This study presents long-term 10-year visual acuity and clinical outcome data for patients following retinal detachment repair. Results demonstrate, as expected, that patients presenting with a macula-on retinal detachment have an excellent prognosis. Macula-off patients had a poorer 10-year BCVA, with a significant negative relationship between duration of macular detachment and BCVA at 10 years. However, most meet the UK driving acuity standard after 10 years and BCVA continues to improve past initial follow-up. Redetachment was uncommon and conferred a poorer 10-year BCVA.
In our cohort of macula-on retinal detachment patients, the mean 10 year BCVA of 0.11 logMAR compares favourably to the Primary Retinal Detachment Outcomes (PRO) study, which reports postoperative mean visual acuity for macula on patients of 0.22 LogMAR (20/33) in both phakic and pseudophakic patients (mean follow-up 399 and 388 days respectively) [9, 10]. Difference in results may in part be explained by the limited follow-up of little more than 1 year in the PRO study, given our results show BCVA to continue to improve past this timeframe, albeit in macula-off patients.
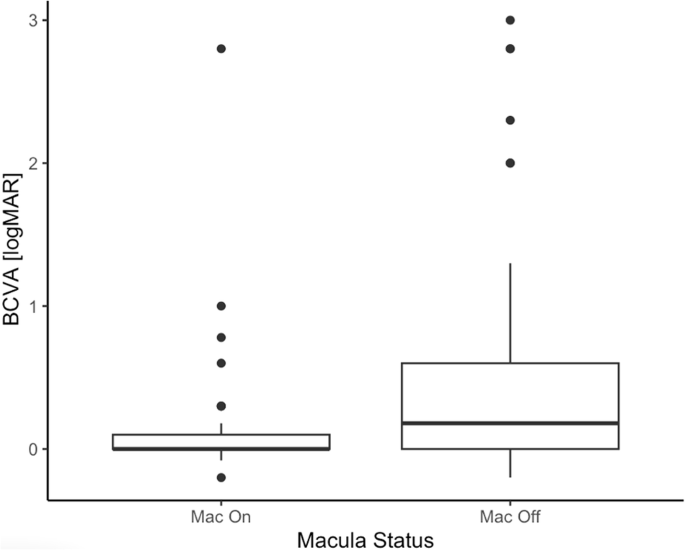
In macula-off patients, we demonstrate that BCVA continues to significantly improve years after repair, and that 65.2% achieved BCVA sufficient for UK driving standard (<0.3 logMAR), and 69.6% achieved 6/18 (<0.4 logMAR). Again, this compares favourably to reference data, with RCOphth NOD audit describing 46.3% achieving 0.3 logMAR (6/12) at 6 months, and the Scottish Retinal Detachment Study reporting 65.9% at 0.4 logMAR (6/15) at 1 year [3, 5]. Although some of the differences in our study may be explained by subsequent cataract surgery, both our data and previous work show continued improvement in BCVA after more than 1 year. The mechanism for this improvement is described by Fig. using en-face OCT analysis of the ellipsoid zone. They demonstrate that improvement in both retinal structure can continue for years after retinal detachment repair, and is associated with improved function [18].
Due to the emergent nature of retinal detachment repair, there is a lack of prospective evidence regarding the relationship between duration of macular detachment and reduction in long-term visual acuity. The Royal College of Ophthalmologists, under guidance from the British and Eire Association of Vitreoretinal Surgeons, suggests that macula-off detachments should be repaired as soon as possible, preferably within 3 days [3, 19]. In practice, evidence suggesting that post-operative visual acuity decreases the longer the macula remains detached is weighed against limited resource (manifest by a large variety in theatre capacity and availability of vitreoretinal specialists between different regions) throughout the UK and Ireland [20, 21]. Yorston et al. show that duration of macular detachment is associated with poorer outcomes. This agrees with our work with a trend to significance in the relationship between BCVA at 10 years and duration of macular detachment. However, our data show no significant difference in BCVA between those <3 d and >3 d of macular detachment in comparison to their results which recommend 72 h as a cut-off for repair [19].
A redetachment rate of 14% is similar to previous published data [3, 6,7,8]. Patients were more likely to redetach if they had not had a vitrectomy, though generalisation of this finding is limited due to the smaller sample size of the redetaching cohort. Ten-year BCVA was poorer in those who had a redetachment, but this is likely at least partly due to a greater proportion of the redetachments being initially macula-off.
The development of cataract is significantly accelerated by vitrectomy. Our results show only 9.8% remained phakic 10 years after vitrectomy, similar to that of Yee et al. who found 87% of patients had cataract surgery within 24 months following extensive vitrectomy for vitreous opacities similar to 80% of patients 29 months after vitrectomy for ERM [22, 23]. The likely need for subsequent cataract surgery is an important part of the consent process for retinal detachment repair with vitrectomy, especially if the patient is aged over 50. It was therefore interesting to note that 4 of 41 patients initially treated with vitrectomy remained phakic long-term, though degree of cataract was not assessed. Two had BCVA > 6/9, but 2 had counting fingers or worse though with a history of amblyopia.
The main limitation of this study is the attrition bias inherent in any long-term follow-up study. To maximise the sample size, we used the most recent BCVA recorded in hospital or by an optometrist. We collected 10-year outcome data for around half of all retinal detachment patients originally included in the study, which we feel is both satisfactory and expected, especially in light of patient migration, use of different primary eye care providers and lack of long-term follow-up in the hospital eye service. The use of ‘duration of central vision loss’ as a proxy to ‘days of macula detachment’ should also be considered. These are not necessarily equivalent as some patients remain ‘asymptomatic’ despite macular detachment, and relying on patient reported data reduces data precision and introduces recall bias [24]. However, this issue is not unique to our study and is one of the reasons that high quality data in this area lacking.

Comments (0)