
Remember me
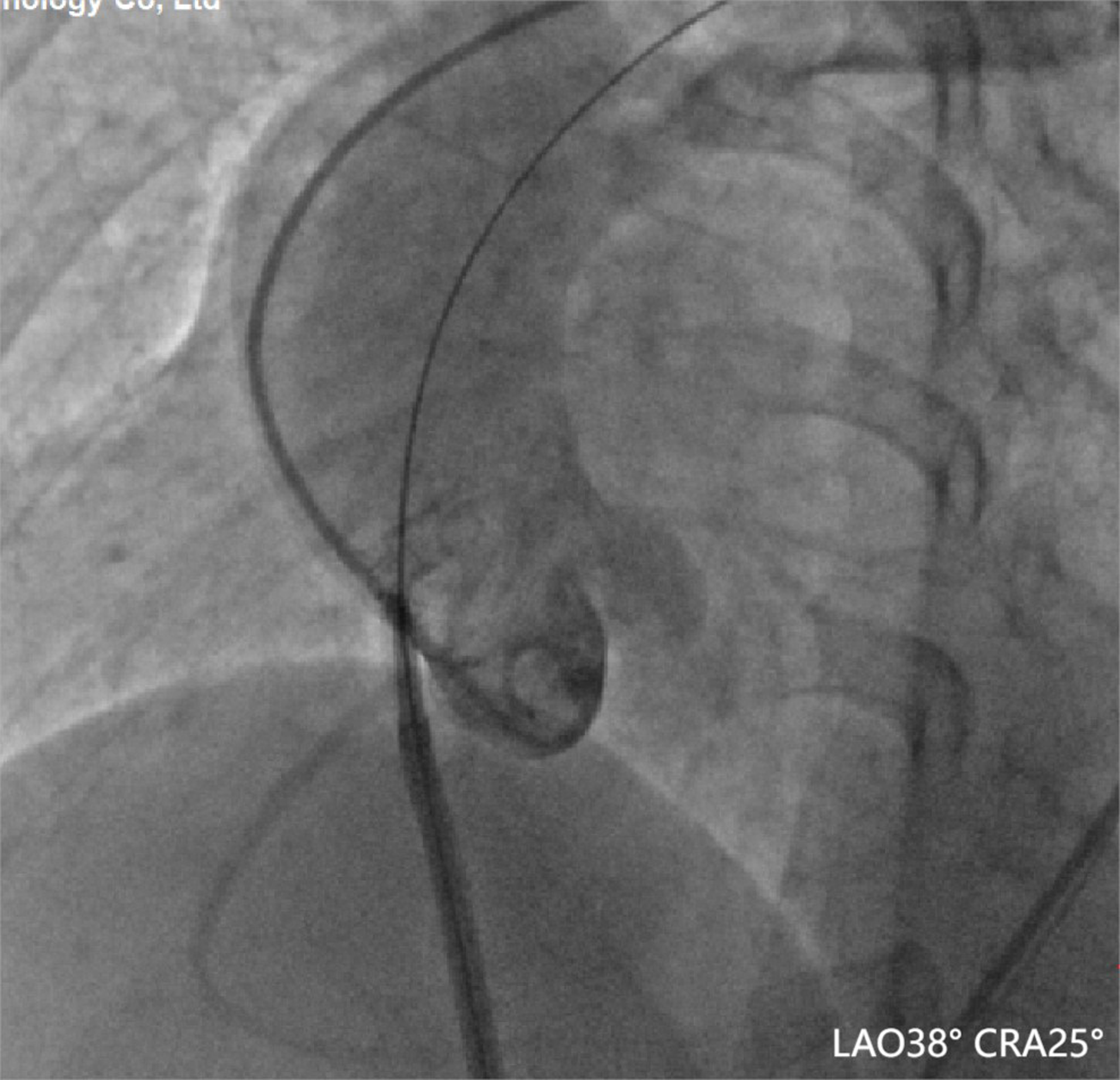
Transseptal puncture is a technique that is routinely performed in mitral valvuloplasty, catheter ablation for AF, and left atrial appendage closure. Complications associated with transseptal puncture occur in 1% of procedures. In one report of 3756 patients who underwent transseptal puncture procedures, only three aortic root perforations were observed [1]. Nevertheless, our case demonstrates that transseptal puncture guided by transthoracic ultrasound and radiography remains difficult, owing to the unusual anatomy of the region. Intracardiac echocardiography-guided puncture can be performed to avoid serious complications during transseptal puncture procedures, particularly in patients with a large atrium or unusual anatomy [2]. If a patient has a large atrium, it is also necessary to reshape the needle to provide greater curvature (Fig. 6). The coronary sinus catheter and the pigtail catheter in the aortic root can also be used to guide transseptal puncture [3].
Fig. 6
The needle was reshaped to provide greater curvature in this case
Cardiac tamponade may not occur if the sheath is not advanced, thus creating a much larger hole. Unfortunately, we did not perform pressure tracing and instead advanced the Swartz sheath into the ascending aorta, which was not prudent at that stage. Previous studies have shown that cardiac tamponade usually occurs immediately and requires surgical treatment [4]. However, percutaneous management may represent a feasible option in the case of hemodynamic stability. A previous report revealed that a similar perforation was closed via an Amplatzer™ duct occluder [5]. Considering the inherent advantages of the muscular VSD occluder for defects > 6 mm and < 3 mm in size [6], as well as the perforation size and physician clinical experience, the VSD occluder may better fit the ascending aorta perforation than the Amplatzer™ duct occluder does. Therefore, we selected an 8-mm muscular VSD occluder. An in vitro test revealed that an 8-mm muscular VSD occluder could be used for right atrium-iatrogenic ascending aortic perforation through an 8.5 F (2.8 mm) Swartz sheath. During the observation period, we found that this percutaneous strategy was viable and effective. Reversal of heparinization with protamine sulfate is unnecessary if there is no evidence of active bleeding [5]. In our case, this measure was not considered.
Percutaneous closure of ascending aortic perforations via a muscular VSD occluder is a viable treatment approach. Our case highlights the fact that timely evaluation and effective intervention are crucial for avoiding adverse outcomes.
Comments (0)