Summary of evidence
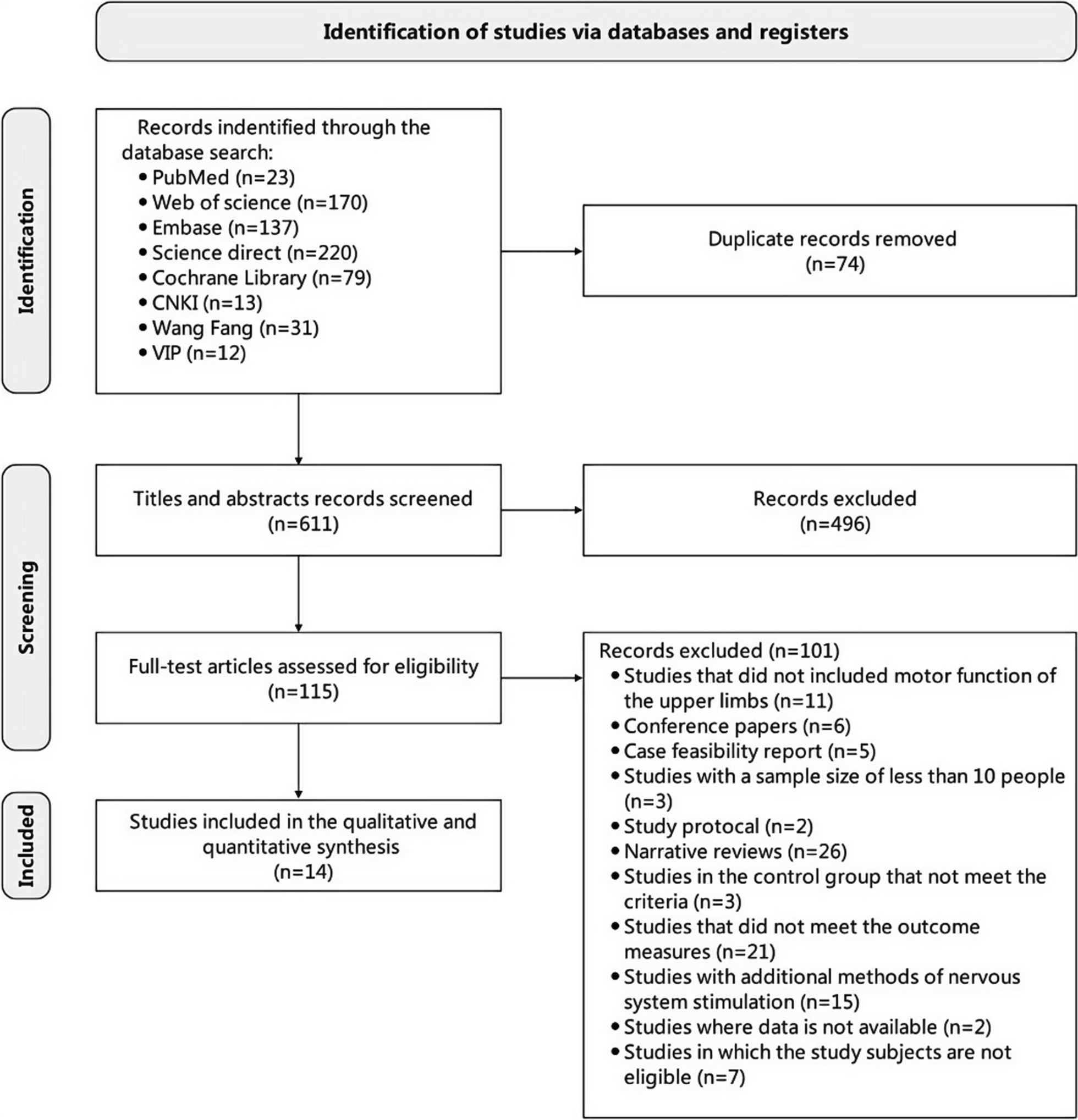
This systematic review and meta-analysis initially included 14 RCTs. However, two articles were divided into four studies, resulting in 16 studies (886 patients) included in the analysis to investigate the effects of MI combined NIBS on upper limb function after stroke. In addition, its effectiveness in motor function of the upper limbs, activities of daily living, functional activity of upper limb movements, and neurophysiological index (MEP-CL and CMCT) were analyzed. Studies have shown the crucial clinical significance of comparing combination therapy with NIBS alone or MI alone to assess real synergistic effects [26, 31]. This systematic review provided evidence that MI combined with NIBS therapy had positive effects on the recovery of upper limb dysfunction after stroke. Subgroup analysis showed that combinations of the stage of stroke, type of MI, type of NIBS may be key factors that can modulate the effects of MI combined NIBS therapy for upper limb function.
Clinical effects of MI and NIBS
Our findings were similar to a recent meta-analysis published by Monteiro et al. [7]. Although their study protocol presented a high degree of heterogeneity, the results indicated that training of motor imagery at least twice a week in the three weeks after stroke was effective in improving the motor performance of patients, suggesting that when motor imagery is used as a supplement to traditional rehabilitation techniques, it is an effective technique for treating post-stroke patients. However, a meta-analysis by Aprigio et al. [42] reviewing 412 stroke patients from 13 studies, including 232 in the intervention group and 180 in the control group. They evaluated motor function based on ARAT and FMA, finding no favorable results for MI training after stroke, which is inconsistent with this study. These previous studies focused only on the results of MI alone and not on the effect of MI combined with NIBS, which is different from our study.
Non-invasive brain stimulation has shown promising clinical results, leading to increased demand for an evidence-based review of its clinical effects [43]. Several systematic review studies have analyzed the effects of tDCS and rTMS on motor function recovery in stroke patients. According to the results by Keser et al. [44], evidence-based guidelines support Level A (definite efficacy) for the use of LF-rTMS of the primary motor cortex for hand motor recovery in the post-acute stage of stroke. A guideline and meta-analysis of the use of tDCS in the treatment of neurological and psychiatric disorders by Fregni et al.[45] found that when tDCS was combined with other therapies to treat subacute and chronic strokes, patients showed improvement, and tDCS enhanced the effect of adjuvant therapy. However, the effect size and duration of the effect are usually limited, and the true clinical impact needs to be further determined through different study designs.
Overall findingsThe upper limb function (FMA-UE, WMFT, ARAT)
FMA-UE is the most commonly used tool to evaluate upper limb motor function after stroke [46], and 13 articles in our study chose this scale as the basis for improving upper limb motor function. The results showed that after the intervention, the FMA-UE score of the combined group was significantly higher than that of the control group, indicating that the improvement of upper limb motor function of the combined group was significantly better than that of the control group. No significant heterogeneity was observed in the results of FMA-UE, indicating that the results were robust and reliable. Furthermore, the MCID serves as a metric to ascertain whether the change in outcome scores due to interventions is meaningful and constitutes a significant clinical improvement for patients [47]. However, the clinical significance of FMA-UE scores may differ across various patient groups and research settings, necessitating a case-by-case analysis [48]. For example, in the case of stroke patients with moderate to severe damage, an increase of 12.4 points in the FMA-UE score is typically regarded as signifying a meaningful clinical improvement [47]. The results of this systematic review and meta-analysis showed that MCID in the combined group exceeded 12.4 in eight studies, and no improvement to the MCID was observed in the control group, suggesting that only MI or only NIBS has limited clinical effect despite the intervention. We observed that the study populations failing to achieve the MCID were all chronic phase patients more than one-year post-onset. Moreover, a previous study has indicated that for chronic stroke patients, particularly those with residual severe upper limb hemiplegia, the MCID for FMA-UE scores has not been clearly defined, necessitating further research to determine the MCID value for this group [49]. Current evidence suggests that MI combined with NIBS is recommended for patients with severe injury, and MI combined with NIBS is not only statistically effective, but also clinically beneficial to patients.
Regarding functional activity of upper limb movements (such as WMFT and ARAT), 3 studies evaluated WMFT, and 3 evaluated ARAT. Similar to FMA-UE changes, these scores also showed better improvement in the combined treatment group compared to MI alone or NIBS alone. Similarly, no significant heterogeneity was observed, suggesting that the results were robust and reliable, and that MI combined with NIBS was more effective in improving the functional activity performance of the upper limbs in stroke patients.
Activity daily living (MBI)
MBI is the most commonly used measure of activities of daily living (ADL) after stroke, which shows the degree of independence of the patient and provides a quantitative estimate of the level of independence [50]. Ten studies in this study used MBI assessment criteria for activities of daily living. Similar to the results of FMA-UE, the MBI score of the combined group was significantly higher than that of the control group after the intervention, suggesting that the combined group was better than the control group in improving the ability of stroke patients to perform activities of daily living.
Cortical excitability (MEP-CL and CMCT)
When the motor cortex is stimulated by TMS, motor-evoked potentials are generated, and the latency of MEP can represent motor cortical excitability and corticospinal cord pathway integrity. CMCT is also a commonly used parameter of motor evoked potentials, which is the conduction time from motor cortical neurons to spinal cord motor neurons, mainly reflecting motor neuron and spinal cord anterior horn cell function [51, 52]. Only 4 studies in this systematic review reported using MEP-CL, and 2 studies evaluated CMCT. Interestingly, despite the theoretical similarity of MEP-CL and CMCT, the results of this study showed an inconsistent trend, contrary to our expectations, as some previous studies have shown that MI and NIBS increase corticospinal excitability [43, 53]. Similarly, Chen et al. [54] found that the duration of MEP-CL and CMCT in the experimental group was significantly shortened compared with the control group when discussing the impact of rTMS combined with motor learning training procedures (MRP) on stroke patients. The inconsistency between the two indexes in this study may be due to individual differences of the patients, trial design differences, as well as objective factors such as the position of the coil and the machine, which cannot be accurately measured to obtain the motor-evoked potential index under the same standard, and the motor evoked potential itself tends to fluctuate in different time states of the same patient. In addition, the small sample size may also be one of the reasons for this result. It is recommended to conduct a large sample size randomized controlled trial in the future to determine the effect of MI combined with NIBS on cortical excitability in stroke patients.
Phases of stroke during the intervention
For stroke patients at different stages, the effect of MI combined with NIBS seems to be different. For example, when compared with single therapy, MI combined with NIBS therapy is more effective at improving the FMA-UE score in the acute and subacute stages, but the effect is not significant for stroke patients in the chronic stage. Similar studies have also reached similar conclusions. For example, Ahmed et al. [55] conducted a meta-analysis of 1120 subjects and found that compared with false stimulation, NIBS combined with other therapies effectively improved the FMA-UE score of acute/subacute stroke, but could not change the FMA-UE score of chronic stroke. Brain plasticity is higher in the acute and subacute phases after stroke, which may be why MI combined with NIBS is more effective in these phases.
Taking into account the stage of the disease and the extent of the injury in the rehabilitation process are essential for developing a more accurate and effective program [56]. Given the limited training options for severely impaired chronic patients, we suggest that early intervention is important, so that the damaged neural network can still be reorganized, which may stabilize in chronic patients [57]. Second, chronic patients can be more personalized to their level of injury, such as different types of NIBS (HF-rTMS or LF-rTMS or a-tDCS or c-tDCS) and different types of MI (GMI or MI-BCI) to find the best treatment for the individual. Severely impaired patients may need more intensive or longer treatment, and other rehabilitation methods such as rehabilitation robots [58] and constraint-induced movement therapy [59] may be combined to improve the effectiveness of training. In addition, new technologies such as virtual reality have also explored for the training of MI combined with NIBS [60], which can help severely impaired chronic stroke patients obtain more immersive MI training through virtual reality, reduce fatigue, increase participation, and improve treatment effect.
Differences in types of MI
Considering the type of MI, 7 studies used general video and audio-guided MI, which provides a standardized guide to MI in which patients typically watch video materials and listen to audio instructions to perform specific actions, such as shrugging shoulders, raising hands, making fists, etc. It is simple and intuitive, using familiar sensory inputs to promote MI [25]. With the development of brain-computer interface technology, it provides a visual window for MI. Four studies used BCI real-time feedback-guided MI, which is performed by collecting changes in sensorimotor rhythms that occur in the brain during MI [30]. Since there is a gap in the individual motor imagery ability, MI-BCI can provide visual, auditory and tactile feedback help, so that patients may benefit more from MI training. Two studies used graded MI, which gradually increases the difficulty of MI tasks according to the patient's ability and stage of recovery, from simple MI to more complex and closer to daily living skills, based on personal experience and memory [31, 32].
Despite the advanced nature of MI-BCI technology, its effect in this study is not beyond the video and audio-guided MI and graded MI methods. Notably, no patients with BCI blindness were reported in any of the included MI-BCI studies, which prevented them from effectively using the BCI system and thus did not achieve a prefetch effect. However, the studies included did not employ a uniform assessment tool to quantify the participants' MI abilities. This difference may have influenced the interpretation of the findings to some extent. Thus, for future research, it is advisable to utilize standardized assessment instruments to measure MI capabilities. This will facilitate a more precise evaluation of the performance of MI-BCI systems and provide a more consistent baseline for comparing results across different studies. In light of the current evidence, it is recommended that video and audio-guided MI and graded MI be given priority in clinical practice, while continuously delving into the optimization of BCI technology.
Differences in types of NIBS
Clinically, different studies have used different types of NIBS to stimulate stroke patients. Our results showed that MI, whether combined with tDCS or rTMS, can significantly improve upper limb motor function (FMA-UE score), functional activity level (WMFT, ARAT score), activity of daily living (ADL score), and corticospinal excitability (CMCT). Similar findings were reported by a recent meta-analysis by Kang et al. [61], which evaluated the effectiveness of NIBS in improving the force production capability in paretic limbs and concluded that tDCS and rTMS regiments (increased cortical excitability of the affected cerebral hemisphere by a-tDCS and HF-rTMS; reducing the excitability of the contralateral cerebral cortex by c-tDCS and LF-rTMS) successfully improved paretic limb force production capabilities.
In addition, subgroup analysis in this study showed differences in MBI outcomes between LF-rTMS and bi-tDCS and a-tDCS subgroups, i.e., the type of NIBS had a significant interaction with the effect of MI combined with NIBS therapy, and the effect of LF-rTMS and a-tDCS was better than that of bi-tDCS. LF-rTMS in the unaffected cerebral hemispheres has been reported to be more effective in the chronic phase of stroke (grade B recommendation) [62]. A recent meta-analysis showed that HF-rTMS increased cortical excitability in the affected hemisphere at the stimulation site and improved impaired upper extremity motor function in stroke patients [63]. Research by Lefebvre et al. [64] suggests that when using tDCS, people should pay attention to which brain regions should be targeted and which stimulation types should be used. As shown in the Muffel et al. [23] study, which included 24 stroke patients randomly divided in two groups treated with bi-tDCS or a-tDCS, bi-tDCS showed a significantly greater beneficial effect on improving motor and sensory function compared with a-tDCS. The differences in therapeutic effects may be due to the fact that rTMS and tDCS are two distinct types of stimulation with different technological mechanisms, stimulation parameters, and targeted brain regions. However, due to the small number of studies extracted and the variability of reported stimulus parameters, we could not perform a sub-analysis to elucidate stimulus parameters for different NIBS, which limited our understanding of the positive changes in motor function promoted by NIBS. Neuroimaging data (fMRI) should be acquired prior to, during, and following treatment to elucidate the underlying neural mechanisms mediating treatment effects. Moreover, MRI-neuronavigation may address potential discordance between coil/electrode placement and region of interest, potentially improving treatment efficacy [65].
Stimulation timing and after-effect
Regarding stimulation time, the current MI training was about 30 min, and the NIBS time was about 20 min, which was taken as a classification in our study. These results may suggest that the time of MI and NIBS is not a direct factor affecting the effect, and it is necessary to conduct a more extensive study in the future to explore the best intervention duration of MI and NIBS to maximize the time and economic benefits of patients and make more people benefit from them. On the other hand, we note that most of the included studies reported only the total duration of MI in their intervention protocols, without specifying the repetition time and exact number of times to perform MI tasks, impeding the development of more structured protocols for MI.
This study showed that compared with a single therapy, stroke patients' upper limb motor function could be better improved regardless of the stimulation timing of MI and NIBS in the combination group. NIBS can promote motor recovery by activating or inhibiting activity in cortical areas, particularly when combined with appropriate motor training, they can optimize changes in brain plasticity and thus play a greater role in the recovery of motor function after stroke [66]. Kang et al. [67] also obtained similar conclusions, which could be explained by the priming stimulation mechanism. This theory suggests that “the brain that has been primed by prior activation is generally more responsive to the accompanying or subsequent training”. However, some preliminary evidence seems to support the notion that applying NIBS prior to activity execution can more effectively enhance motor performance, and that NIBS can prime cortical excitability for subsequent motor training tasks, thereby optimizing the processes of motor learning involved in standard rehabilitation therapies, leading to more pronounced and longer lasting functional gains [68,69,70,71]. As demonstrated by Cabral et al. [69] and Jo et al. [70], the absence of tDCS-induced effects when tDCS is applied during or after motor training may be due to the induction of meta-plasticity plasticity and the activation of homeostatic regulation mechanisms. Conversely, Jin et al. [72] proposed that applying tDCS during motor training may be more conducive to motor recovery. We speculate that different NIBS protocols (HF-rTMS, LF-rTMS, a-tDCS, c-tDCS, or bi-tDCS) may lead to inter-individual differences in therapeutic outcomes, and therefore their efficacy might vary. Consequently, the optimal timing of NIBS (ie, before vs during MI) is still open to question. In the future, the successful implementation of combined NIBS and MI will critically rely on improved understanding of their functional interactions and associated effects on neural plasticity. Greater understanding of the mechanisms of action of each approach is necessary in order to optimize their combined use in rehabilitation and realize the promise of a more effective means to promote functional recovery after stroke.
It is also worth mentioning the post-intervention follow-up, which was found in a total of 5 included studies. The subgroup analysis showed that the intervention effect varied at different time points. At the 2-week follow-up, the functional improvement of MI combined with NIBS therapy was still better than that of single therapy, indicating that this functional improvement was maintained in the short term. However, four weeks after the end of the intervention, there was no difference in the effects between the two, suggesting that the advantage of the combination therapy was lost. The reason for this fact may be that the initial effect of MI combined with NIBS is more pronounced, and the intervention time in the study is relatively short, which leads to the effect not being maintained for a long time. In addition, differences in individual characteristics and study design, as well as follow-up methods, may affect the assessment of long-term effects. Although the combination of MI and NIBS has shown positive effects in the follow-up, how to maintain this effect is still a challenge, and it is necessary to explore long-term effective intervention strategies.
Clinical implications and recommendations
MI combined with NIBS therapy can effectively improve the upper limb motor function and activities of daily living in acute and subacute stroke patients with severe injury, and this improvement has clinical significance. The safety of treatment and combination of various types provides patients with more personalized rehabilitation options, and the short-term effect is significant.
It is important to note that this systematic review and meta-analysis included only Asian studies, which may limit the generality of MI combined with NIBS in the treatment of upper limb function recovery after stroke. We speculate that different regional research priorities, genetic and cultural differences may be responsible for this phenomenon. Non-invasive treatment methods may be preferred in Asia, and the healthcare system and resource allocation differ from those in Western countries, which may affect the implementation and effectiveness of treatment [73]. It is suggested that future studies of NIBS combined with MI should be conducted on a global scale to improve the generality and applicability of the conclusions and to explore the influence of geography and culture on treatment outcomes in order to design personalized rehabilitation strategies for different regions.
As it has been highlighted in numerous studies, there are several issues regarding combining MI and NIBS that still need to be addressed. Personalized selection of the specific types of MI and NIBS is essential, as the appropriate combination of these factors can lead to synergistic effects that enhance therapeutic outcomes. Considering the individual differences in MI abilities, standardized assessment tools are required to evaluate and teach effective imagery techniques. We should educate patients on how to recognize and report any discomfort or side effects to ensure the safety of treatment. In the future, developing is necessary remote rehabilitation platforms that allow patients to conduct MI combined with NIBS training at home, thereby increasing the accessibility of treatment. At the same time, further promotion of its integration with other rehabilitation technologies, such as virtual reality, augmented reality, and electromyography biofeedback, will enhance patient engagement and therapeutic outcomes [74]. Through the collection and analysis of treatment data, the therapy protocol can be continuously optimized to enhance its general effectiveness, and advanced imaging techniques such as functional near-infrared spectroscopy and multimodal functional magnetic resonance imaging can be used to objectively monitor changes in brain activity after treatment to provide direct evidence of treatment effectiveness, thereby enhancing the medical community and patients’ acceptance of this treatment regimen. Additionally, conducting long-term studies are essential to assess the long-term effects of MI combined with NIBS treatment. This not only helps in understanding the sustainability of the therapeutic effects but also evaluates its impact on patients' quality of life and social participation. Therefore, taking these aspects into comprehensive consideration will provide patients with more comprehensive, safer, and more effective treatment options.
Limitations
The present study has some limitations. First, the number of included studies was small, with only 7 articles in English and 7 in Chinese. Second, the research design of the included articles in this study was quite different, and the methods of allocation hiding and blinding were different in the included population, some of which were not mentioned in the article. Third, due to the small number of studies addressing the electrophysiology indicators and the different equipment used in different studies, understanding the role of MI combined with NIBS in promoting cortical excitability is limited. Fourth, routine rehabilitation varied slightly across studies in addition to the set intervention. Fifth, there was a high degree of heterogeneity in MBI evaluation results, which diminished the power of the findings and their implications for clinical practice. Sixth, it remained unclear whether age, injury severity, and injury type affect the outcome of MI combined with NIBS. These factors should be considered when forming a uniform sample to determine whether these factors are essential for movement improvement after combination therapy. Finally, the monitored study outcomes differed across studies, limiting the ability to compare outcomes and the inconsistencies in the results.


Comments (0)