Patients
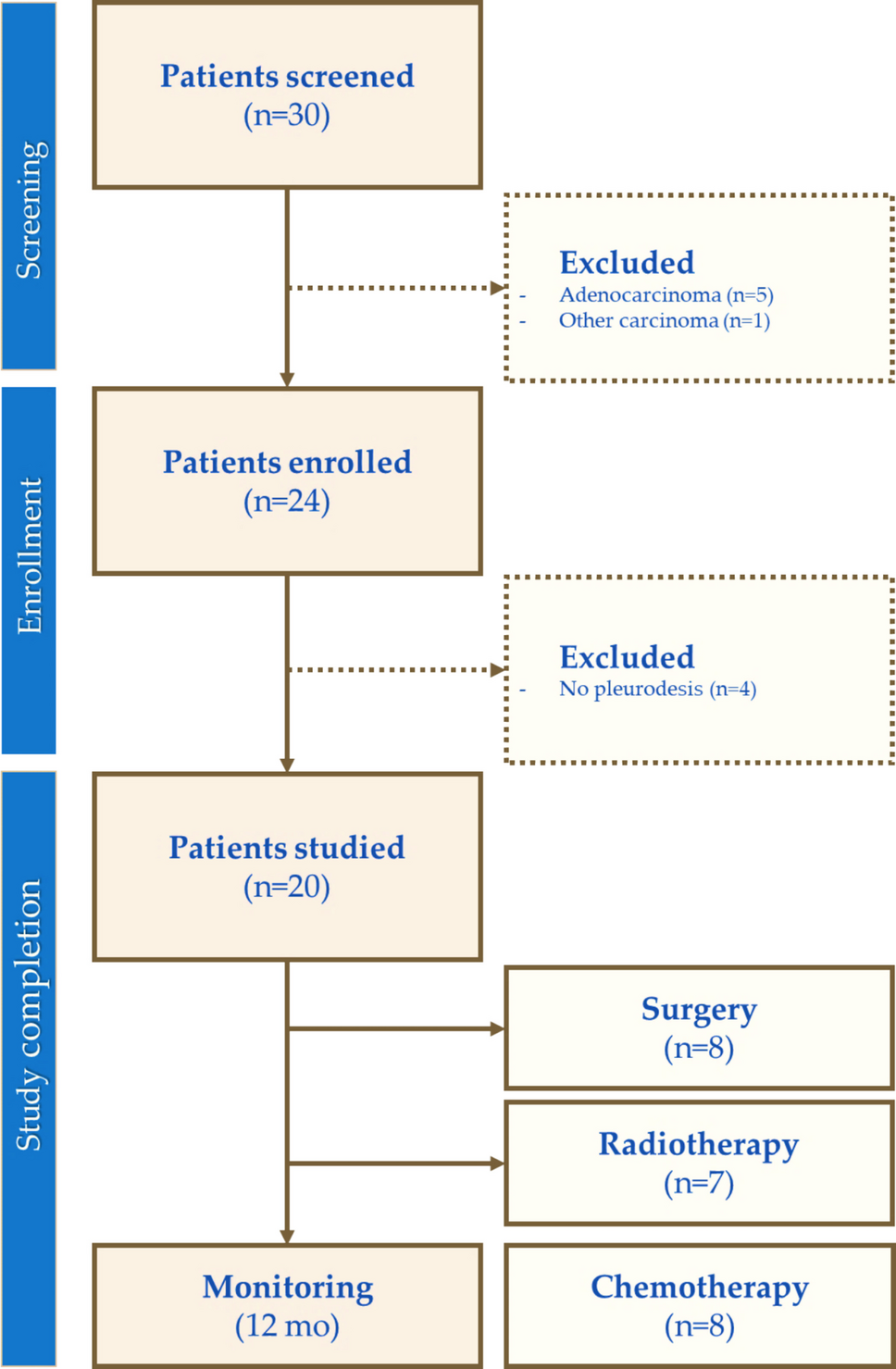
Eleven patients (median age 69 years; range 36–79; 5 male) were enrolled in a prospective, single-centre observational clinical trial (NCT03951142). The trial was approved by the National Research Ethics Committee and the Institutional Review Board (approval number 2017/1875). All patients provided written informed consent prior to participation. Eligible patients were those (I) aged ≥ 18 years and newly diagnosed with a new BM originating from NSCLC, (II) measured in at least one dimension as ≥ 5 mm on contrast-enhanced T1-weighted (ce-T1w) magnetic resonance imaging (MRI), and (III) eligible for radiotherapy and with a life expectancy of longer than 6 weeks. Recruitment occurred during routine clinical visits. All participants were referred for SRS as part of their treatment plan. Patient characteristics are presented in Table 1.
Table 1 Patient characteristicsPET/CT Acquisition and Image Reconstruction
[18F]PSMA-1007 (2.5 MBq/kg) was injected intravenously, and the patients were scanned dynamically over the head using a dual-time-point (DTP) protocol at 0–30 min and 80–95 min post-injection. The exam concluded with a 2.5-min per bed full-body PET/CT scan. Scanning was performed on a Discovery MI PET/CT system (GE Healthcare, Milwaukee, WI, USA). The first exam occurred before SRS, and the second exam 12 weeks after the first exam. Notably, two patients (patients 1 and 4) underwent SRS two days prior to the first exam. The median injected activity of [18F]PSMA-1007 was 195.3 MBq (range 189.8—220.2 MBq) for the first exam and 197.9 MBq (range 195.0–219.1 MBq) for the second exam. Patients were positioned head-first supine with arms alongside their bodies. Brain PET images were reconstructed using Q.Clear (time-of-flight, point-spread function correction, 256 × 256 matrix, 30 cm field-of-view) with β-factor of 900, based on an in-house phantom study [13]. The whole-body PET data were reconstructed using the Q.Clear reconstruction algorithm with β-factor of 600. Dynamic PET data were reconstructed into 35 frames of variable durations (18 × 10 s, 6 × 30 s, 4 × 1 min and 7 × 5 min), and were corrected for radioactive decay, dead time, attenuation, randoms and scattering. A low-dose CT (120 kVp, 35 mA, revolution time 1, pitch 0.98, slice thickness 0.625) was used for attenuation correction. In addition, a diagnostic non-contrast-enhanced CT was acquired at the second time-point (120 kVp, 119 mA, revolution time 0.6, pitch 0.98, slice thickness 0.625).
Image Processing and Analysis
Image analysis was conducted using PMOD 4.0 (PMOD Technologies LLC, Zurich, Switzerland). To correct for patient motion, a rigid registration method was applied between frames. For the first time point, the reference image was the average uptake over the initial two minutes. For the second time point, the first five-minute frame served as the reference. A combined dynamic PET dataset covering 0–95 min post-injection was created by registering the CT images from the two time points using a rigid matching technique with normalized mutual information.
The BMs were segmented using a static image derived from the averaged uptake between 85- and 95-min post-injection. An individual segmentation threshold was determined based on the average signal from the blood background in the bilateral internal carotid arteries (ICAs). The threshold for each patient is shown in Table 2. The ICAs were segmented using a threshold of 50% of the maximum signal intensity from the early blood pool image (the first minute post-injection). The lung tumour was segmented using a threshold of 40% of the maximum signal within the tumour, based on previous [18F]FDG PET/CT studies [14]. SUVpeak and biological tumour volumes (BTV) were calculated for both the lung tumour and BM VOIs. SUVpeak was defined as the mean SUV of the five voxels with highest values within the VOI. Although SUVmax is frequently reported, SUVpeak was used in this work, as it better reflects the tracer uptake and is less sensitive to noise or single-pixel outliers. To assess the heterogeneity of tracer uptake, the coefficient of variance (CoV) was calculated by dividing the standard deviation by the mean SUV in the VOI.
Table 2 Tumour [18F]PSMA-1007 imaging characteristicsThe arterial input function (AIF) was approximated using an image-derived input function (IDIF) extracted using the time-activity curves (TACs) from the ICAs. Given that the ICA diameter (~ 5 mm) [15] approaches the spatial resolution limit of clinical PET systems, the IDIF is subject to partial-volume effects, leading to underestimation of the true activity concentration. Therefore, a recovery coefficient (RC) was applied. The RC was derived from an in-house phantom experiment performed under identical scanner, acquisition, framing and reconstruction conditions (including Q.Clear β-values) [13], and calculated as the ratio between measured and true activity concentration in vessel-equivalent structures. The resulting RC (0.59) was applied as a scaling factor to the IDIF, yielding an approximate 70% increase in arterial activity estimates.
Pharmacokinetic modelling was performed using linear Patlak graphical analysis to estimate the net influx rate constant (Ki) [16]. TACs were generated for the BMs using the average values in the segmented VOIs. A normalized time (t*) of 15 min was applied to ensure steady-state conditions. The Patlak model was selected due to the relatively slow pharmacokinetic profile of [18F]PSMA-1007 [17] observed in the 95-min acquisition window used in this study, which is consistent with prior findings in prostate cancer [18, 19]. The Patlak model provides a robust estimation of Ki in comparison to the microparameters obtained from traditional compartment models [20]. In particular, previous work has demonstrated that ICA-derived IDIFs in combination with the Patlak model provide a reliable estimation of Ki [21].
Image Evaluation and Treatment Response Assessment
A board-certified radiologist evaluated the response to SRS treatment using the Response Assessment in Neuro-Oncology Brain metastases (RANO-BM) criteria [22] for the seven patients who underwent both scans, as well as the number of BMs from the radiological images. The RANO-BM criteria categorize treatment responses into four types: complete or partial response, stable disease or progression, based on (preferably) ce-T1w or contrast-enhanced CT. The MR exams were not acquired as part of our study protocol but rather obtained from clinical follow-up. The time interval between MRI and PET is presented in Table 1. For two patients, no MR images were available; therefore contrast-enhanced CT images were used as an alternative. One patient passed away shortly after the second [18F]PSMA-1007 scan and had no MRI or CT scan and was therefore not assessed with the RANO-BM criteria. For two of the patients an [18F]FDG PET examination of their primary lung tumour, taken as part of clinical routine practice within one month preceding their first [18F]PSMA-1007 exam, was compared to the [18F]PSMA-1007 scan by a nuclear medicine specialist.
Statistical Analysis
Statistical analysis was performed with Statistical Package for the Social Sciences (SPSS) version 30.0.0.0. (IBM Corporation, New York, USA). Normality of the data was tested with Kolmogorov–Smirnov Z-test for continuous variables. All data were reported as median and range. Correlation between CoV, SUVpeak and Ki were assessed using the Spearman correlation. A p-value < 0.05 was considered statistically significant.



Comments (0)