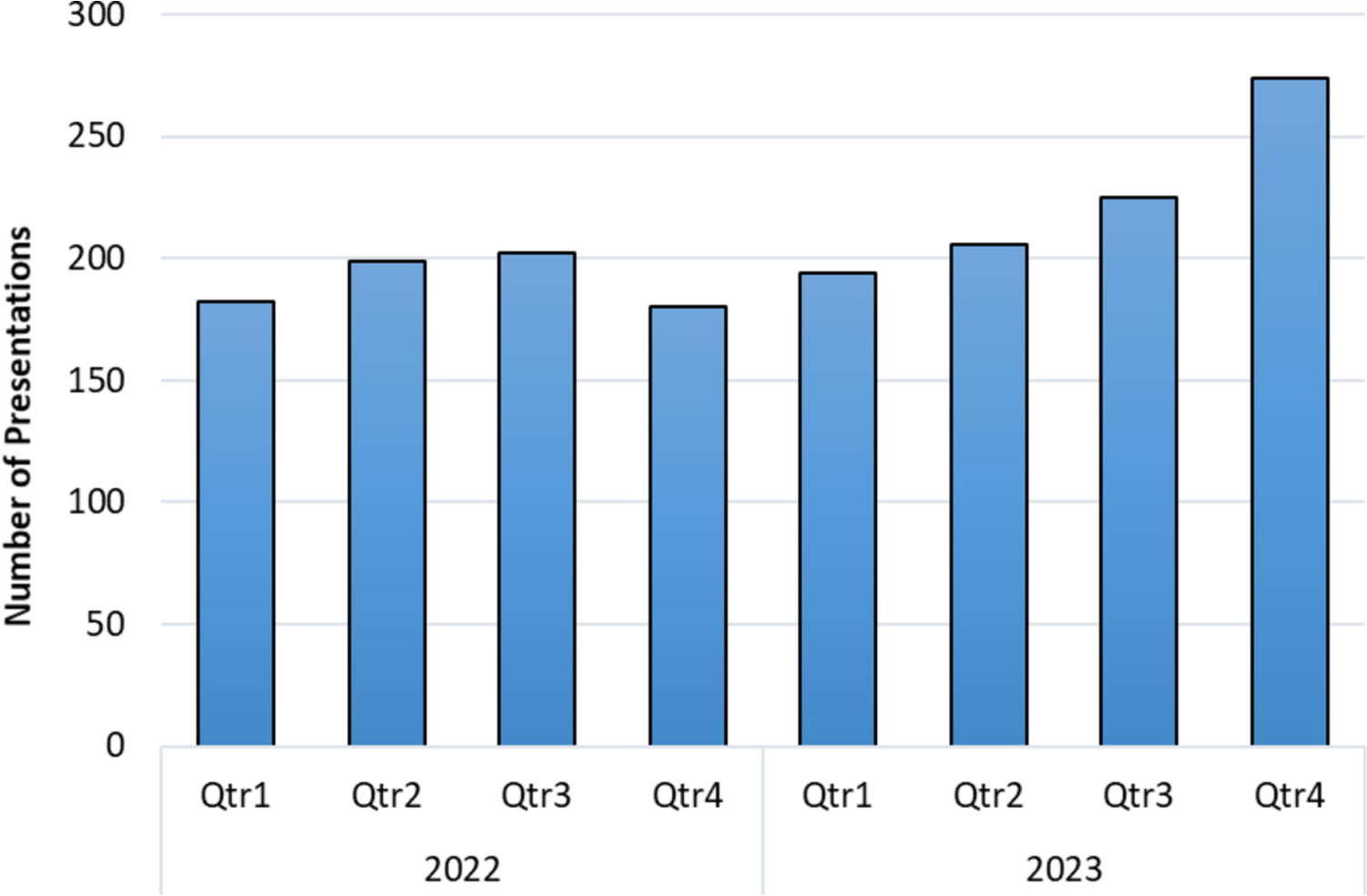
The study underscores the significant impact of alcohol-related presentations on the ED at MUH, emphasizing critical public health concerns. The findings revealed that 1662 presentations, representing 3% of all ED visits over the 2-year period, were categorised as “Apparently Drunk”. This 18% increase from 2022 to 2023 indicates a growing trend that necessitates immediate attention. The majority of these patients were male, with distinct age groups being more affected: males aged 30–39 years and females aged 20–29 years. This demographic trend aligns with existing literature suggesting that young adults and middle-aged individuals are particularly vulnerable to alcohol.
Implications of findings
The data revealed that 23% of these presentations were from people experiencing homelessness, highlighting a significant intersection between alcohol and housing instability. Frequent presentations by people experiencing homelessness underscore the need for integrated health and social services to address the underlying issues contributing to repeated ED visits. This intersectionality suggests a broader social problem of multiple disadvantages where homelessness and substance abuse are mutually reinforcing issues that require comprehensive and coordinated intervention strategies. Limitations in accessing primary care and other health and social services may also contribute to these ED presentations.
Moreover, there were notable differences in the proportions of people experiencing homelessness, patients with immediate triage urgency, and admitted patients between 2022 and 2023. This suggests a possible increase in the severity and complexity of alcohol-related ED presentations, further straining hospital resources. Part of this observed difference may also be a result of changes in social behaviour and access to or use of alcohol related to the COVID-19 pandemic.
Associated injuries and concurrent issues
The spectrum of alcohol-related harm is extensive. The data showed that 7% of patients presented with head injuries, 6% with injuries from falls or collapses, 5% had concurrent mental health issues, and 4% reported assaults.
These injuries not only affect the individuals but also place additional burdens on the healthcare system, requiring specialised care and resources. The high prevalence of injuries and mental health issues among these patients calls for targeted interventions that address both physical and mental health needs.
For those with head injuries, 3% are known to have had an intracranial haemorrhage. The majority (82%) of the patients with head injuries were managed clinically and did not require advanced imaging. This places a significant responsibility on the clinicians to ensure they do not expose patients to radiation, unless absolutely necessary. Almost one in five (18%) patients with a head injury noted at triage did have advanced imaging performed. This part of the service evaluation adds to our knowledge of the complexity involved in assessing and managing this challenging cohort of patients. This also has implications for how we may improve our service and the amount of advanced imaging that is required.
Ambulance utilisation and ED resource burden
The high percentage (81%) of patients conveyed by ambulance underscores the significant strain on emergency medical services. On average, two ambulances per day were dedicated to transporting patients categorised as “Apparently Drunk”, diverting resources from other critical emergencies. This utilisation pattern suggests that alcohol-related incidents are not only a hospital burden but also a substantial operational challenge for emergency medical services.
Policy implications and future directions
Policies like the Public Health Alcohol Act of 2018, which introduced minimum unit pricing, advertising restrictions and forthcoming health warning labels, represent positive steps towards mitigating alcohol-related harm. However, the study’s findings are particularly pertinent in light of the proposed Sale of Alcohol Bill (2022), which aims to extend alcohol trading hours and increase the availability of alcohol outlets.
International evidence suggests that extended trading hours are associated with increased alcohol-related harm, including higher rates of crime, traffic collisions, domestic violence, and other injuries requiring hospital treatment [6,7,8,9]. Additionally, the opposite is true with reductions in alcohol trading hours resulting in less alcohol-related violence [7, 10]. Rural communities may be particularly affected as Norwegian data suggests that extending bar closing hours increases the number of traffic collisions [11].
The potential exacerbation of alcohol-related ED presentations due to increased alcohol availability presents a significant public health risk. Policymakers must weigh the potential benefits of economic gains from extended trading hours against the likely increase in public health and safety risks.
A possible policy intervention that could reduce alcohol-related harm and violence is the introduction of the Cardiff Model, a data monitoring system between hospitals and the police [12]. The Cardiff Model involves the anonymous and routine collection of data on the location, time, and weapon used in violent incidents from patients presenting to the ED [12]. These data are then shared with the police and local authorities to inform crime prevention strategies and target high-risk areas. The Cardiff Model has been shown to reduce violence-related hospital admissions by 35% and serious violence reported by the police by 42% [12]. This is particularly relevant to our study because of the location of MUH in the city centre and the relatively high number of assaults and injuries among our patients. Implementing the Cardiff Model could help reduce the burden of alcohol-related violence on the ED and the community.
Comparison to other literature
This study reports a comparatively smaller proportion of patients presenting to the ED with an alcohol-related issue compared to other recent Irish literature. McNicholl et al. [3] reported 5.9% of presentations to all EDs in Ireland, and Maharaj et al. [4] reported that 19.4% of presentations to Beaumont ED were alcohol-related. However, when comparing the findings of these studies to this study, it should be noted that the time period is not comparable. McNicholl et al. [3] studied four different 6-h periods selected in December 2015 and January 2016. Maharaj et al. [4] conducted their study over four 1-week periods between 4 pm and 4 am during the 8th to 15th of November, 28th of November to 4th of December 2021, 28th of February to 7th of March, and 3rd to 9th of April 2022. In addition, that study only included patients willing to participate in the survey and had a response rate of 73% [4]. In contrast, this study included all ED presentations to MUH over a 2-year period. As alcohol-related presentations are less frequent during weekdays and during the day, this may partially explain the lower proportion of alcohol-related ED presentations. On the other hand, the data presented may underestimate the true rate of alcohol-related presentations in MUH as the data source used was not designed for this purpose.
Limitations
Several limitations were acknowledged:
Data reliability: The reliance on routinely collected data, not originally intended for service improvement analysis, may introduce inaccuracies or missing data.
Underreporting of alcohol-related presentations: Not all alcohol-related presentations may be captured under the “Apparently Drunk” code, possibly leading to an underestimation of the true burden of alcohol-related cases.
Variability in triage coding: As the triage code “Apparently Drunk” is applied based on the subjective assessment of triage personnel, its use and interpretation may vary, leading to potential inconsistencies. For example, some patients categorised as “Apparently Drunk” may not be intoxicated at the time of presentation, but this code was applied because the injuries sustained were deemed to be a result of alcohol. Intoxication with other drugs/substances also cannot be excluded. Additionally, associated injuries or co-presenting complaints may not be recorded consistently as only one presenting complaint is required by IPMS, and therefore, it is possible that not all presenting complaints are captured.
Recommendations
1.
Enhanced public health interventions: There is a critical need for targeted public health interventions to reduce alcohol consumption.
2.
Reduce alcohol-related violence: Consideration should be given towards implementing the Cardiff Model, or similar, in Cork City. Collaboration and data-sharing between the city council, Gardaí, MUH, and Public Health may enhance the combined response to alcohol-related violence and lead to a safer community.
3.
Integrated services for people experiencing homelessness: Given the high proportion of people experiencing homelessness, integrated health and social services should be developed to address both alcohol use and housing instability.
4.
Policy considerations: Policymakers should carefully consider the potential public health implications of the Sale of Alcohol Bill (2022) and prioritise policies that mitigate alcohol-related harm.





Comments (0)