
Remember me

Gastrointestinal cancer is a malignancy of the gastrointestinal tract with a high global morbidity and mortality [1]. Studies have confirmed that gastrointestinal tumorigenesis is closely related to modifiable risk factors [2], such as dietary patterns, physical activity, and smoking and drinking status. Changes in these factors can reduce the risk of tumorigenesis [3,4]. Effective interventions for external factors in cancer control can alleviate disease burden [5]. Therefore, research on gastrointestinal tumorigenesis-associated external factors is necessary to develop primary prevention strategies to reduce morbidity.
Diet plays a crucial role in tumorigenesis. A large body of evidence has demonstrated that a high intake of plant foods and a low intake of meat are associated with a reduced incidence of gastrointestinal malignancies [6–11]. Increase intake of plant foods, such as fruits, vegetables, whole grain cereals, and legumes, is associated with gastrointestinal malignancy-preventive effects [4,6,11–14]. Contrarily, a high intake of red and processed meats is associated with an increased risk of gastrointestinal tumorigenesis [10,11,15,16]. Therefore, the risk of gastrointestinal cancers seems to be associated with the intake proportion of plant foods and meat. Vegetarian diets refer to pure-plant-food diets without the intake of any kind of meat. Some prospective studies have suggested that vegetarian diets may reduce the risk of colorectal cancers [17,18]. In addition, a recent meta-analysis on the relationship between plant-based diets and the risk of digestive system cancers was published [19], although not optimally conducted because it combined a large number of different plant-based diets in the same analysis. Evidence-based exploration of the association between pure-plant-food diets and the risk of various types of gastrointestinal cancers is lacking. Moreover, the popularity of vegetarian diets varies widely in different parts of the world [20].
The aim of this systematic review was to summarize the study results on the correlation between vegetarian diets and the risk of gastrointestinal cancers (cancer incidence) to elucidate the effects of vegetarian diets on gastrointestinal tumorigenesis in different populations.
MethodsThis study was conducted in strict accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 [21], and the study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; Registration No. CRD42022310187).
Search strategyPubMed, Embase, Cochrane Library, and Web of Science databases were searched from their inception until 9 August 2022. The language of publication was restricted to English. Search items were designed based on the combination of medical subject headings (Mesh) and free words, which mainly included ‘diet, vegetarian’, ‘gastrointestinal neoplasms (containing esophageal, gastric, and colorectal neoplasms)’, and ‘cohort studies or case-control studies’. Reference lists of articles with similar topics were manually searched for potentially eligible studies. A detailed search strategy is provided in Appendix 1, Supplemental digital content 1, https://links.lww.com/EJGH/A915.
Inclusion and exclusion criteria Inclusion criteria Types of participants: All individuals recruited and assessed in the study, with or without gastrointestinal cancers. Types of exposure: Vegetarian diets, defined as diets containing no meat or meat products [22]. Types of control: Non-vegetarian diets, defined as diets containing meat or meat products. Types of outcome: Association between response to vegetarian diets and the risk of gastrointestinal cancer [23] (cancer incidence), pooled using relative risk (RR) or odds ratio (OR) with 95% confidence interval (95% CI ). Types of study: Observational study (cohort study and case-control study) conducted in humans. Exclusion criteria Exposure to certain plant foods rather than vegetarian diets. Literature review, systematic review, study protocol, comments, letters, case reports, or summaries. Full-text or data unavailable. Repeated publication. Outcome of morbidity of benign cancers. Study screeningStudy screening was conducted independently by two reviewers (Bai and Peng). Disagreements were resolved through discussion or by a third reviewer (Wu).
Titles and abstracts of included articles were screened manually in Endnote X9 to identify studies that met the inclusion criteria. Full texts of studies that met the inclusion criteria were retrieved and read to identify eligible studies. For the same study reported by more than one article, the latest published study with the most complete data was included.
Data extraction and quality assessmentData extraction and quality assessment were independently conducted by two reviewers (Bai and Peng). Disagreements were resolved through discussion or by a third reviewer (Wu).
We extracted the following data from the included studies: name of the first author, publication date, nationality, type of study, participant characteristics (age, sex, and sample size), follow-up duration in the cohort study, cancer site and outcome (effect), exposure, and confounders modified using multivariate models.
The Newcastle-Ottawa Scale (NOS) [24] was used to assess the risk of bias in the included observational studies. The NOS comprises two subscales: cohort and case-control studies. Both subscales have a maximum score of 9. Study scores of 7–9, 3–6, and 0–3 were considered high, medium, and low quality, respectively.
Data synthesis and statistical analysisGastrointestinal cancer morbidity was selected as the primary outcome of this study. RR was applied as a pooled statistic, and a 95% CI was provided. In this meta-analysis, results from multivariate models were used, and potential confounders were analyzed. The effects from all included studies were converted into natural logarithmic values and standard errors before statistical analysis. A random-effects model was used to pool the effects. Statistical significance was set to <0.05. The results are presented in a forest plot. The I2 statistic was used for heterogeneity assessment. An I2 value of >50% indicated significant heterogeneity. A subgroup analysis was performed to identify the sources of heterogeneity. Cancer sites, geographical regions, sex, and study design were used as variables for subgroup analysis. A sensitivity analysis was performed to assess the potential effects of each study on the results. A funnel plot was used for the intuitive assessment of publication bias, and the results were confirmed using Egger’s test. A P-value of <0.05 indicated significant publication bias of included studies. All data analyses were performed using Stata 15.0.
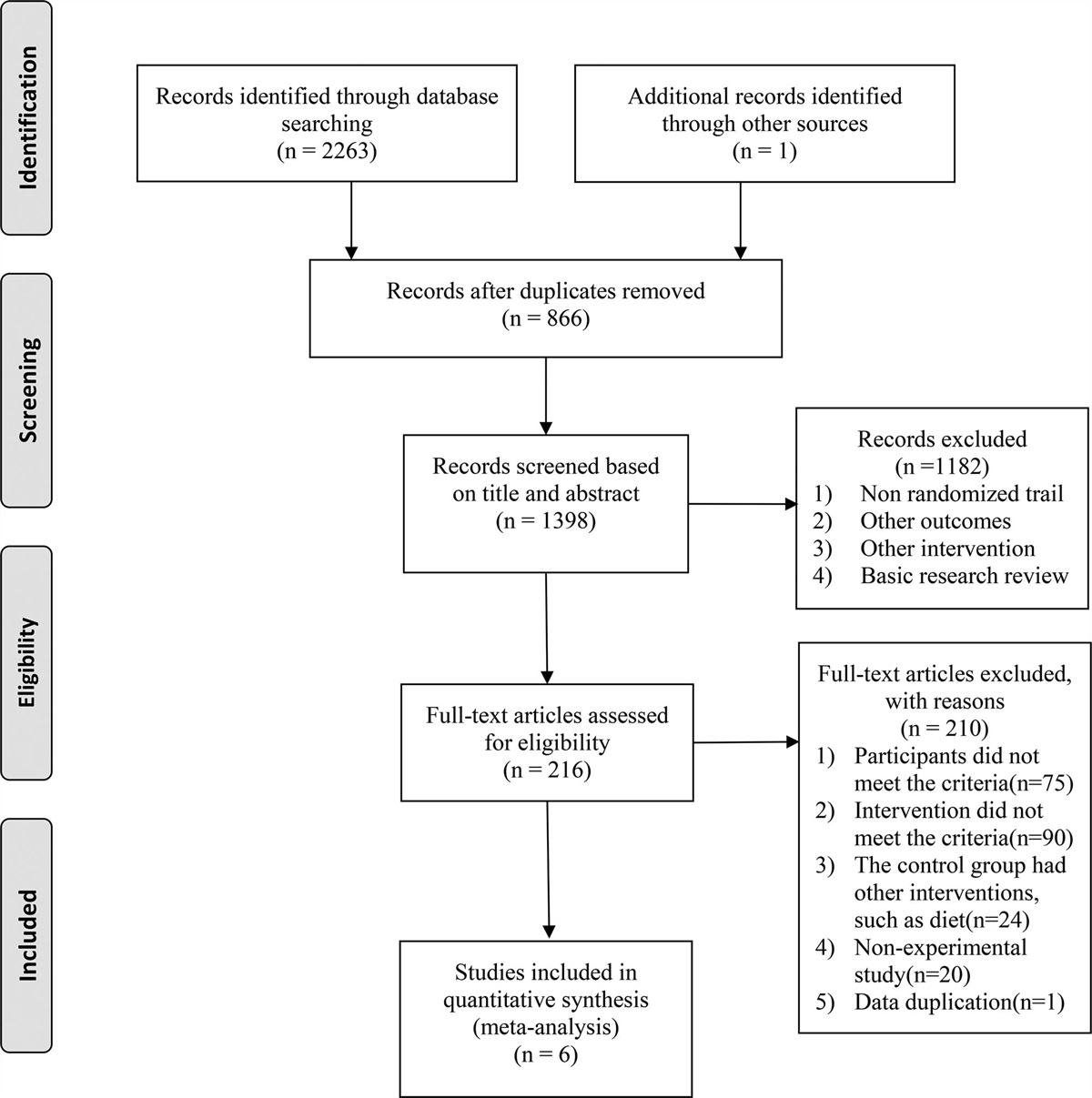
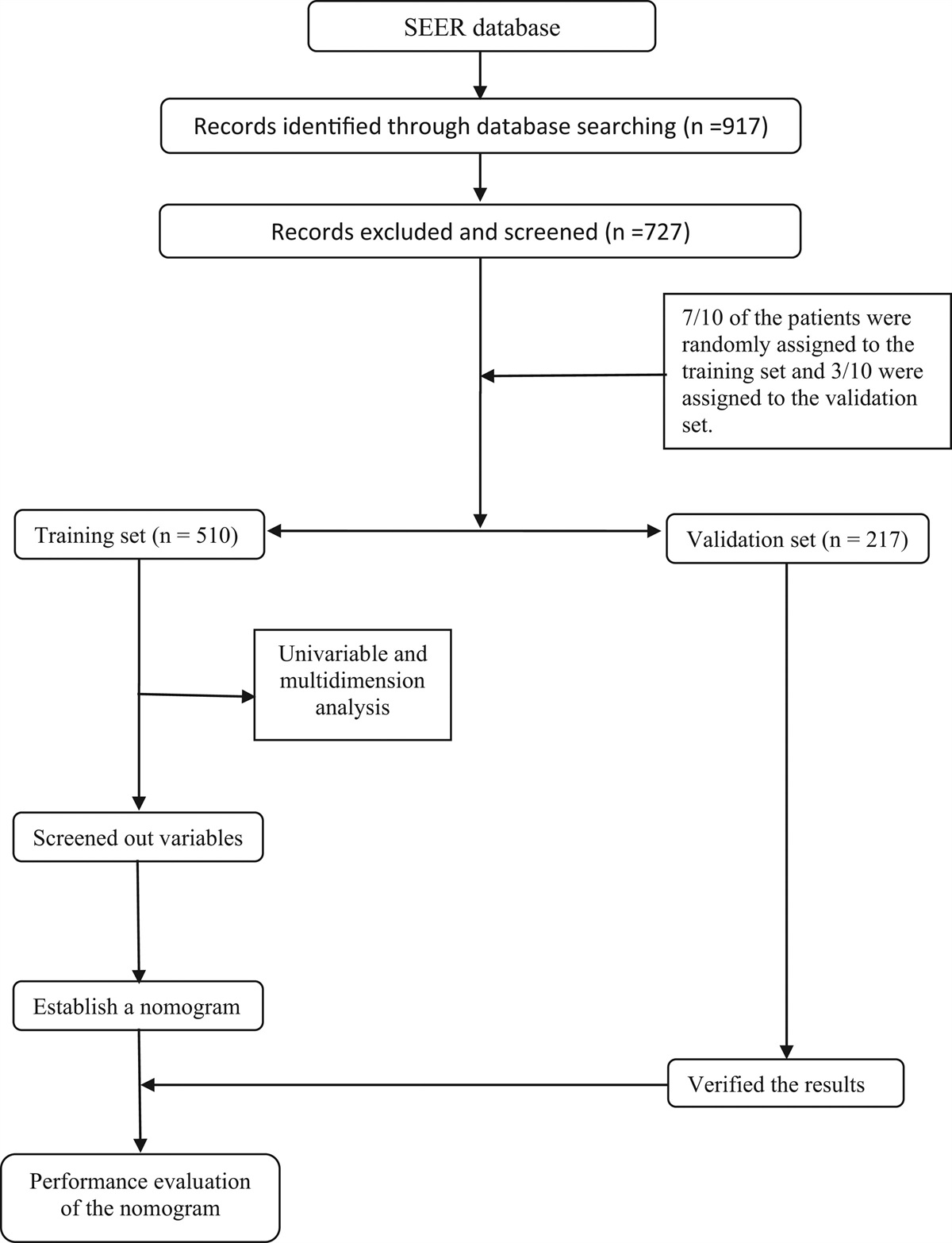
Results Study selectionA total of 1066 articles were identified. After removing 72 duplicates, the titles and abstracts of the remaining 994 articles were reviewed, and 948 articles were excluded. The full texts of the remaining 46 articles were retrieved and read, of which seven studies were finally included in the meta-analysis. The study selection process is shown in Fig. 1. The 39 articles were excluded after full-text reading for the following reasons: (a) repeated reporting for the same cohort; (b) use of a certain plant food as exposure rather than vegetarian diets; (c) unavailable data; (d) other types of studies; and (e) outcome of other cancer sites. The detailed reasons for exclusion are provided in Appendix 2, Supplemental digital content 2, https://links.lww.com/EJGH/A916.
 Fig. 1.:
Fig. 1.: Flowchart of study selection.
Characteristics of included studiesSeven articles were included [17,18,25–29], including one case-control study [27] and seven cohort studies [17,18,25,26,28,29]. The characteristics of the included studies are presented in Table 1. The studies included 686 691 participants aged 20–89 years. The follow-up duration of the included studies was 5–20.3 years, and the publication dates ranged from 1998 to 2022. Only two of the included studies reported sex-associated outcomes, of which one study contained the outcomes of both male and female participants [17], whereas the other study contained only the outcomes of female participants [28]. Regarding the cancer types, one study focused on upper gastrointestinal cancers (excluding the stomach) [26], two focused on gastric cancers [26,27], and six focused on colorectal cancers [17,18,25,26,28,29]. Regarding study location, two studies were conducted in North America (the USA [29], the USA and Canada [18]), five were conducted in Europe (the UK [17,26,28] and the Netherlands [25]), and one in Asia (India [27]). Regarding the types of exposure identification, seven studies used questionnaire surveys [17,18,25,26,28,29] and one used a questionnaire interview [27]; further, one study defined meat-free diet as vegetarian diet [29], one study provided a clear description of lacto-ovo-vegetarian and strict vegetarian diets [18], and one failed to subdivide the types of vegetarian diets [27]. All included studies processed confounders during data analyses, and the confounders included sex, age, BMI, physical activity, and smoking and drinking status.
Table 1. - Characteristics of included studies First author Year Country Designa Age (years) Genderb Number of subjects Follow-up (years) Exposure Cancer sitec Effect size Adjustmend SinghaCohort: cohort study, case-control: case-control study.
bF, female; M, male.
cGI: gastrointestinal; ICD 9th/ ICD-9: International Classification of Diseases, 9th Revision; ICD-10: International Classification of Diseases, 10th revision; ICD-O: International Classification of Diseases for Oncology.
dCRC, colorectal cancers.
The risk of bias was assessed using the NOS. All eight included studies were graded as high-quality, as shown in Appendix 3, Supplemental digital content 3, https://links.lww.com/EJGH/A917.
Statistical synthesis of resultsThe effects of the eight studies were pooled using a random-effects model (I2 = 55.4), and the results showed that vegetarian diets were inversely associated with the risk of gastrointestinal tumorigenesis compared with non-vegetarian diets [RR = 0.77, 95% CI (0.65–0.90), P = 0.017] (Fig. 2).
 Fig. 2.:
Fig. 2.: Forest plot (random-effect model) of the correlation between vegetarian diets with gastrointestinal cancer.
Due to existing heterogeneity (I2 = 55.4, P = 0.017), a subgroup analysis was performed to identify the sources of heterogeneity: cancer sites, geographical regions, sex, and study design. The results are shown in Table 2 (Figures of analysis are presented in Appendix 4 and Figures S1–4, Supplemental digital content 4, https://links.lww.com/EJGH/A918). Subgroup analysis showed that heterogeneity may be associated with sex (0%-65.2%) and geographical regions (26.5%-50.1%). Subgroup analysis based on cancer sites showed that vegetarian diets were negatively correlated with the risk of gastric cancer [RR = 0.41, 95% CI (0.28–0.61), I2 = 0%, P = 0.766] in two studies and with the risk of colorectal cancer [RR = 0.85, 95% CI (0.76–0.95), I2 = 20.1%, P = 0.277] in six studies, while they were uncorrelated with the risk of upper gastrointestinal cancer (excluding the stomach) [RR = 0.93, 95% CI (0.61–1.42)] in one study. Subgroup analysis based on sex indicated that vegetarian diets were negatively correlated with the risk of gastrointestinal tumorigenesis in men [RR = 0.57, 95% CI (0.36–0.91)] in one study, whereas they were uncorrelated in women [RR = 0.89, 95% CI (0.71–1.11), I2 = 0%, P = 0.399] in two studies. Subgroup analysis based on different regions revealed that vegetarian diets were negatively correlated with the risk of gastrointestinal tumorigenesis in North American populations [RR = 0.76, 95% CI (0.61–0.95), I2 = 26.5%, P = 0.256] in two studies and Asian population [RR = 0.43, 95% CI (0.26–0.72)] in one study, and they were uncorrelated in European populations [RR = 0.83, 95% CI (0.68–1.01), I2 = 50.1%, P = 0.075] in five studies. Subgroup analysis based on study design revealed that vegetarian diets were negatively correlated with the risk of gastrointestinal tumorigenesis in cohort studies [RR = 0.81, 95% CI: 0.70–0.94, I2 = 42.1%, P = 0.087] in seven studies and case-control studies [OR = 0.43, 95% CI: 0.26–0.72] in one study.
Table 2. - Subgroup analysis based on random-effect model for the correlation between vegetarian diets with gastrointestinal cancer Subgroup Number of studies RR (95% CI) I 2(%) P-value of heterogeneity z P-value Overall 8 0.77aGI, gastrointestinal; upper GI, upper gastrointestinal tract (excluding stomach).
bCohort: cohort study, case-control: case-control study.
Sensitivity analysis showed that the removal of any of the included studies did not result in reversed results (Appendix 4, Figure S5, Supplemental digital content 4, https://links.lww.com/EJGH/A918). Publication bias assessment showed that the funnel plot was slightly asymmetric (Appendix 4, Figure S6, Supplemental digital content 4, https://links.lww.com/EJGH/A918), and Egger’s test confirmed the existence of publication bias among the included studies (P = 0.011 < 0.05) (Appendix 4, Figure S7, Supplemental digital content 4, https://links.lww.com/EJGH/A918). However, the estimated results of publication bias identified by the trim-and-fill method or fail-safe number would be greatly impacted by the small number of studies included in this meta-analysis; therefore, no further analysis was performed in this study. We also assessed all included cohort studies using a modified version of the NOS scale to evaluate study quality [30,31], as shown in Appendix 3 and Table S3, Supplemental digital content 3, https://links.lww.com/EJGH/A917. The risk of bias assessment of included studies using NOS and NOS Modified version was similar.
DiscussionThis is the first systematic review conducted to assess the correlation between vegetarian diets and the risk of gastrointestinal cancers. Compared with other systematic reviews on similar topics, this study included more types of gastrointestinal cancers (upper gastrointestinal, gastric, and colorectal cancers). The other three published reports on the subject only evaluated the relationship between vegetarian diets and colorectal cancer risk [32–34]; however, they did not evaluate the association between vegetarian diets and the risk of gastrointestinal cancers at other sites, although previous studies have shown that upper gastrointestinal cancer risk is not only related to the level of food processing [35–41] but also to the type of food [42–44]. The study results are consistent with those of a previously published systematic review based on prospective cohort studies [34]; that is, vegetarian diets are correlated with a decreased risk of colorectal cancers.
The results of this systematic review indicate that adherence to vegetarian diets can reduce the risk of gastrointestinal cancers compared with non-vegetarian diets. This study provides a reference for primary prevention strategies for gastrointestinal cancers. However, the effects of vegetarian diets on different gastrointestinal cancers varied because of the small number of studies included. First, the effects of vegetarian diets may depend on cancer sites. Consuming vegetarian diets can reduce the risk of gastric and colorectal cancers, but it is not correlated with the risk of upper gastrointestinal cancers (excluding the stomach). However, the number of included studies was small, and this could easily be a chance variation; therefore, the results need to be confirmed by more relevant studies. Second, the effects of vegetarian diets on gastrointestinal tumorigenesis may be influenced by sex and geographical region. Based on the small amounts of data, the study results indicate that vegetarian diets can reduce the risk of gastrointestinal cancers in male participants; however, this association was not observed in female participants. Vegetarian diets can reduce the risk of gastrointestinal cancers in North American and Asian populations, whereas no correlation was observed in the European population. In summary, heterogeneity in this study was associated with participant sex and geographical regions. None of the studies included in this meta-analysis significantly affected the statistical results; however, publication bias was present.
This systematic review has shown that the effects of vegetarian diets on gastrointestinal cancers vary in different cancer sites, which may be associated with differences in etiology, histopathological backgrounds, and contactants (foods, feces, etc.) of the upper gastrointestinal (excluding the stomach), gastric, and colorectal cancers [45–52]. Plant foods such as fruits, vegetables, legumes, and whole grains and nutrients in these foods such as vitamin C, folic acid, β-carotene, and dietary fiber exert different protective effects on gastrointestinal cancers in different locations, whereas animal foods such as red meat, seafood, poultry meat, and other animal foods have different pathogenetic effects on gastrointestinal cancers in different locations. At present, relevant studies have yielded limited data; therefore, the effects of vegetarian diets on the risk of gastric and upper gastrointestinal cancers (excluding the stomach) need to be further elucidated.
Vegetarian diets can reduce the risk of gastrointestinal cancers in male participants, while no correlation has been observed in female participants, indicating different gastrointestinal cancer-protective activity of vegetarian diets between the sexes. This may be related to the natural difference in the risk of gastrointestinal cancers between the sexes. Global epidemiologic studies have shown a lower morbidity of gastrointestinal cancers in the female population than in the male population [53–57], which could be explained by differences in cancer-associated risk factors and gonadal hormones between the sexes. Since the correction factors included in this study mostly contained cancer-related risk factors such as obesity, smoking, and physical activity, sex differences in the effects of vegetarian diets on gastrointestinal cancer risk can be considered to be related to different sex hormones. Previous studies have demonstrated the protective activity of estrogen and its receptors in the pathogenesis of gastrointestinal cancers [58–62]. Therefore, sex differences in vegetarian diets may be attributed to the protection of women by estrogen. Alternatively, these findings could be coincidental as few studies were included. Future studies need to further explore this phenomenon and its potential mechanisms, as sex variance is a crucial factor in clinical trials [63–65].
The effects of vegetarian diets on gastrointestinal cancers vary in different geographic regions, which might be related to differences in the risk for gastrointestinal cancers among regions [53–57]. Race, living conditions, and customs vary across regions [45,66–71], leading to different effects of vegetarian diets on the risk of gastrointestinal cancers. For example, most regions in the UK and Europe are Se-deficient, which could explain the lack of a correlation between vegetarian diets and colorectal tumorigenesis in the populations of these regions.
Generally, the protective effects of vegetarian diets on gastrointestinal tumorigenesis are based on two aspects. First, vegetarian diets avoid the carcinogenic risks posed by red and processed meat diets [15,38]. Studies have demonstrated a correlation between meat consumption and tumorigenesis [8,9,72], and previous studies have partially uncovered its potential mechanisms. The alkylation characteristics of colorectal cancers are associated with patients’ high intake of red meats before diagnosis [73], and the cause of this mutation is N-nitroso compounds (NOC). NOC are metabolites of heme, ferrous iron, or meat nitrite/nitrate [74]. Second, intake of whole grains, plant fibers, fruits, and vegetables decreases the risk of cancer [75,76]. These plant-based foods comprise the majority of vegetarian diets. Other dietary patterns, consisting primarily of plant-based foods, can also reduce the risk of gastrointestinal cancers [37,77]. The mechanisms of plant-based diets in cancer prevention are as follows. First, fruits and non-starchy vegetables contain abundant anticancer agents such as dietary fibers, carotenoids, and vitamin C [78]. In contrast, the gut microbiota plays a potential role in regulating the correlation between diet and colorectal cancers [75]. For instance, various types of dietary fibers can be fermented or metabolized by colonic microbes [79], generating a metabolite called butyrate, which has been demonstrated to have proliferation-inhibiting activity against colonic cancer cells [80].
Although vegetarian diets can reduce the risk of many chronic diseases, different types of vegetarian diets have different health effects [81]. However, this approach is not always beneficial. Compared with healthy plant-based diets, unhealthy plant-based foods may increase disease risk [82–84] because vegetarian diets contain various types of food, and it would be too broad to consider all vegetarian diets as a dietary pattern. Therefore, future studies should subdivide vegetarian diets more specifically and scientifically and provide healthy plant diet recommendations individually based on risk factors (age, family history of cancer, BMI, etc.) in different populations [85].
This systematic review has the following limitations. First, although this study involves a large number of participants, the heterogeneity between studies is significant. Second, publication bias exists in the systematic review. Third, some limitations exist due to the limited number of included studies. The included studies failed to involve populations in other regions, such as Oceania, South America, and Africa, and data on upper gastrointestinal (excluding the stomach) and gastric cancers appear insufficient. Therefore, more comprehensive clinical trials involving more geographical regions, races, social backgrounds, religious beliefs, and other factors are warranted to further describe in detail the effects of different subtypes of vegetarian diets on the risk of upper gastrointestinal (excluding the stomach), gastric, and colorectal cancers and provide more evidence supporting the primary prevention strategy for gastrointestinal cancers.
ConclusionVegetarian diets can reduce the risk of gastrointestinal cancers compared with non-vegetarian diets. Specifically, adherence to vegetarian diets can reduce the risk of gastric and colorectal cancers but not of upper gastrointestinal cancers (excluding the stomach). They can also reduce the risk of gastrointestinal cancers in men, but not in women. Further, vegetarian diets may reduce the risk of gastrointestinal cancers in North American and Asian populations, whereas no correlation was observed in the European population. This study has some limitations owing to its small sample size. Further studies are required to assess the effects of vegetarian diets.
AcknowledgementsConception – Tongtong Bai and Chengyu Wu; Literature Search – Tongtong Bai and Juanjuan Peng; Screening and Selection – Tongtong Bai, Juanjuan Peng, and Chengyu Wu; Collection and assembly of data – Tongtong Bai and Juanjuan Peng; Risk of Bias – Tongtong Bai, Juanjuan Peng, and Chengyu Wu; Data analysis and interpretation – Tongtong Bai and Xinqi Zhu; Manuscript writing – Tongtong Bai, Xinqi Zhu and Chengyu Wu; Approval – All authors.
Conflicts of interestThere are no conflicts of interest.
References 1. Arnold M, Abnet CC, Neale RE, Vignat J, Giovannucci EL, McGlynn KA, et al. Global burden of 5 major types of gastrointestinal cancer. Gastroenterology 2020; 159:335–349.e15. 2. Wu S, Powers S, Zhu W, Hannun YA. Substantial contribution of extrinsic risk factors to cancer development. Nature 2016; 529:43–47. 3. Solans M, Chan DSM, Mitrou P, Norat T, Romaguera D. A systematic review and meta-analysis of the 2007 WCRF/AICR score in relation to cancer-related health outcomes. Ann Oncol 2020; 31:352–368. 4. Shams-White MM, Brockton NT, Mitrou P, Romaguera D, Brown S, Bender A, et al. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) cancer prevention recommendations: a standardized scoring system. Nutrients 2019; 11:1572. 5. Siegel RL, Jemal A, Wender RC, Gansler T, Ma J, Brawley OW. An assessment of progress in cancer control. CA Cancer J Clin 2018; 68:329–339
Comments (0)