
Remember me


Linking children and adolescents (CAs) to HIV care in eastern and southern Africa (ESA) should be designated a priority. The Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated there were 1,050,000 CAs aged 0–14 years living with HIV in ESA in 2021, and of those, only 56% were on antiretroviral therapy (ART).1 For Kenya specifically, UNAIDS estimates were at 83,000 for this age group, with 59% on ART.1
This low percentage of CAs who have linked to HIV care and who are on treatment needs to improve. Without it, many CAs will die needlessly. There were an estimated 46,000 AIDS-related deaths among CAs in ESA in 2021, and in Kenya, there were 3100.1
Many CAs in communities are living with HIV but are not being connected to care for a myriad of reasons, resulting in an attrition in the HIV Treatment Cascade.2 How can we increase the number of CAs who test positive for HIV and then link to care so they can go onto begin ART?
A first step in addressing this issue may be obtaining more accurate and comparable estimates of HIV linkage to care to better understand how many CAs are actually linking, as some current limitations exist. For example, available estimates of linkage to care using facility-based or provider-initiated data may overestimate population-level linkage given caregivers or adolescents have actively sought out testing or other medical care.3 Other existing estimates may be inaccurate given they may fail to take into account the outcomes of those who have transferred to another care system or those who have died.4–6 Finally, definitions of linkage to care may vary, making interpretation and examination of findings over time challenging, particularly because guidelines for initiating ART have changed.3,5–8
Population-level estimates, by contrast, should offer more accurate and generalizable information that can help us improve linkage to care. These calculations should be less biased given they should capture and represent more of a designated target population, thereby also providing better insights into the factors associated with poor HIV outcomes. This in turn could increase the effectiveness of interventions, including policies, designed to improve linkage to care. Relatedly, the findings should also apply to a larger group of people.
Given the limited population-level linkage to care estimates that exist for CAs in western Kenya, we used home-based counseling and testing (HBCT) data to estimate population-level outcomes, acquiring the data by performing door-to-door visits and achieving extensive coverage (∼97%) in the geographic area.9,10 We then merged that HBCT data with medical record data in the same areas to estimate the percentage of CA who had linked to care since their encounter with the HBCT team. Subsequently, the team conducted follow-up of children and adolescents without evidence of linkage to care at facilities to determine their outcomes (eg, linked to care elsewhere or died) to update our estimates of linkage to care and death and to determine factors associated with linkage and death among children and adolescents in western Kenya. Our primary hypothesis was that more CAs would have linked to care than evident based in the Academic Model Providing Access to Healthcare (AMPATH) Medical Records, but that linkage would still be low.
METHODS Study Setting and Data SourcesThis study included 2009–2015 HIV testing and care data from the Bunyala (Busia County), Chulaimbo (Kisumu County), and Teso North (Busia County) subcounties in Kenya and were collected by the AMPATH program.
AMPATH is a medical, teaching, and research collaborative between Moi University, Moi Teaching and Referral Hospital in Kenya, and other national and international institutions.11,12
AMPATH, as part of a USAID–AMPATH initiative to increase HIV testing among communities, implemented door-to-door home-based HBCT, which included community mobilization, HIV testing and counseling in homes, and follow-up by counselors after diagnosis.9,10 The counselors for HBCT worked within defined geographic areas to follow-up with people over time. As is captured in one of the publications directly related to HBCT, individuals aged 13 years and older in the geographic areas above were eligible for HIV testing and a child younger than 13 years was eligible if his/her mother was HIV-positive or the mother's HIV status was unknown or if the mother had died or her death status not known.9 Data were also captured from individuals who were either diagnosed as HIV-positive before HBCT or who were previously known to be HIV-positive during HBCT.9
From 2013 to 2017, individuals who were diagnosed with HIV during HBCT or known to be HIV-positive at the time of HBCT were matched with patient data from the AMPATH medical record system (AMRS) using unique patient identifiers. Matching of the data sources occurred through use of multiple methods, including probabilistic and deterministic matching.13–17 More information on HBCT, AMRS, and the data matching process used are provided in other published literatures.9,10,15,17 Subsequent to this matching process, each child or adolescent living with HIV was identified as “linked to care,” with linkage dates defined by a clinical encounter with an HIV care provider, or linkage to care status “unknown”, with no records matching within AMRS.
Given that previous research among adults suggested a substantial amount of error in the matching process, we conducted follow-up of children and adolescents in the Bunyala catchment who were identified as HIV-positive during HBCT, but whose linkage to care status remained “unknown” after the matching process.15,17 The study team conducted visits to the child or adolescent and his or her caregiver or an informant who knew the child/adolescent or family.
The individuals who conducted the tracking for this analysis were study staff and worked with those from the HBCT teams to locate individuals in communities to determine their outcome status. The child or adolescent's linkage to care and vital status at the time of the visit was determined and categorized as one of the following: (1) alive and had linked to AMPATH care (but the record was missed during matching), (2) alive and had linked to care elsewhere, (3) alive but unable to be reached, (4) did not link to care, (5) died since HBCT, or (6) could not be reached and the outcome was unknown. The “Alive and had linked to AMPATH care (but the record was missed during matching)” status meant the child/adolescent was alive and had linked to HIV care in an AMPATH clinic, but the record was not identified during the matching process. The “Alive and had linked to care elsewhere” status meant the child/adolescent was alive and had linked to HIV care at another clinic not affiliated with AMPATH, and this information was determined during the follow-up visit. “Alive but unable to be reached” means the person who conducted the interviews during the follow-up study found an informant (such as a neighbor) who confirmed the child/adolescent was still alive, but the child/adolescent/parent or guardian could not be reached to provide more information.
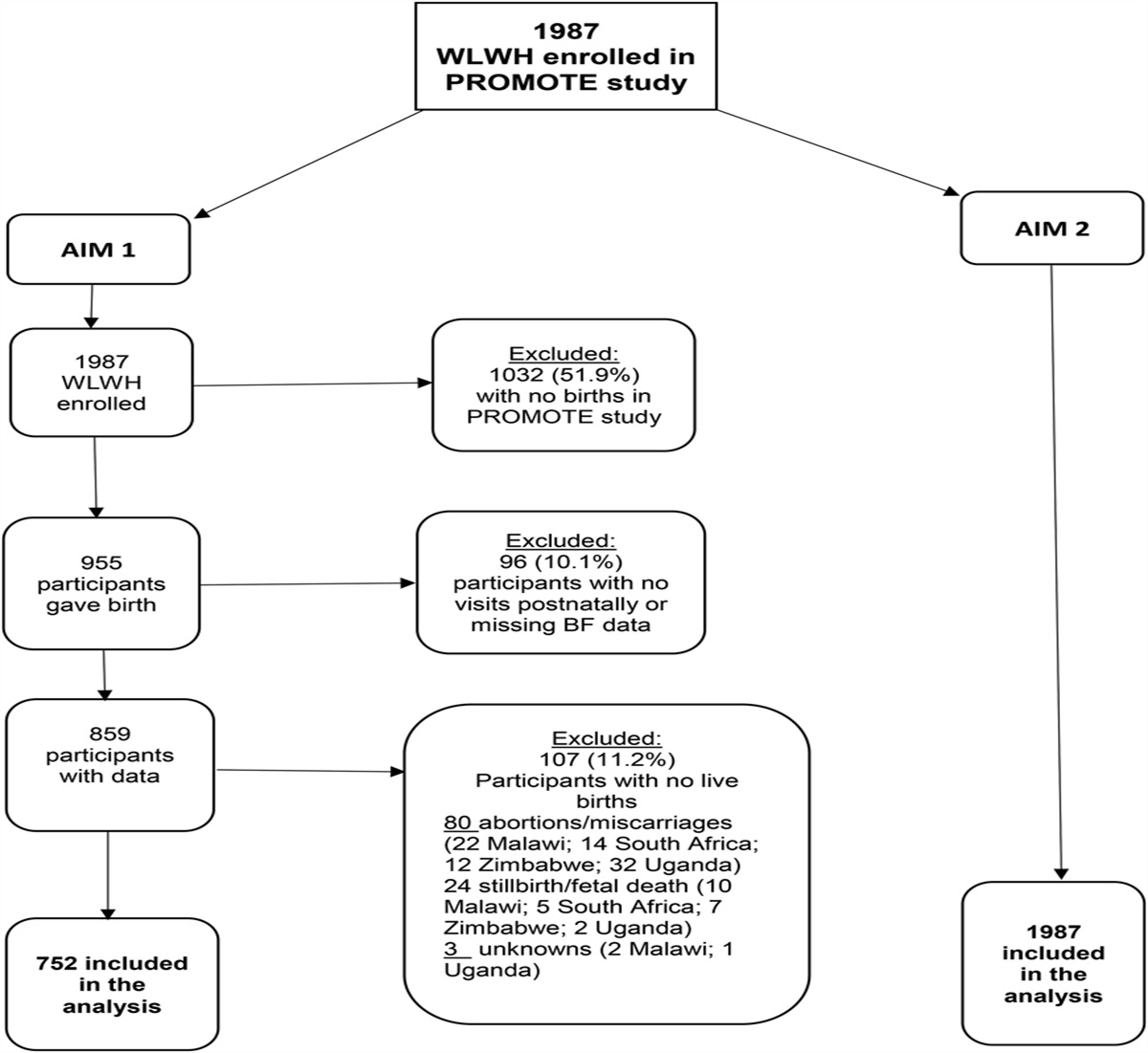
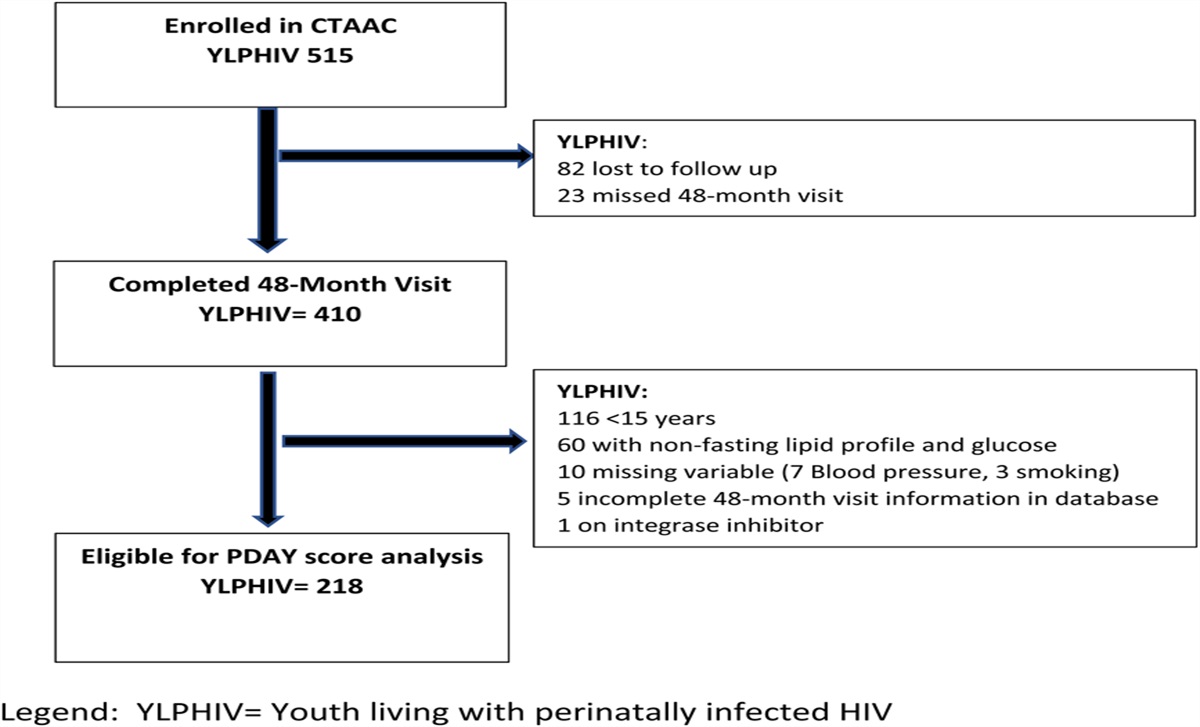
Children and adolescents were eligible for inclusion in our analysis if they were younger than 18 years and HIV-positive during an HBCT testing visit (either self-reported prior positive or testing positive at that visit; data were taken from the visit where the child or adolescent was first identified as positive if data from >1 HBCT visit was available) and if they had not enrolled in HIV care before being identified as positive at their first HBCT visit (Fig. 1).
 FIGURE 1.:
FIGURE 1.: Flowchart of children and adolescents in the AMPATH HBCT original sample—Bunyala, Teso North, and Chulaimbo subcounties in western Kenya.
VariablesInformation collected by HBCT counselors included the demographic characteristics of the children or adolescents and their family or primary caregivers (eg, sex, age, and marital status), as well as information related to their HIV status. For those persons who were found HIV-positive and who linked to care in AMPATH clinics, additional data from the AMRS were extracted, such as date of enrollment in HIV care (ie, linkage to HIV care).
Individual CharacteristicsAge was a continuous variable, measured in months for children younger than 1 year and years for children aged 1–17 years. Age was included in the analyses because it is a critical demographic factor affecting whether a child/adolescent is more dependent on a caregiver to access HIV care for him/herself. Sex was a binary variable representing the sex of a child or adolescent, female, or male. Sex is also an important demographic variable included in the analysis that has the potential to influence whether a child/adolescent receives access to healthcare, as male children may be prioritized over girl children in some cultures and this has the potential to influence care received.18 Orphan status was a categorical variable (yes/no/unknown), representing having a deceased mother and/or father. Orphans are considered a vulnerable population for many issues, which may potentially include linking to HIV care and the other HIV Care Continuum stages.19 Finally, the mother's HIV status (positive/negative/unknown), indicating whether the child or adolescent's mother was HIV-positive based on a positive test or prior HIV-positive status obtained during HBCT, was included as a categorical variable in the analysis. We postulated that a mother with a known HIV-positive status may be more likely to access care for her HIV-positive child at or close to her own treatment appointments.
OutcomesTime to linkage to care was defined as the time from the first positive HIV result according to HBCT (origin) to the time when a child or adolescent completed a clinical encounter with an HIV care provider as documented in AMRS or identified as linked to care through the Bunyala follow-up study. Time to death was defined as the time from the first positive HIV test result from HBCT (origin) to the time a child or adolescent died as documented in AMRS or as identified in the Bunyala follow-up study. For both linkage to care and death, those with an “unknown” status were treated as missing and imputed using a discrete-time competing risks model that is detailed below.
AnalysesWe generated estimates of linkage to care and death using data from all 3 subcounties, Teso North, Chulaimbo, and Bunyala, and used the imputation model developed on the follow-up sample to handle those with missing linkage information. To address the possibility that the follow-up sample was not perfectly representative of the larger sample, we weighted the observations by the inverse probability of being selected for follow-up. We fit a weighted multinomial logistic regression model using double-sampled visits data from Bunyala. The multinomial outcome includes the following levels: “Alive and linked to care” (we combined responses for linkage to care at AMPATH and linkage to care outside of AMPATH), “Did not link to care” (censored), and “Died.” “Alive unable to be reached” was used in the sensitivity analysis. “Could not be reached and outcome unknown” was not included in the models. We determined the odds of linkage to care and death based on the individual characteristics and year (modeled as first order and second order). Adjusted odds ratios (aORs) of linkage and death with 95% confidence intervals (CIs) were estimated for each individual characteristic of interest. Missing data for orphan status and mother's HIV status were modeled as a no/unknown category. Sex and age had no missing data.
The imputation of the status for those with missing linkage information was conducted using a Bayesian data augmentation procedure: to generate each imputation, we first took a draw from the posterior of the model parameters, then conditional on that posterior parameters estimate, we calculated the posterior marginal probability of the multinomial outcome, based on which we generated a predicted (imputed) value for linkage status. The imputation model was constructed as a discrete-time competing risks model to allow for linkage, no linkage, or death at each time point.
Following imputation of missing linkage data, we calculated the total percentage of CAs who were linked to care or who had died for all 3 catchment areas combined, stratified by individual characteristics and year. We plotted Kaplan–Meier curves of time to linkage to care and death for all 3 combined catchment areas. The time scale was in 1-year intervals. We imputed the trajectory for each person by simulating multinomial outcomes sequentially over time until an absorbing state, that is, simulated linkage to care or death, occurred or until the end of 8 years when an individual was simulated to be censored. We explored the upper bound of linkage to care by combining the number of those known to be linked with the 20 people who were known to be alive but unable to be reached and then the lower bound by assuming 0 of those individuals had linked (resulting in their being censored).
EthicsInstitutional review board (IRB) approvals were obtained from Moi University and the University of Toronto. Johns Hopkins University provided additional IRB approval of analyses. Individuals provided consent at the time of testing and at the time of follow-up.
RESULTS Characteristics of the Original Sample of the Three Catchment Areas (n = 720)There were a total of 1478 children and adolescents younger than 18 years who were either diagnosed with HIV or identified as known HIV-positive during HBCT. Of these 1478 CAs, 757 had already accessed HIV care before HBCT, leaving 721 eligible for this analysis, with 523 from Chulaimbo, 145 from Bunyala, and 53 from Teso. One CA was removed from the analytic sample owing to a negative time calculation, with time being needed for later analyses. Of the remaining 720, approximately 68% of the sample was aged 0–9 years and 59% were female (Table 1). Around 39% were a single or double orphan, with approximately 10% having an unknown or missing orphan status, and 28% of the CAs overall had completed primary school. Sixty-seven percent of children or adolescents had a mother known to be HIV-positive, with 24% having a mother with unknown HIV status.
TABLE 1. - Individual and Household Characteristics of 720* Children and Adolescents Identified as Living With HIV During HBCT, by Geographic Location Child/Adolescent Characteristics Total (n = 720) Bunyala (n = 144) Chulaimbo (n = 523) Teso (n = 53) n (%) or Med (IQR) n (%) or Med (IQR) n (%) or Med (IQR) n (%) or Med (IQR) Age (year) 0–9 487 (67.6) 94 (65.3) 350 (66.9) 43 (81.1) 10–17 233 (32.4) 50 (34.7) 173 (33.1) 10 (18.9) Missing 0 0 0 0 Sex Females 428 (59.4) 89 (61.8) 306 (58.5) 33 (62.3) Males 292 (40.6) 55 (38.2) 217 (41.5) 20 (37.7) Missing 0 0 0 0 Single or double orphan Yes 279 (38.8) 43 (29.9) 217 (41.5) 19 (35.9) No 371 (51.5) 73 (50.7) 268 (51.2) 30 (56.6) Unknown 22 (3.1) 5 (3.5) 15 (2.9) 2 (3.8) Missing 48 (6.7) 23 (16.0) 23 (4.4) 2 (3.8) Education level of child or adolescent Primary school 204 (28.3) 30 (20.8) 160 (30.6) 14 (26.4) Secondary or tertiary school 16 (2.2) 1 (0.7) 13 (2.5) 2 (3.8) None 475 (66.0) 90 (62.5) 348 (66.5) 37 (69.8) Missing 25 (3.5) 23 (16.0) 2 (0.4) 0 Mother HIV positive Yes 481 (66.8) 79 (54.9) 365 (69.8) 37 (69.8) No 22 (3.1) 6 (4.2) 12 (2.3) 4 (7.6) Unknown 169 (23.5) 36 (25.0) 123 (23.5) 10 (18.9) Missing 48 (6.7) 23 (16.0) 23 (4.4) 2 (3.8) Father HIV positive Yes 228 (31.7) 51 (35.4) 157 (30.0) 20 (37.7) No 44 (6.1) 8 (5.6) 29 (5.5) 7 (13.2) Unknown 400 (55.6) 62 (43.1) 314 (60.0) 24 (45.3) Missing 48 (6.7) 23 (16.0) 23 (4.4) 2 (3.8) Household characteristics Land owned (acres) 1 (0.0, 2.0) 0.5 (0.0, 1.0) 1 (0.25, 2.0) 1 (0.25, 2.0) Missing 272 (37.8) 61 (42.4) 188 (36.0) 23 (43.4) Owned at least 1 cow, goat, or sheep Yes 222 (30.8) 21 (14.6) 184 (35.2) 17 (32.1) No 185 (25.7) 41 (28.5) 127 (24.3) 17 (32.1) Missing 313 (43.5) 82 (56.9) 212 (40.5) 19 (35.9) Household size 4 (3, 6) 4 (3, 6) 4 (3, 6) 5 (4, 6) Missing 0 0 0 0 Number of children in a Household 2 (1, 3) 2 (1, 3) 2 (1, 3) 2 (2, 3) Missing 0 0 0 0*One CA dropped from analytic sample given negative time calculation; time needed in later analyses.
Of the 97 CAs in the follow-up study sample from Bunyala, more than half (61%) were younger than 10 years. Sixty-seven percent were female, and 33% were a single or double orphan, with approximately 14% having missing or unknown orphan status. Twenty-four percent had attended primary school, and 57% had a mother known to be HIV-positive, with 39% of mothers having an unknown or missing HIV status. The percentages of characteristics among this follow-up study sample versus the original sample of the 3 catchment areas were similar (data not shown).
Probability of Linking to HIV Care or DeathIncorporating data from the follow-up study in Bunyala, the average probability of linking to care in the 3 catchment areas was between 47.6% and 49.2% at 2 years, 50.7%–50.9% at 4 years, 53.9%–59.3% at 6 years, and 63.7%–78.0% at 8 years (Fig. 2). The average probability of death was 13.0% at 2 years, 16.1% at 4 years, 18.4% at 6 years, and 19.3% at 8 years.
 FIGURE 2.:
FIGURE 2.: Time to linkage and death among children and adolescents in Bunyala, Teso North, and Chulaimbo subcounties in western Kenya. The red dashed lines are credible intervals. Blue and black lines indicate that the true linkage probability has more than 95% chance of lying in this range. There is no upper bound for the blue line and no lower bound for the black line. The average lower bound early in the figure may be slightly higher than the higher bound as a result of stochasticity, being imputed separately.
The median age of CAs who linked to care was 7 years (IQR: 3–12). Around 57% of those who linked were female, and one-third were orphans. Sixty-five percent of those who linked had mothers who were HIV-positive. Of those who died in the 3 catchment areas, the median age was 5 years (IQR: 3.5–10.5). Sixty-four percent of CAs who died were female, and 55% who died were orphans (Table 2).
TABLE 2. - Observed Linkage to Care or Death, by Individual Characteristics Among Children and Adolescents in Bunyala, Teso North, and Chulaimbo Subcounties in Western Kenya (n = 720)* Linked to Care, Unable to Reach but Alive Included (n = 161)† Linked to Care‡ (n = 141) Died (n = 11) N (%) or med (IQR) N (%) or med (IQR) N (%) or med (IQR) Age (year) 7 (4, 14) 7 (3, 12) 5 (3.5, 10.5) Female§ 99 (61.5) 81 (57.4) 7 (63.6) Mother HIV-positive§ 96 (59.6) 92 (65.2) 9 (81.8) Single or double orphan§ 52 (32.3) 47 (33.3) 6 (54.5) Year 0 (0, 2) 0 (0, 1) 1 (0.5, 3.5)*Estimates use imputed data for Teso North and Chulaimbo; imputed information is based on data from the follow-up study involving children and adolescents in Bunyala, Kenya. From the follow-up study: “Alive and linked to care” (we combined responses for linkage to care at AMPATH and linkage to care outside of AMPATH) was modeled as an outcome. “Did not link to care” was not modeled and ultimately censored. “Died” was modeled as an outcome. “Alive unable to be reached” was used in sensitivity analysis. “Could not be reached and outcome unknown” was not included in models.
†Upper bound estimate—“Unable to reach but alive” included.
‡Lower bound estimate—“Unable to reach but alive” not included.
§Percentage of Yes, No, Unknown, and Missing responses.
Model 1 in Table 3 presents adjusted odds of linkage to HIV care or death among those who linked to care or who died. Among those who were single or double orphans, the adjusted odds of linkage to care was 2.66 times (95% CI: 1.33 to 5.32) the odds of linkage of those who were not orphans or status was unknown. CAs whose mothers were known to be HIV-positive had nearly 2 times the odds of linkage, compared with those whose mothers' status was not HIV-positive or unknown (aOR = 1.94, 95% CI: 0.97, 3.86). In both of these estimates, the magnitude of the estimate was elevated and precision was fair. In examining the odds of linkage to care for sex or age, the magnitude of the association was weak and was more protective, with the precision of the estimates being good.
TABLE 3. - Adjusted Odds Ratios of Linkage to Care or Death by Individual Characteristics Among Children and Adolescents in Bunyala, Teso North, and Chulaimbo Subcounties in Western Kenya Model 1* Model 2† Linked to care Died Linked to care, unable to reach but alive included Died aOR (95% CI)‡§ aOR (95% CI)‡§ aOR (95% CI)‡§ aOR (95% CI)‡§ Age 0.95 (0.89, 1.02) 0.89 (0.77, 1.03) 0.99 (0.93, 1.05) 0.9 (0.78, 1.04) Female 0.88 (0.48, 1.64) 1.62 (0.45, 5.8) 0.88 (0.5, 1.55) 1.63 (0.46, 5.87) Mother HIV-positive‖ 1.94 (0.97, 3.86) 14.49 (3.32, 63.19) 1.18 (0.66, 2.11) 12.1 (2.82, 52.03) Single or double orphan‖ 2.66 (1.33, 5.32) 9.85 (2.21, 44.01) 1.44 (0.79, 2.64) 8.79 (1.95, 39.51)*Lower bound estimate—“Unable to reach but alive” not included.
†Upper bound estimate—“Unable to reach but alive” included.
‡Adjusted for all variables in the table.
§Intercept, first-order year, and second-order year included in the models.
‖Unexposed status is combined no/unknown.
These numbers are calculated from the exponential of the estimated coefficient from the multinomial function in R.
The adjusted odds of death among those who were a single or double orphan was 9.85 times the odds among those who were not an orphan or had an unknown orphan status (95% CI: 2.21 to 44.01), while the adjusted odds of death among those whose mothers were HIV-positive was 14.49 (95% CI: 3.32, 63.19) times the odds of death among those whose mothers were not HIV-positive or HIV status was unknown. In both estimates, the magnitude of the association was greatly elevated; however, these estimates were not very precise, likely because of smaller numbers. The estimate for age suggested a weak association on the protective side, with fair precision, while the estimate for sex suggested an elevated association, although a very imprecise estimate, also perhaps because of small numbers.
DISCUSSIONThis study assessed time to linkage to care or death among children and adolescents aged 0–17 years in western Kenya who had not previously engaged in HIV care, as well as predictors of linkage and death. The probability of linkage, defined as having had an initial clinical encounter with an HIV care provider, among a population-based cohort of CAs in the Bunyala, Chulaimbo, and Teso North catchment areas, ranged from 47.6% to 49.2% at 2 years to 63.7%–78.0% at 8 years. The most current UNAIDS data for Kenya (2021; recent national data on percentage of linkage among CA in the country for comparison is limited) estimate that 59% of children aged 0–14 years in Kenya living with HIV were on ART (and thus had linked to care) in 2021, as well as 68% of adolescents aged 10–19 years.1 Although numbers from both our study and UNAIDS suggest there is need for improvement in linking CAs to care in Kenya, comparing our study's findings with that of the UNAIDS estimates is challenging given our data assess time to linkage to care over an 8-year period, whereas the UNAIDS estimates are based on the percent of those linked as of a certain year, 2021. In addition, our study only focuses on a limited geographic area in western Kenya while the UNAIDS estimates represent the whole nation of Kenya.
Finally, these results from our study are population-based, whereas the UNAIDS estimates are informed by other data sources.
Our study also found that the probability of death in these same 3 catchments was high, ranging from 13.0% at 2 years to 19.3% at 8 years. Death among these CAs represent CAs who never linked to care to begin ART (given they were not captured as linking to care over an extended period of time) and likely had advanced disease and died to opportunistic infections such as pneumonia or tuberculosis.20–22 Again, comparing our data against that of the above UNAIDS estimates is difficult, but both our data and the UNAIDS child and adolescent AIDS-related mortality data represent a high number of deaths, with an estimated 3100 children aged 0–14 years dying in Kenya in 2021.1 It is critical that CAs be linked to care on testing positive for HIV to prevent death in children and adolescents.
Predictors of Linkage to Care and DeathIn examining predictors of linkage to care, our study found that those who were a single or double orphan were more likely to link to care than nonorphans or those whose orphan status was unknown. There could be a number of reasons for this finding. One reason may be that more caregivers of orphans linked these CAs to care as compared with fewer nonorphan/orphan status unknown mothers, who did not link out of lack of disclosure issues and fear related to a partner learning of her own HIV status if she linked the CA. A qualitative study from Nigeria found that pregnant or new HIV-positive mothers feared disclosing their HIV status to a male partner out of concern for it being a threat to the marriage/relationship.23 The sister qualitative study to our own linkage to care study also found that disclosure of HIV status to a partner delayed CAs linkage to care (Malone, Submitted).
A second possible reason for the finding could be that HBCT direct engagement efforts and related follow-up at the household level acted in way that promoted linkage to care among orphans in particular. One study by Thurman et al24 in South Africa, for example, found that a home visitation program for orphans and vulnerable children (OVC) doubled the odds of an orphan being tested for HIV as compared with orphans who did not receive this program. Although HBCT itself is not a formal “home visitation program,” it may be that it acts in a similar way (engaging with the household at the home and discussing HIV), conferring some of the same benefits and promoting achievement of key milestones on the HIV Care Continuum, in this instance, linkage to HIV care.
Finally, a third possible reason for the finding could be if caregivers of orphans in the HCBT villages were engaged in OVC programs in the area that promoted linkage to care to achieve better HIV outcomes for these children as compared with children in the general community. Since 2017, the United States Agency for International Development has operated Mwendo project in the western Kenya area with a goal of improving health of OVC and HIV outcomes.25 Other OVC programs preceding this, one may have also been operating in the HBCT area and could have influenced linkage to care among orphans.
At the same time in which we saw that single and double orphans were more likely to link to care than nonorphans or those whose orphan status was unknown, we also saw that single and double orphans were more likely to die than nonorphans or those whose orphan status was unknown, although estimates related to death in our study were not precise given that numbers were small. One possible explanation for these mortality findings could be cost and time incurred to caregivers of some orphans. A 2009 systematic review by Kuo et al26 demonstrated that many AIDS-orphaned children were cared for by extended family members, in particular, older women, and that caregiving could cause increased burden (ie, monetary and family care) on the family with whom the orphan lives. Thus, it may be that some caregivers in our study did not routinely have funds for issues such as transporting the CAs to the clinic to link him/her to care or to obtain medicine, placing the CAs at greater risk of death. It could also be that the caregiver did not have additional time away from other family members to obtain care for the CA. Furthermore, neglect of the orphans may have been the cause.27 OVC programs should continue to work with caregiving families to identify support that promotes timely linkage to care for orphans.
Finally, our study demonstrated that CAs with HIV-positive mothers were more likely to both link to care and to die than those with HIV-negative mothers or with mothers whose HIV status was unknown. CAs who acquired HIV perinatally will have had HIV-positive mothers, and some mothers seeking HIV care for themselves may also have been more likely to link their CAs to care as compared with CAs with HIV-negative mothers (CAs acquired HIV sexually) or CAs with mothers whose HIV status was unknown. In these latter 2 instances, it may be that the mother was less likely to proactively provide HIV care for the CA and link him/her as she was not focused on her own health. Some evidence in the literature suggests children will follow a similar HIV treatment path as the caregiver/parent, although other evidence suggests the HIV treatment path of a child and his/her caregiver/parent is independent.28–30 Furthermore, our study also found that CA with HIV-positive mothers were more likely to die than those with HIV-negative mothers or with mothers whose HIV status was unknown. Some HIV-positive mothers may not have sought care for themselves or their CAs, or only themselves, leading to a greater number of deaths of CAs. This is in comparison with CAs with HIV-negative mothers (CAs acquired HIV sexually) or CAs with mothers whose HIV status was unknown.
All of this evidence supports PEPFAR's prioritization of the need for investment into family-focused HIV care programs to support mothers in ensuring they link their children and adolescents to HIV care. Testers and counselors aware of a mother's HIV-positive status should also advise mothers to link the CAs to care and for them to attend covisits together.29 Those adolescents who test positive but do not have mothers who are HIV-positive or whose status is unknown should also be provided support such as a peer navigator to help them link.31
Limitations and StrengthsThere are several limitations and a number of strengths to this study. First, some of the children and adolescents in our study knew they were previously HIV-positive at HBCT, and thus, time taken to link may have been underestimated given we only assessed time to linkage to care since the HBCT data collection occurred. Second, there may be additional individual, family, behavioral, or social characteristics not measured by our study that predict time to linkage or death. Third, many of the CAs in this study will have been perinatally infected with HIV given their ages (0–17 years), but there may be additional influences that should be considered on time to linkage to care for those adolescents who acquired HIV sexually. Fourth, although we attempted to reach all 97 children/adolescents and their caregivers in the follow-up study, we were unable to reach 11 to ascertain their outcome status (not included in modeling). Relatedly, we were only able to determine 20 children/adolescents were “alive with linkage to care status unknown”; however, we did conduct several sensitivity analyses exploring these individuals as linked (Fig. 2, Tables 2 and 3). Fifth, there could have been some under ascertainment of CA orphan status if parents died after possible moves/relocations for work or other reasons, but we anticipate this would be a small number of occurrences. Finally, it is possible that there were time-varying confounders that were unmeasured in our study given the length of follow-up time and lack of data between the HBCT encounter and the tracking visit.
Strengths of this study are robust and include a focus on linkage to HIV care among children and adolesc
Comments (0)