
Remember me
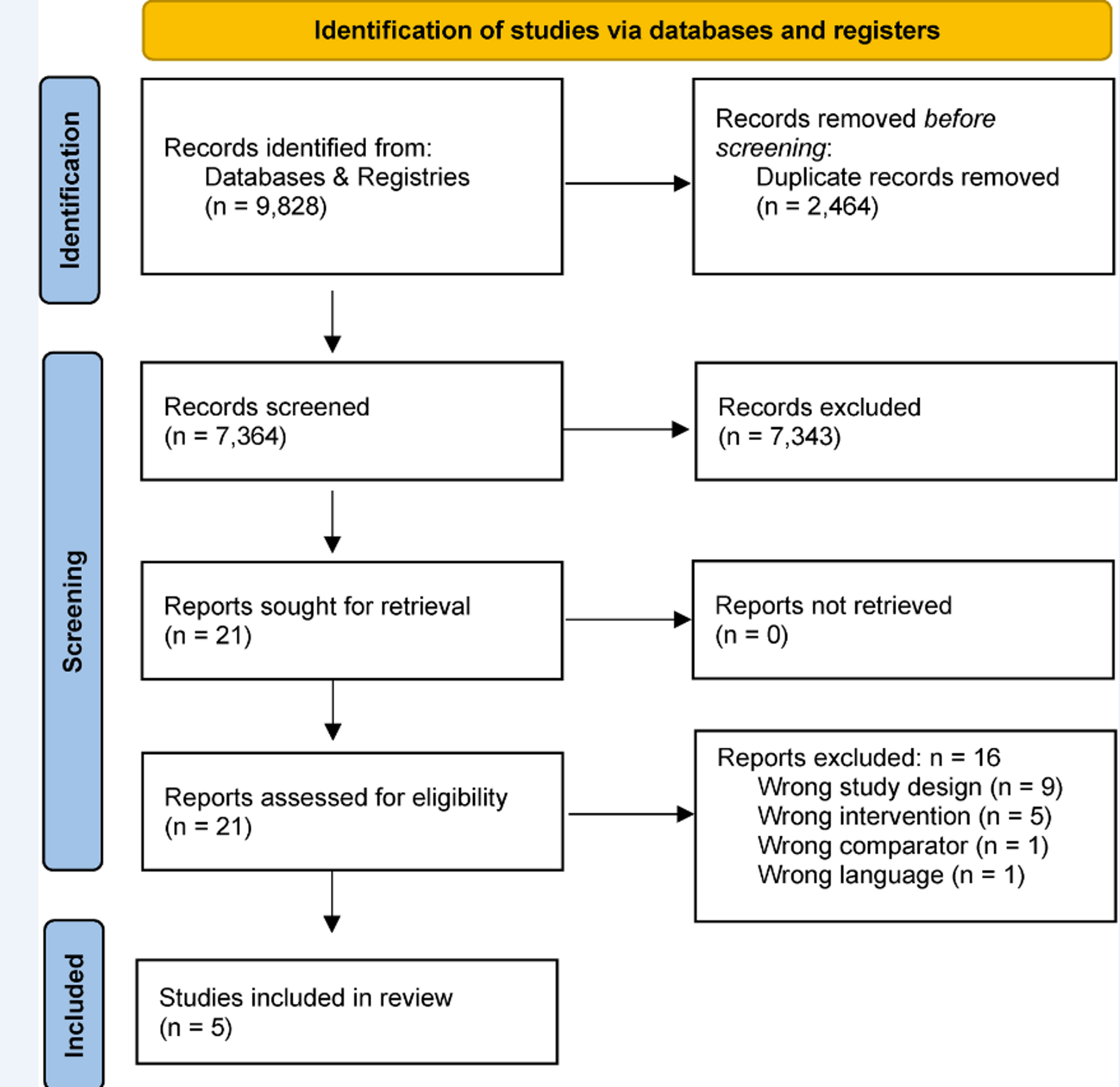
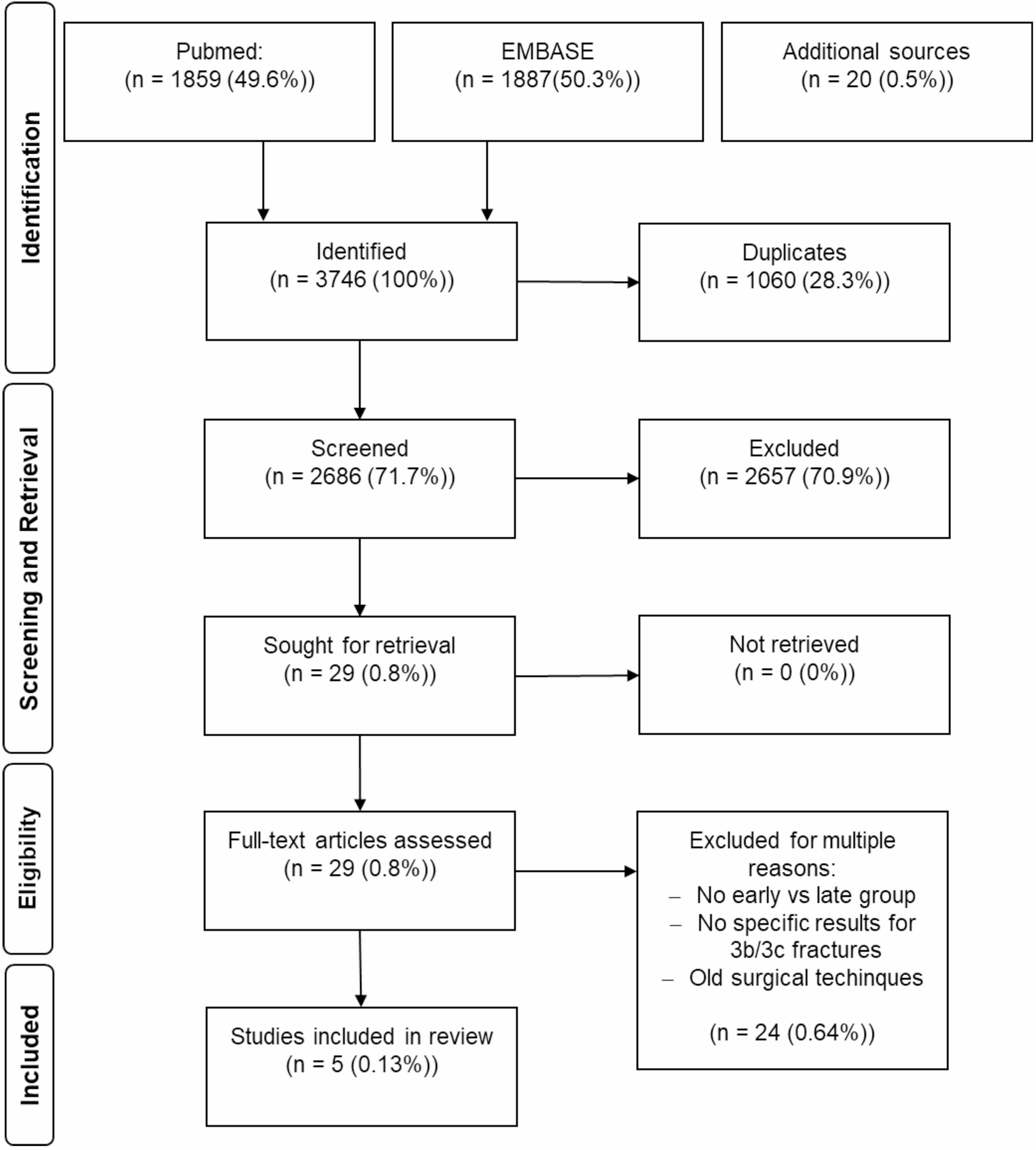
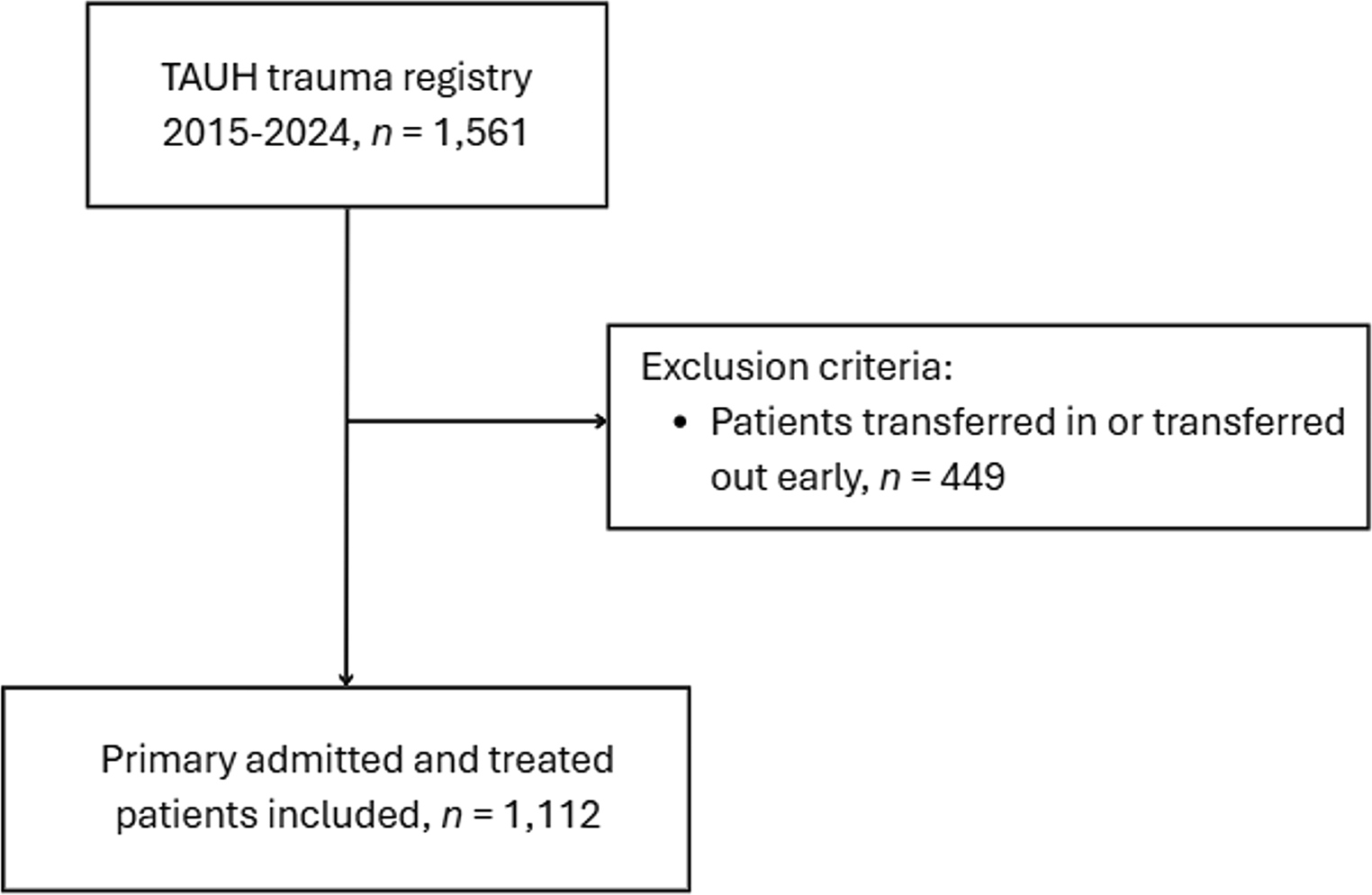
The search identified 990 records (Fig. 1). After removing all duplicates, title abstract screening was performed on 818 records. After that, 815 studies were excluded and of the remaining two studies the full texts were screened. Reasons for exclusion of these two studies were “not meeting the definition of multiple trauma” (n = 1 [6];) and “no handover tool used” (n = 1 [7]). Given the identified evidence gap, the results of those studies reporting any effects of handover tools were reported in this review. In total, 26 studies of the 818 screened records were assessed. In this way, descriptive effects, offering valuable insights into tool utilization were summarized. This broader inclusion facilitated the capture of descriptive trends and patterns in handover tool implementation and effectiveness, enriching our understanding despite the absence of statistically rigorous evidence.
Fig. 1
Flow chart of the systematic review selection process
Study characteristicsThe study characteristics are presented in Table 1. Study designs varied, with 13 studies employing a observational study design [8,9,10,11,12,13,14,15,16,17,18,19,20], four utilizing qualitative methods [21,22,23,24], three involving randomized trials [25,26,27], and one each for multiphase mixed-method study [28], single-centered controlled study [29], retrospective analysis [30], prospective cohort study [2], mixed methods [28], interventional comparative study [31] and prospective intervention study [32]. In the context of the study settings, 18 of the included studies (69.2%) incorporated (ICUs, while the remaining 8 studies (30.8%) did not have ICUs as part of their settings. Moreover, in relation to the inclusion of polytrauma cases, 5 studies (19.2%) specifically addressed polytrauma patients, whereas the remaining 21 studies (80.8%) focused on different patient populations.
Table 1 Study characteristicsThe use of the handover tools was tested in various scenarios, which can be subdivided as follows: patients in the ICU without trauma (n = 16), patients in the ICU with trauma (n = 3), patients who were not in the ICU and had no trauma (n = 4), and those who were not in the ICU but had trauma (n = 1).
Utilized handover tools individual studiesIn 12 out of the 26 studies examined, standardized tools were implemented as part of their methodology (see Table 2). The most frequently employed standardized tool was SBAR, which featured in seven studies. One of these studies conducted a direct comparison with the Vicur tool. Additionally, the UW-IPASS, SBARQ, and the Targeted Solution Tool were utilized each in the remaining studies, further exemplifying the diverse range of standardized tools in use.
Table 2 Description of Handover tools used in included studiesIn another 12 studies, the focus was assessing the effectiveness of customized handover tools. In the remaining two studies a customized ICU discharge letter and a door communication card were chosen as a tool for handover. Table 2 provides a detailed overview of the tools and strategies employed within the included studies, Fig. 2 gives an overview of the positive effects reported.
Fig. 2
Overview of positive effects reported due to handover tools in hospitals: customized vs. validated tools
Treatment improvementTwo types of handover tools were identified: custom-designed tools and well-established validated tools. Among the studies that employed custom-designed tools, three did not identify any positive effects [13, 27, 29]. These outcomes included enhancements in information quality and quantity, improved communication among healthcare staff, as well as increased psychological safety and perceptions of accuracy and completeness. Additionally, two studies explicitly noted a reduction in risks and a decrease in treatment errors, see Table 2 [15, 16].
One study, which compared different standardized tools while also assessing their overall impact, did not find any positive effect [27]. Among the studies that employed a well-established standardized tool, twelve studies documented beneficial outcomes [2, 9, 14, 17, 21, ,25,26,27,28, 30,31,32]. These positive results were characterized by improvements in communication and documentation, heightened satisfaction among medical professionals regarding handovers, and enhancements in managing challenging cases and referral issues. Additionally, these studies observed a reduction in incidents of lost information and communication lapses, see Table 2.
Comments (0)