
Remember me

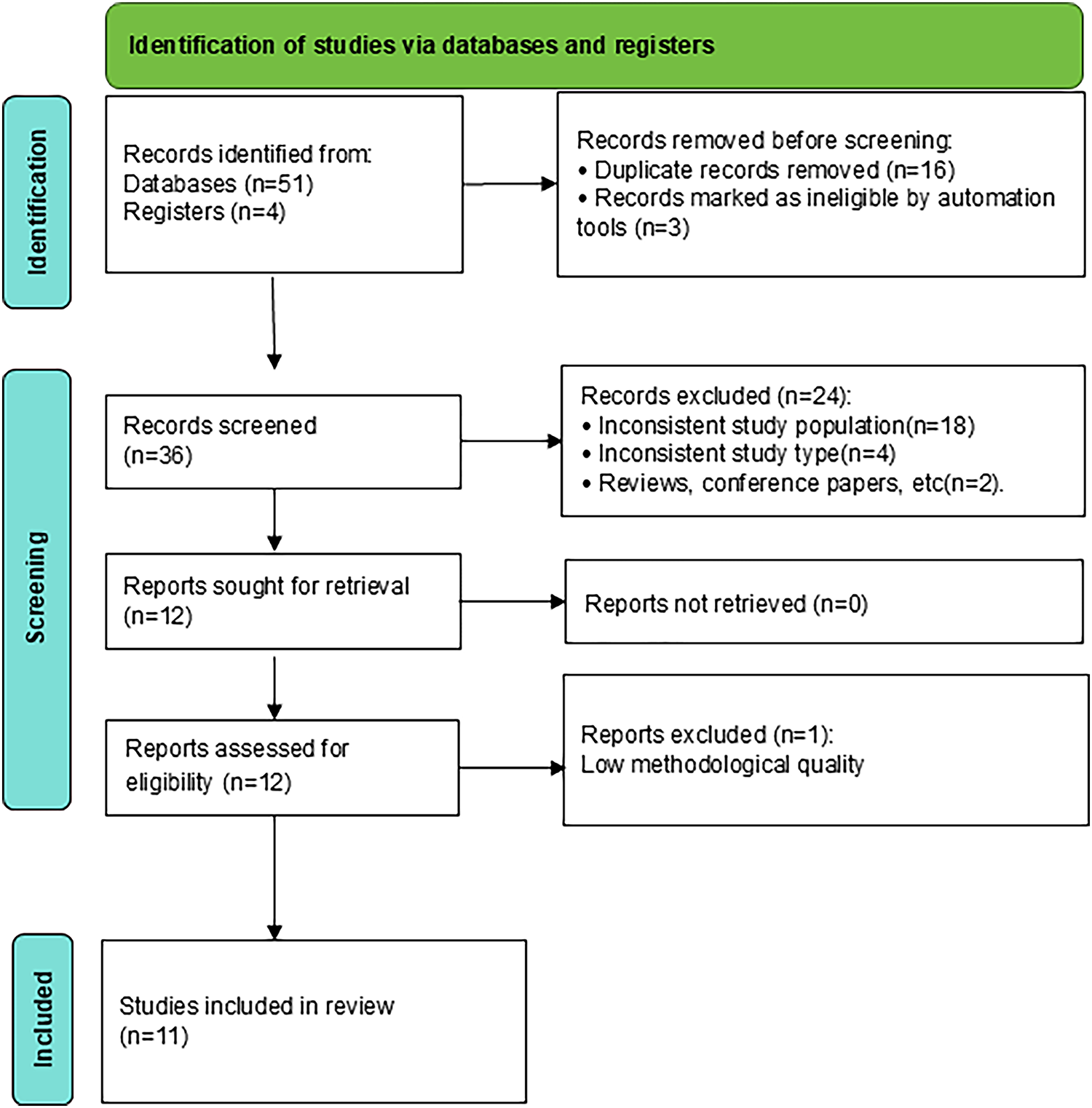
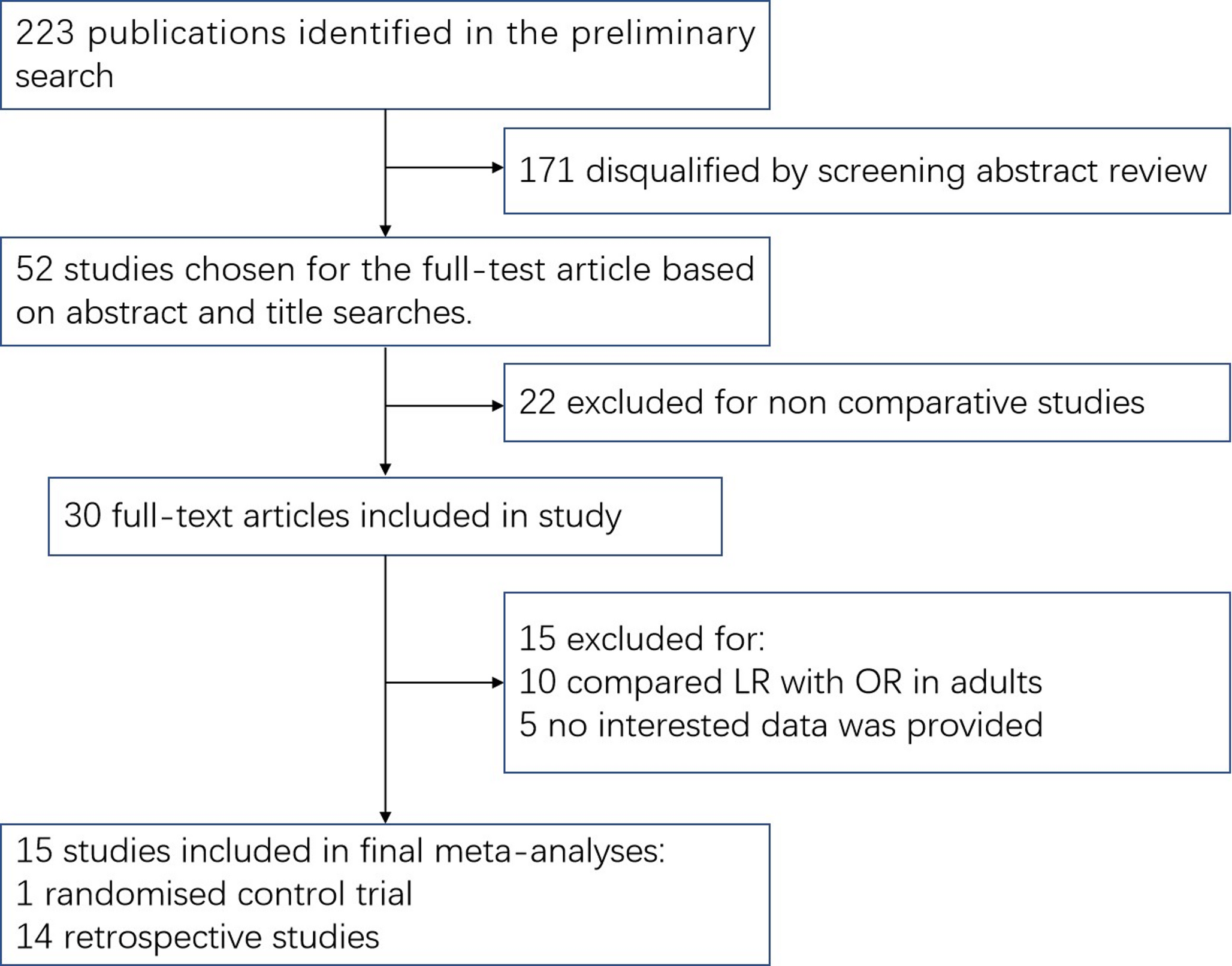
The systematic literature search yielded a total of records through the database search. Following the removal of duplicates, the remaining articles were evaluated based on their titles and abstracts. During the full-text screening step, we found that three studies were abstracts only, four studies were outside the review’s scope, and one study had incomplete data. Finally, nine studies that met eligibility criteria were included in the qualitative and quantitative synthesis [13,14,15,16,17,18,19,20,21], as illustrated in Fig. 1.
Fig. 1
Study characteristics A total of nine retrospective observational studies comparing lobectomy and segmentectomy for CLMs were included in the quantitative synthesis. The population primarily consisted of infants and young children, with mean ages ranging from 0.58 months to 12.7 years at the time of surgery. Across studies, the lobectomy group consistently included more patients than the segmentectomy group. Reported male proportions ranged between 48 and 63% in studies that provided sex-specific data. Most of them were conducted in China. Several studies reported that segmentectomy provided comparable short-term and mid-term outcomes to lobectomy, particularly in terms of postoperative complications, length of hospital stay, and pulmonary function recovery. Two studies indicated that segmentectomy was associated with better preservation of short-term pulmonary function, while long-term pulmonary function remained normal in both groups. However, one large pediatric series reported a higher incidence of persistent air leakage following segmentectomy. Overall, the collective evidence suggests that segmentectomy is a feasible lung-sparing alternative to lobectomy in selected pediatric patients with CLMs, without compromising short-term safety, as summarized in Table 1.
Table 1 Characteristics of included studiesQuality assessmentThe methodological quality of all included cohort studies was assessed using NOS. Overall, the studies demonstrated moderate to high methodological quality, with total NOS scores ranging from 7 to 9 stars. Most studies achieved the maximum score for selection, reflecting well-defined cohorts, reliable ascertainment of exposure through imaging and surgical records, and confirmation that outcomes were absent at baseline. Comparability scores were generally lower, as adjustment for confounders was limited in several studies, with only one multicenter propensity-matched study achieving full comparability. Outcome assessment was strong, with most studies employing objective outcome measurements, adequate follow-up durations, and low rates of loss to follow-up, as summarized in Table 2.
Table 2 Quality assessment of included cohort studies using the Newcastle–Ottawa scale (NOS)Outcome assessmentLength of hospital Stay (LOS)Meta-analysis was performed to assess the difference in LOS; the forest plot for LOS demonstrated no statistically significant difference between lobectomy and segmentectomy (MD = − 0.20, 95% CI [− 0.83 to 0.44], p = 0.547). Heterogeneity was high (I² = 80.7%), as shown in Fig. 2. Sensitivity analysis was performed by excluding the study by Cheng et al., which showed complete heterogeneity resolution, as shown in Figure S1 in the supplements.
Fig. 2
Forest plot of length of hospital stays
Funnel plot asymmetry testing showed no evidence of publication bias (Egger’s t = 0.83, p = 0.444), indicating strong stability of the LOS result, as seen in Figure S2 in the supplements.
lobectomy.
Operative (Surgery) timeA pooled meta-analysis of operative time revealed a statistically significant difference between surgical techniques, showing that lobectomy performed in a shorter time (MD = − 18.45, 95% CI [− 28.41 to − 7.64], p < 0.0001). Between-study heterogeneity was substantial (I² = 84.8%), as shown in Fig. 3. Sensitivity analysis was performed by excluding the study by Xi Huang et al., which helped reduce heterogeneity, with I² = 47%, as shown in Figure S3 in the supplementary materials.
Fig. 3
forest plot of surgery time
Publication bias assessment showed no significant bias (Egger’s t = − 65, p = 0.5526), as shown in Figure S4 in the supplements.
Chest tube removalWe found no statistically significant difference between the two groups regarding the time taken to remove chest tubes after surgery (MD = − 0.55, 95% CI [− 1.57 to 0.47], p = 0.2929). Between-study heterogeneity was high (I² = 95.9%), as shown in Fig. 4. Sensitivity analysis was performed by excluding the study by He et al., which helped reduce heterogeneity, with I² = 60.2%. Additionally, a change in the context of results following sensitivity analysis supports the association between lobectomy and lower time, as shown in Figure S5 in the supplementary materials.
Fig. 4
forest plot of chest tube removal
Publication bias assessment approached but did not reach significance (Egger’s t = − 2.38, p = 0.063), suggesting a possible small-study effect for this outcome (Figure S6 in the supplements).
Pulmonary function outcomesAcross all pulmonary function indices, the forest plots demonstrated no statistically significant differences between lobectomy and segmentectomy. The confidence intervals overlapped neutral effect thresholds in all comparisons, indicating comparable postoperative lung function preservation between the two surgical approaches.
Tidal volume (VT)No significant difference was observed between lobectomy and segmentectomy (MD = − 0.06, 95% CI [− 0.27 to 0.14], p = 0.5337). There was low heterogeneity with I² = 11%, as seen in Figure S7 in the supplements.
Inspiratory time to expiratory time ratio (TI/TE)There was no statistically significant difference between the two surgical techniques (MD = 0.01, 95% CI [− 0.06 to 0.08], p = 0.8152). There was no heterogeneity, as indicated by an I² value of 11%, as shown in Figure S8 in the supplements.
Time to peak tidal expiratory flow to total expiratory time ratio (TPTEF/TE)Pooled results showed no significant difference (MD = 2.34, 95% CI [− 2.44 to 7.12], p = 0.3375). There was high heterogeneity, as indicated by an I² value of 95.1%, as shown in Figure S9 in the supplements.
Volume of peak expiratory flow to expired volume ratio (VPEF/VE)Similarly, no significant difference was identified (MD = 1.58, 95% CI [− 1.73 to 4.88], p = 0.3497). There was high heterogeneity, as indicated by an I² value of 93.3%, as shown in Figure S10 in the supplements.
Overall postoperative complicationsThe pooled analysis of overall complications showed no statistically significant difference between groups, as indicated in the forest plot (OR = 0.96, 95% CI [0.58–1.61], p = 0.8827). Heterogeneity for complications was low (I² = 28.3%), as shown in Fig. 5. Sensitivity analysis was performed by excluding the study by Cheng et al., which helped resolve heterogeneity, with an I² value of 0%, as shown in Figure S11 in the supplements.
Fig. 5
Forest plot of complication rate
However, publication bias was detected for this outcome (Egger’s t = − 3.89, p = 0.008), indicating that the pooled complication effect may be influenced by small-study effects or selective reporting, as seen in Figure S12 in the supplements.
PneumoniaTwo studies were included in this analysis; the forest plot analysis showed no statistically significant difference in postoperative pneumonia between lobectomy and segmentectomy (OR = 0.47, 95% CI [0.07–3.27], p = 0.4427). There was no observed heterogeneity, as seen in Figure S13 in the supplements.
BleedingThree studies examined the incidence of bleeding, showing no significant intergroup difference (OR = 2.96, 95% CI [0.38–22.92], p = 0.2989). Low heterogeneity was observed (I² = 25.9%), as shown in Figure S14 in the supplementary materials. Sensitivity analysis was performed by excluding the study by Polites et al., which resolved heterogeneity, as shown in Figure S15 in the supplementary materials.
PneumothoraxThree studies examined the incidence of pneumothorax, showing no significant intergroup difference (OR = 1.22, 95% CI [0.36–4.12], p = 0.7483). No heterogeneity was observed (I² = 0%), as shown in Figure S16 in the supplementary materials.
InfectionPostoperative infection rates showed a statistically significant difference between lobectomy and segmentectomy across all included studies (OR = 1.06, 95% CI [0.10–10.68], p = 0.924). No heterogeneity was observed (I² = 0%), as shown in Figure S17 in the supplementary materials.
Pleural effusionNo statistically significant difference was observed in pleural effusion rates (OR = 0.31, 95% CI [0.03–2.99], p = 0.3125). No heterogeneity was observed (I² = 0%), as shown in Figure S18 in the supplementary materials.
Air leakageThree studies examined the incidence of air leakage, showing a significant difference between the two groups, favoring lobectomy (OR = 0.30, 95% CI [0.11–0.83], p = 0.0201). Low heterogeneity was observed (I² = 21.6%), as shown in Figure S19 in the supplementary materials. Sensitivity analysis was performed by excluding the study by Joo et al., which resolved heterogeneity and altered the context of the results, showing no difference between the groups, as shown in Figure S20 in the supplementary materials.
Comments (0)