
Remember me

Baseline and disease characteristics for the ICC (n = 103) and HCC (n = 377) cohorts are summarised in Table 1. Additional information is available in Supplementary Table 1.
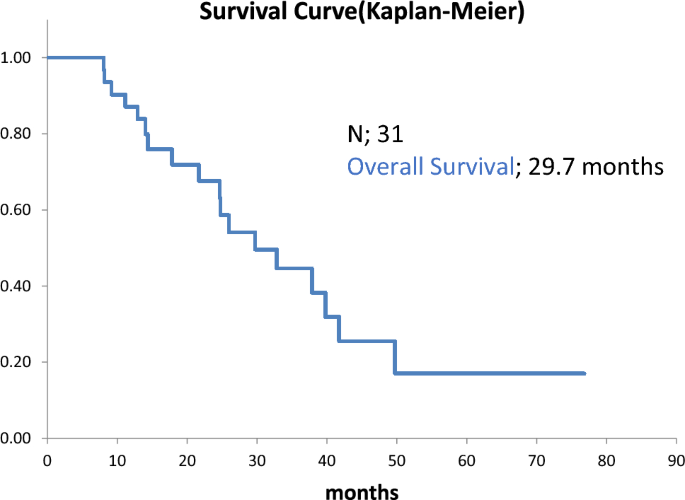
Table 1 Patient and disease characteristics by indicationICCMedian APRI was 0.5 (interquartile range [IQR]: 0.3–0.8). More than half of the patients (58.3%) had received prior systemic therapy (Table 1). 34 (33%) and 69 (67%) patients had APRI ≤ 0.4 and APRI > 0.4, respectively; and 74 (72%) and 29 (28%) had APRI ≤ 0.7 and APRI > 0.7, respectively (Fig. 1). For individuals with ICC, APRI > 0.4 showed a significant correlation with shorter OS (p = 0.0056; Fig. 1A).
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier curves on the effect of APRI cut-offs on survival. A ICC APRI cut-off 0.4. B HCC APRI cut-off 0.4. C ICC APRI cut-off 0.7. D HCC APRI cut-off 0.7. Overall Survival of ICC (A and C) and HCC (C and D) with APRI cut-offs 0.4 (A and B) and 0.7 (C and D)
After propensity score matching, a multivariable analysis was performed to assess the potential impact of other factors (Table 2). In the ICC cohort, compared to single tumours, having 2–5 tumours (1.04–5.19, p = 0.039), > 5 tumours (1.09–5.71, p = 0.031) and uncountable tumours (1.57–6.86, p = 0.002) were correlated with shorter OS.
Table 2 Multivariable analysis by indicationTo evaluate the differences between body surface area (BSA) and modified BSA (mBSA) as a broad strategy for calculating approximate dose and personalised models, dosimetry methods were assessed for the different cut-offs using both the empirical BSA/mBSA method and the more personalised partition model. OS differed by APRI threshold when BSA/mBSA was used, with higher APRI (> 0.4) associated with poorer outcomes (Supplementary Fig. 1A). In contrast, under partition model OS differences were not shown (Supplementary Fig. 1B). These results should be interpreted with caution based on the strong correlation between dosimetry and tumour spread (Supplementary Table 2).
Sensitivity analyses including ALBI grade as a marker of liver function were performed. In ICC patients, APRI > 0.4 remained independently associated with worse OS (HR 2.58, 95% CI 1.42–4.71, p = 0.002), indicating that the prognostic value of APRI was not explained by liver function alone (Supplementary Tables 3 and 4).
HCCHalf of the patients (52.5%) had intermediate stage BCLC-B, and 9.8% had received prior systemic therapy. Median APRI was 0.8 (IQR: 0.4–1.4) (Table 1). 84 (22.3%) and 293 (77.7%) patients had APRI ≤ 0.4 and APRI > 0.4, respectively; and 169 (44.8%) and 208 (55.2%) had APRI ≤ 0.7 and APRI > 0.7, respectively (Fig. 1). APRI > 0.7 showed a significant correlation with shorter OS compared to patients with APRI ≤ 0.7 (p = 0.0055; Fig. 1D).
Results from the multivariable analysis showed that extrahepatic disease (0.97–2.28, p = 0.066) and main PVT (1.41–4.09, p = 0.001) were correlated with shorter OS. Right-lobe tumour location (0.32–0.79, p = 0.003) was associated with longer survival in the HCC cohort (Table 2).
Similar to the ICC group, OS differed by APRI threshold when BSA/mBSA was used, with higher APRI (> 0.7) associated with poorer outcomes (Supplementary Fig. 1C). These survival differences were not observed under partition model (Supplementary Fig. 1D).
In HCC patients the association between APRI > 0.7 and OS lost statistical significance after adjustment for ALBI grade (HR 1.21, 95% CI 0.80–1.83, p = 0.361), suggesting that the effect of APRI in this population may largely reflect underlying liver dysfunction (Supplementary Table 4).
Comments (0)