According to a systematic review by Godbole et al. of 160 cases published in 2019, PTTM is most commonly associated with gastric adenocarcinoma, accounting for 59% of cases, followed by lung cancer and breast cancer [2]. To better characterize PTTM associated with prostate cancer, we reviewed previously reported cases and summarized their clinical characteristics (Table 1). To date, only six cases of prostate cancer–associated PTTM have been reported, and ante-mortem diagnosis was achieved in only one case [1, 3,4,5,6,7]. Imakura et al. reviewed 20 cases of PTTM diagnosed ante-mortem across all malignancies [8]. The longest survival previously reported was 32 months after diagnosis in a patient with breast cancer, as described by Takahashi et al. [9]. Notably, the present patient has survived for more than 10 years since disease onset. This represents the longest survival reported to date and may be attributable to minimally invasive diagnostic strategies and early therapeutic intervention.
The pathophysiology of PTTM involves fibrocellular intimal thickening of the pulmonary arteries induced by vascular remodeling mediated by tumor-derived growth factors such as vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and osteopontin, leading to increased pulmonary vascular resistance and progressive pulmonary hypertension. In addition, activation of the coagulation cascade with intravascular thrombosis and fibrin deposition further accelerates the progression of pulmonary hypertension [2, 10, 11]. A characteristic feature of the present case was the rapid deterioration of respiratory status shortly after prostate biopsy. Although direct evidence is limited, several reports have described PTTM progression in association with invasive procedures, including a fatal postoperative case after lung cancer resection [12] and acute respiratory worsening following surgery for a perianal abscess in a patient later diagnosed with PTTM [13]. These observations suggest that invasive interventions may promote tumor cell embolization to the pulmonary microvasculature, unmasking or exacerbating subclinical microangiopathy, and warrant careful clinical decision-making when PTTM is suspected.
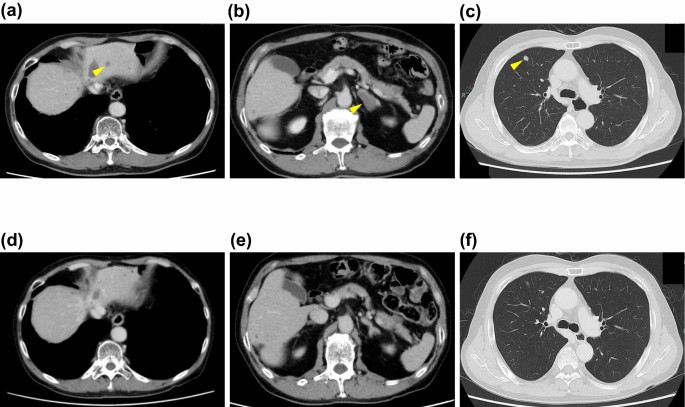
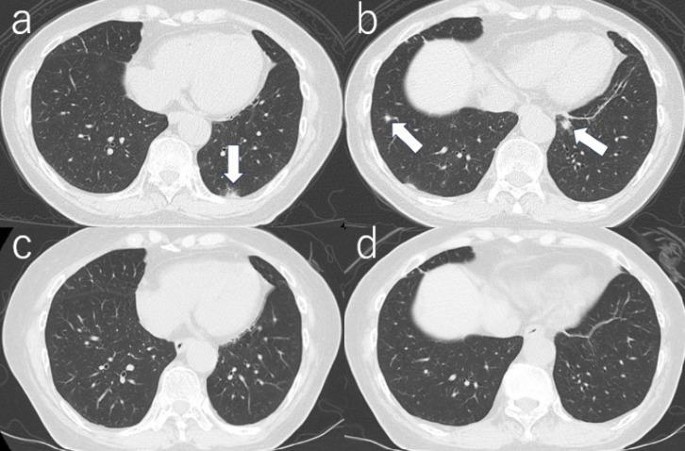
Chest CT findings in PTTM are nonspecific and may include diffuse ground-glass opacities, small nodules, and tree-in-bud–like patterns, whereas contrast-enhanced CT typically shows no macroscopic pulmonary embolism. Pulmonary perfusion scintigraphy typically demonstrates multiple, symmetric, and peripheral perfusion defects. Although bronchoscopic or CT-guided lung biopsy is considered a definitive diagnostic modality, the invasive nature of these procedures often precludes their use in patients with impending respiratory failure. In contrast, pulmonary artery aspiration cytology obtained during right heart catheterization is a less invasive diagnostic approach and may be particularly useful in critically ill patients [2]. Tashima et al. demonstrated the potential utility of FDG-PET/CT in detecting findings suggestive of pulmonary hypertension and right heart strain in a patient with PTTM, supporting its role as an adjunctive diagnostic modality [14]. However, that report described PET findings only after clinical deterioration had occurred. In contrast, the present case demonstrates that FDG-PET/CT can suggest the presence of PTTM prior to overt respiratory failure and directly influenced early therapeutic decision-making.
Table 1 Previously reported cases and the present case of pulmonary tumor thrombotic microangiopathy associated with prostate cancerCurrently, there is no established treatment for PTTM itself, and the prompt initiation of therapy targeting the underlying malignancy remains the cornerstone of management. Imatinib, a PDGF receptor tyrosine kinase inhibitor, has been reported to be effective in selected cases of PTTM associated with PDGF overexpression [15, 16]. In addition, several case observations have suggested that the inhibition of VEGF signaling may attenuate the clinical manifestations of PTTM, implying that anti-VEGF therapy could have potential therapeutic utility in selected patients [17, 18]; however, further investigation is required to establish the role of these signal inhibitors. Notably, in many reported cases, even when an ante-mortem diagnosis is achieved, rapidly progressive respiratory failure often precludes the initiation of systemic anticancer therapy [2]. In the present case, rapid initiation of hormonal therapy, which was considered to have minimal direct adverse effects on cardiopulmonary hemodynamics, may have contributed to disease stabilization and survival. Furthermore, the fact that PTTM developed in the setting of previously untreated, hormone-sensitive prostate cancer, rather than castration-resistant disease, likely contributed to the favorable therapeutic response and successful rescue in this patient.
In conclusion, we reported a case of PTTM associated with metastatic prostate cancer in which early clinical suspicion based on FDG-PET/CT findings enabled prompt initiation of cancer-directed therapy prior to definitive diagnosis by pulmonary artery aspiration cytology, resulting in successful rescue and long-term survival exceeding 10 years. This case highlights that early clinical suspicion, minimally invasive diagnostic strategies, and prompt treatment of the underlying malignancy may enable successful rescue even in this otherwise rapidly fatal condition.

Comments (0)