide synthase (eNOS) activity, reducing nitric oxide bioavailability, while visceral adiposity promotes the secretion of pro-inflammatory cytokines, creating a pro-oxidant, pro-inflammatory state [36, 37]. This axis synergizes with HDP-induced placental ischemia and oxidative stress pathways, thereby establishing a persistent foundation for postpartum cardiovascular risk, characterized by sustained endothelial dysfunction and vascular remodeling that are fundamental to the pathogenesis of CVD after HDP [38,39,40].
Wu et al. [41] in their systematic review and meta-analysis, established preeclampsia as a significant predictor of future cardiovascular morbidity and underscored the need for better predictive markers in postpartum care. Addressing this need, our study investigated the TyG index as a quantifiable metabolic indicator in women with prior HDP. To complement observational findings and strengthen causal inference, we further performed MR analysis. The IVW method revealed a significant positive causal association between the TyG index and overall CVD risk. Importantly, to address potential pleiotropy, we introduced BWMR; its results further supported a causal role of TyG‑related metabolic dysregulation in CVD pathogenesis. The concordance between longitudinal cohort analysis and genetic causal inference substantially strengthens the hypothesis that the TyG index is not merely a correlative marker but an active participant in postpartum CVD development, thereby solidifying its clinical relevance as a target for PPPM strategies.
In contrast to some prior studies in general populations that have reported non-linear associations between metabolic indices and CVD [42, 43], our analyses consistently identified linear dose–response relationships between TyG indices and postpartum CVD among women with prior HDP. This linearity, observed in both continuous and tertile-based analyses, reinforces the clinical utility of TyG indices for risk stratification. The consistency of findings across observational and genetic analyses (BWMR) strengthens causal inference. Notably, their predictive strength was particularly evident in subgroups often regarded as lower risk in routine practice, namely younger women (< 49 years; HR, 1.68 vs. 1.30 in older women), those normotensive at baseline (HR, 1.88 vs. 1.39 in hypertensive women), and non-obese individuals (HR, 1.52 vs. 1.40 in obese women). This pattern suggests that TyG indices may detect early, compensatory metabolic derangements, driven by unfavorable visceral fat distribution and low-grade inflammation [44, 45], before overt obesity or hypertension emerges, in line with the PPPM focus on identifying suboptimal health states amenable to early intervention. Notably, we observed consistent associations across age and obesity subgroups (all P < 0.05), aligning with findings from Hong et al. [46] in patients with cardiovascular-kidney-metabolic (CKM) syndrome. In contrast, no significant association was detected in the small diabetic subgroup (n = 76), which most likely reflects limited statistical power rather than a true null effect. This finding contrasts with the U-shaped relationship reported in diabetic populations by Liu et al. [43] and underscores the need for further research in this specific population.
Our findings reinforce the role of TyG indices as practical, low-cost tools for postpartum cardiovascular risk stratification. As continuous surrogate markers of insulin resistance and adverse visceral adiposity, TyG indices enable quantitative identification of subclinical cardiometabolic risk beyond traditional categorical classifications based solely on HDP status. The robust predictive value maintained throughout our extended follow-up period (6–14 years) further strengthens the clinical relevance of these findings, suggesting that metabolic alterations captured by TyG indices may represent enduring pathophysiological changes rather than transient postpartum adaptations. Regular TyG indices screening may enhance postpartum risk stratification, particularly among seemingly low‑risk women (younger, normotensive, non‑obese), a group in whom conventional risk‑based follow‑up is often limited despite accumulating evidence of elevated long‑term CVD susceptibility [47,48,49]. Women with adverse metabolic profiles may benefit from lifestyle interventions targeting glycemic control and visceral adiposity, strategies that have been shown to improve insulin sensitivity and cardiometabolic outcomes in postpartum and high‑risk populations [50], with pharmacological approaches considered for persistent cases [51]. Integrating TyG indices into structured postpartum monitoring protocols, beginning with early metabolic assessment, may facilitate timely and individualized intervention [41]. This strategy directly promotes the PPPM goal of shifting from reactive management to proactive, biomarker-informed prevention based on each woman’s biological profile. While these strategies require validation through interventional studies, they provide a foundation for evidence based, biomarker informed protocols to reduce cardiovascular risk in this vulnerable population.
Strengths and Limitations
This study has several strengths. It draws on a large, well-characterized longitudinal cohort to establish temporal relationships between TyG indices and postpartum CVD. A key methodological strength of this study lies in the integration of observational analysis with MR, particularly through the application of BWMR to reinforce causal inference, thereby providing a more comprehensive and multi‑layered evidence base. The consistent linear dose–response patterns observed across multiple TyG derivatives enhance the robustness and reproducibility of the findings. In addition, framing the analyses within a PPPM paradigm provides a clear translational pathway from epidemiologic evidence to clinical risk prediction, targeted prevention, and personalized postpartum care.
Limitations warrant consideration when interpreting our findings. First, reliance on self-reported HDP history without standardized obstetric confirmation may have introduced misclassification, likely biasing estimates toward the null. Second, metabolic parameters were measured at a single post-enrollment timepoint, limiting our ability to characterize detailed longitudinal trajectories of metabolic recovery or deterioration after pregnancy. Third, generalizability may be constrained by the characteristics of the UK Biobank cohort, including older recruitment age (37–73 years) and predominantly European ancestry, which may not fully reflect younger, more ethnically diverse postpartum populations. Finally, the lack of detailed data on placental pathology, body fat distribution, and longitudinal lipid profiles before, during, and after pregnancy restricts mechanistic interpretation. Despite these limitations, the large sample size and the robust, consistent associations we observed between TyG indices and long-term postpartum CVD risk underscore their potential as clinically relevant indicators of persistent metabolic dysfunction.
These limitations highlight the need for future prospective studies with longitudinal metabolic profiling from early pregnancy onwards in diverse, younger populations. Validating these findings in such cohorts and integrating them with placental pathology and detailed body composition data will be crucial to elucidate the complete trajectory and mechanisms linking HDP to future cardiometabolic risk.
Conclusion and expert recommendations in the framework of 3P medicine
In conclusion, in the framework of PPPM, our study demonstrates a clear, linear dose–response relationship between TyG indices and incident postpartum CVD in women with a history of HDP, supported by both observational and genetic causal evidence. TyG derivatives, particularly TyG-BMI, TyG-WC, and TyG-WHtR, provide effective risk stratification, even among women conventionally considered low risk, by revealing latent metabolic dysfunction rooted in the insulin resistance–visceral adiposity axis. Leveraging TyG indices could enhance early detection, facilitate risk stratification, and support primary prevention efforts for postpartum CVD. These observations support a shift away from uniform postpartum follow-up toward a stratified, biomarker-driven prevention strategy. Further research in diverse populations with standardized obstetric phenotyping and longitudinal assessment is warranted to better understand these relationships.
Predictive medical approaches
The core of predictive medicine lies in identifying individuals in a suboptimal health status or pre-disease state [28, 29, 52, 53]. HDP acts as a powerful metabolic stress test that unmasks underlying cardiometabolic vulnerability. Within the PPPM framework, the central predictive question is not merely who experienced HDP, but who exhibit persistent metabolic dysfunction after pregnancy. Our findings demonstrate that the TyG indices offer a quantitative means to answer this question, identifying women in a suboptimal health state long before clinical CVD appears [54]. After delivery, metabolic trajectories of women with a history of HDP diverge: some women recover to normal, while others maintain persistent dysfunction, potentially leading to irreversible pathophysiological changes and future clinical cardiovascular disease. Incorporating TyG indices into postpartum assessments enables early risk stratification and creates a critical window for timely intervention before overt postpartum CVD occurs.
Targeted prevention
Traditional preventive strategies often apply uniform interventions to all women with a history of HDP, overlooking fundamental differences in metabolic recovery. Under the guidance of the PPPM paradigm [52], TyG indices enable graded, risk-adapted prevention for stratifying metabolic risk in postpartum women, revealing not only fundamental biological variability but also distinguishing between metabolic recovery and persistent dysfunction. The causal evidence provided by MR analysis further strengthens the rationale for interventions targeting TyG‑associated metabolic pathways. Based on such stratification, preventive strategies should shift from a uniform approach to individualized management. Women with normal TyG profiles may benefit primarily from standard lifestyle counseling, whereas those with elevated indices, indicating ongoing metabolic impairment, should be prioritized for more intensive, targeted interventions. These may include structured, evidence-based programs focusing on diet, physical activity, and weight management to enhance insulin sensitivity, combined with closer monitoring of blood pressure, glucose, and lipid levels.
Personalized medicine
The core principle of personalized medicine is to translate biomarker discoveries into robust, actionable tools for clinical decision-making. Personalized care plans should be tailored to each woman’s TyG profile and broader risk context. For women with elevated TyG indices, especially those who are young, normotensive, or non-obese, clinicians should adopt a lower threshold for enhanced follow-up and earlier initiation of lifestyle or pharmacologic measures aimed at reducing insulin resistance and visceral adiposity. In this way, TyG-guided management transforms HDP from a purely historical risk factor into an actionable entry point for long-term cardiovascular health optimization. This evidence-based approach supports a shift in HDP management from empirical, one-size-fits-all strategies to personalized medicine, establishing a solid foundation for lifelong cardiovascular care in women with HDP and promoting the transition from reactive to predictive medical practice.
Contribution to the paradigm shift
Effectively identifying modifiable metabolic risk factors offers opportunities for implementing PPPM strategies in cardiovascular prevention for women with a history of HDP, thereby contributing to the extension of healthy lifespan. By applying the TyG indices, a simple and cost-effective biomarker, we have achieved three key shifts: quantitative risk prediction across a wide range of subclinical stages; targeted prevention during the critical postpartum period for women with ongoing metabolic vulnerability; and the design of individualized care plans based on each patient’s unique biological status rather than medical history alone. This approach promotes a transition from treating diseases after their onset to proactive prevention early in the postpartum period.
The TyG index provides a practical tool for implementing PPPM on a large scale among millions of women with a history of HDP. By transforming retrospective obstetric diagnoses into proactive, lifelong cardiovascular health management strategies, our study reframes HDP from a clinical challenge into an opportunity for early intervention and individualized prevention. Effective PPPM strategies underscore the immense potential and public health significance of metabolically informed cardiovascular disease prevention.

Comments (0)