
Remember me
In recent years, the incidence of endometrial and ovarian cancers has increased in Japan [1]. Synchronous endometrial and ovarian cancer (SEOC) accounts for approximately 5% of endometrial cancers and 10% of ovarian cancers [2]. SEOC typically carries a favorable prognosis [3] and has traditionally been regarded as a distinct clinical entity rather than a manifestation of metastatic disease [4]. However, recent next-generation sequencing (NGS) studies have shown that most SEOCs are not independent primary tumors, but rather represent metastasis from endometrial cancer to the ovary [3, 5]—except in cases associated with Lynch syndrome [6].
Fertility-sparing treatment is an established option for well-selected cases of grade 1 endometrioid carcinoma confined to the endometrium, particularly in young women [7, 8]. Similarly, it is considered acceptable for stage IA mucinous and endometrioid ovarian carcinomas with low-grade histologic features [7, 9]. Reported pregnancy rates following fertility-sparing treatment range from 25 to 66% for endometrial cancer and 30 to 54% for ovarian cancer. Among patients actively attempting conception, the rates are even higher—93.3% for endometrial cancer and 89% for ovarian cancer [10]. Despite these favorable outcomes, reports of fertility-sparing treatment for SEOC—in which both tumors independently fulfill the criteria for conservative management—remain extremely limited. As a result, the feasibility and reproductive outcomes of such treatment in SEOC remain uncertain.
In this study, we report a rare case of SEOC in a young woman who achieved two successful spontaneous pregnancies and deliveries following fertility-sparing treatment. We also review the existing literature to provide further insight into the feasibility and outcomes of fertility preservation in SEOC. We believe this case offers valuable evidence to inform future guidelines on fertility-sparing management of SEOC.
Case reportThe patient was a 26-year-old nulligravid woman with a history of irregular menstrual cycles since menarche at age 12. She was 158 cm tall, weighed 49 kg, and had a body mass index (BMI) of 19.6. Her medical history included a left salpingectomy at age 13 due to torsion of a left tubal cyst. No significant family history of malignancy was identified among first- or second-degree relatives.
She initially presented to a local clinic with abnormal vaginal bleeding. Transvaginal ultrasound revealed endometrial thickening and a left ovarian tumor with solid components. She was referred to our institution for further evaluation. An endometrial biopsy revealed grade 1 endometrioid carcinoma. Pelvic contrast–enhanced magnetic resonance imaging (MRI) showed endometrial thickening measuring 3 cm (Figs. 1A and B) with restricted diffusion (Fig. 1C), while preservation of the junctional zone suggested that the tumor was confined to the endometrium. The left ovary was cystically enlarged to 5 cm and contained solid components (Figs. 1D–F). Chest–abdominal contrast–enhanced computed tomography (CT), as well as positron emission tomography–CT (PET–CT), revealed no lymph node involvement or distant metastasis. Complete endometrial curettage, laparoscopic left adnexal resection, and partial omentectomy were performed. Intraoperative findings revealed that the left fallopian tube had already been removed, and no abnormalities were observed in the right adnexa or on the uterine serosa. The ovarian tumor was resected intact via a 7-cm laparotomy without rupture.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Pelvic magnetic resonance imaging findings at initial presentation. (A, B) Sagittal and axial T2-weighted images showing endometrial thickening (arrowheads). (C) Diffusion-weighted image showing restricted diffusion in the thickened endometrium (arrowhead), consistent with malignancy. (D–F) Axial T2-weighted, contrast-enhanced T1-weighted, and diffusion-weighted images, respectively, showing a left ovarian mass with cystic and solid components (arrowheads). The junctional zone is preserved, and no evidence of extrauterine or metastatic spread is observed
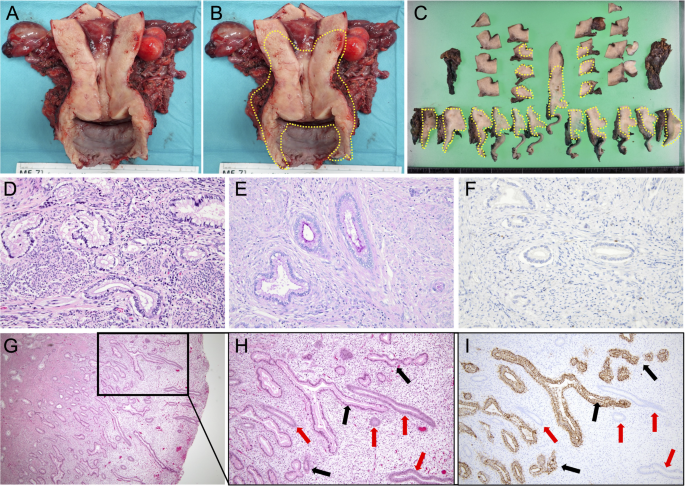
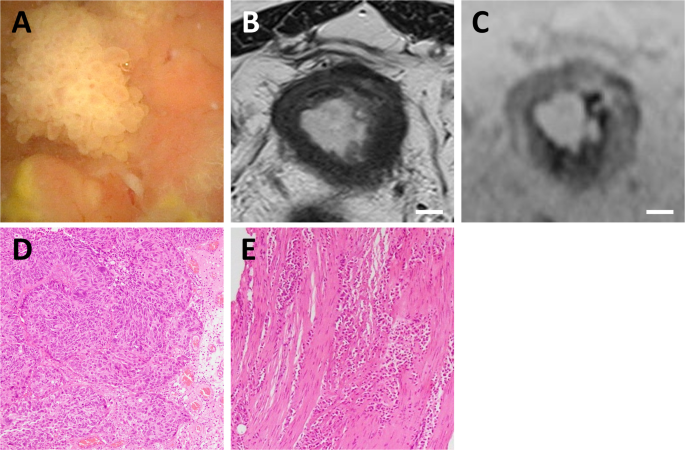
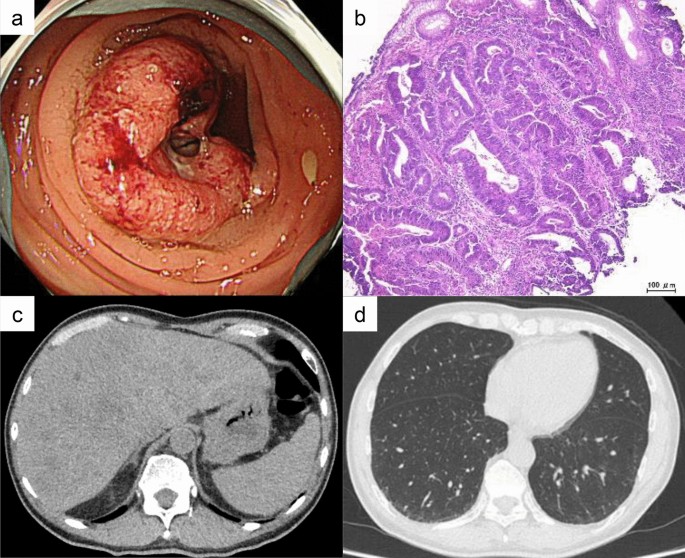
Postoperative pathological examination of the endometrial specimen confirmed grade 1 endometrioid carcinoma (Fig. 2A). The ovarian tumor was likewise diagnosed as grade 1 endometrioid carcinoma (Fig. 2B). No metastasis was found in the omentum, and peritoneal cytology was negative. The diagnostic criteria for distinguishing ovarian metastasis of endometrial cancer from SEOC include: (1) small ovarian size (< 5 cm), (2) bilateral ovarian involvement, (3) deep myometrial invasion, (4) lymphovascular space invasion, and (5) fallopian tube involvement [4]. In this case, only criterion (1) was met. Therefore, the diagnosis was SEOC, with stage IA endometrial cancer (The International Federation of Gynecology and Obstetrics (FIGO) 2008) and stage IA ovarian cancer (FIGO 2014). Although tumor-specific genetic or mutational analyses were not performed, the diagnosis of synchronous primary tumors was established based on widely accepted clinicopathological criteria, including those proposed by Ulbright and Roth and later modified by Scully. In the present case, both tumors were confined to their respective organs without lymphovascular space invasion, fallopian tube involvement, or peritoneal dissemination, supporting independent primary origins rather than metastatic disease. While recent studies have highlighted the potential role of molecular analyses in distinguishing synchronous primary tumors from metastatic disease, the clinicopathological findings in this case were considered sufficient to support the diagnosis of SEOC.
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Histopathological findings of endometrial and ovarian tumors. Both tumors were diagnosed as grade 1 endometrioid carcinoma (A: endometrial lesion; B: ovarian lesion, H&E staining)
Given the patient’s young age at diagnosis, Lynch syndrome was considered. Immunohistochemistry for mismatch repair (MMR) proteins (MLH1, MSH2, MSH6, and PMS2) showed preserved expression of all markers. Additionally, germline NGS of peripheral blood detected no pathogenic variants. Multiplex ligation-dependent probe amplification (MLPA) analysis of BRCA1, BRCA2, MLH1, MSH2, and EPCAM also revealed no germline mutations.
At the time of surgery, only one case of fertility–sparing treatment for SEOC had been reported [11]. However, due to the patient’s strong desire to preserve fertility, definitive surgery was deferred. Instead, conservative management was initiated with medroxyprogesterone acetate (MPA) at 600 mg/day for 26 weeks. Complete remission was confirmed by total endometrial curettage performed under general anesthesia, demonstrating no residual carcinoma or atypical hyperplasia. Pelvic MRI and chest–abdominal CT confirmed the absence of residual disease or distant metastasis. MPA therapy was concluded as planned. Following treatment completion, endometrial biopsy was performed every 3–6 months, and thoracoabdominal CT was conducted annually as part of oncologic surveillance. The patient subsequently received six cycles of progesterone withdrawal therapy, each resulting in withdrawal bleeding. Treatment was discontinued in accordance with the patient’s desire to conceive. Two months later, she spontaneously conceived. The pregnancy progressed uneventfully, and she delivered a healthy female infant vaginally at 40 weeks and 3 days of gestation. The newborn weighed 2,892 g, with Apgar scores of 8 and 10 at one and five minutes, respectively.
Follow-up endometrial biopsies and CT revealed no evidence of recurrence. Two years and two months after the first delivery, the patient spontaneously conceived again. The second pregnancy also progressed without complications, resulting in a vaginal delivery at 39 weeks and 2 days. The second newborn, also female, weighed 3,000 g with Apgar scores of 8 and 10 at one and five minutes, respectively. No obstetric complications, including placenta accreta spectrum or excessive hemorrhage, were observed in either pregnancy, and placental histopathological examination was not performed.
The patient remains committed to fertility preservation and has not undergone hysterectomy. She has shown no signs of recurrence during the six years since completing MPA treatment.
Comments (0)