
Remember me
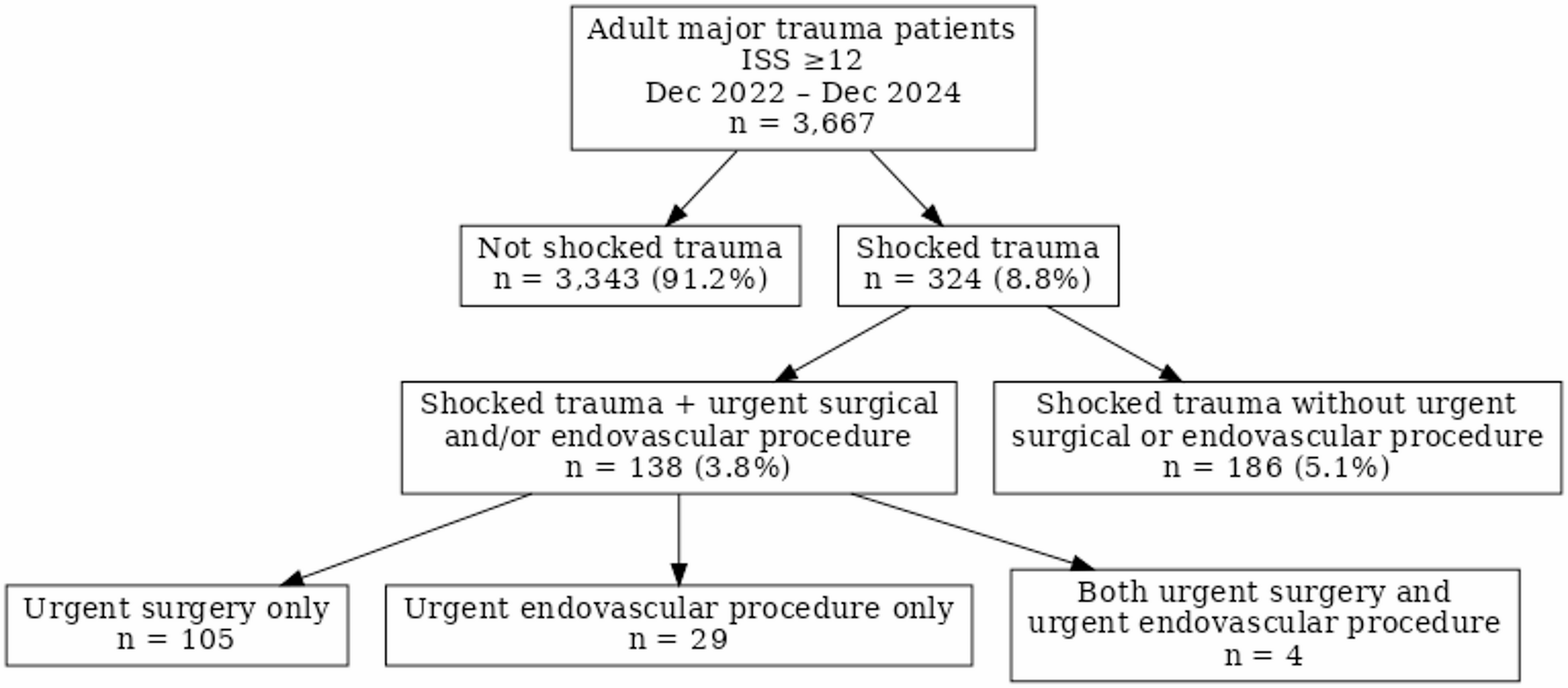
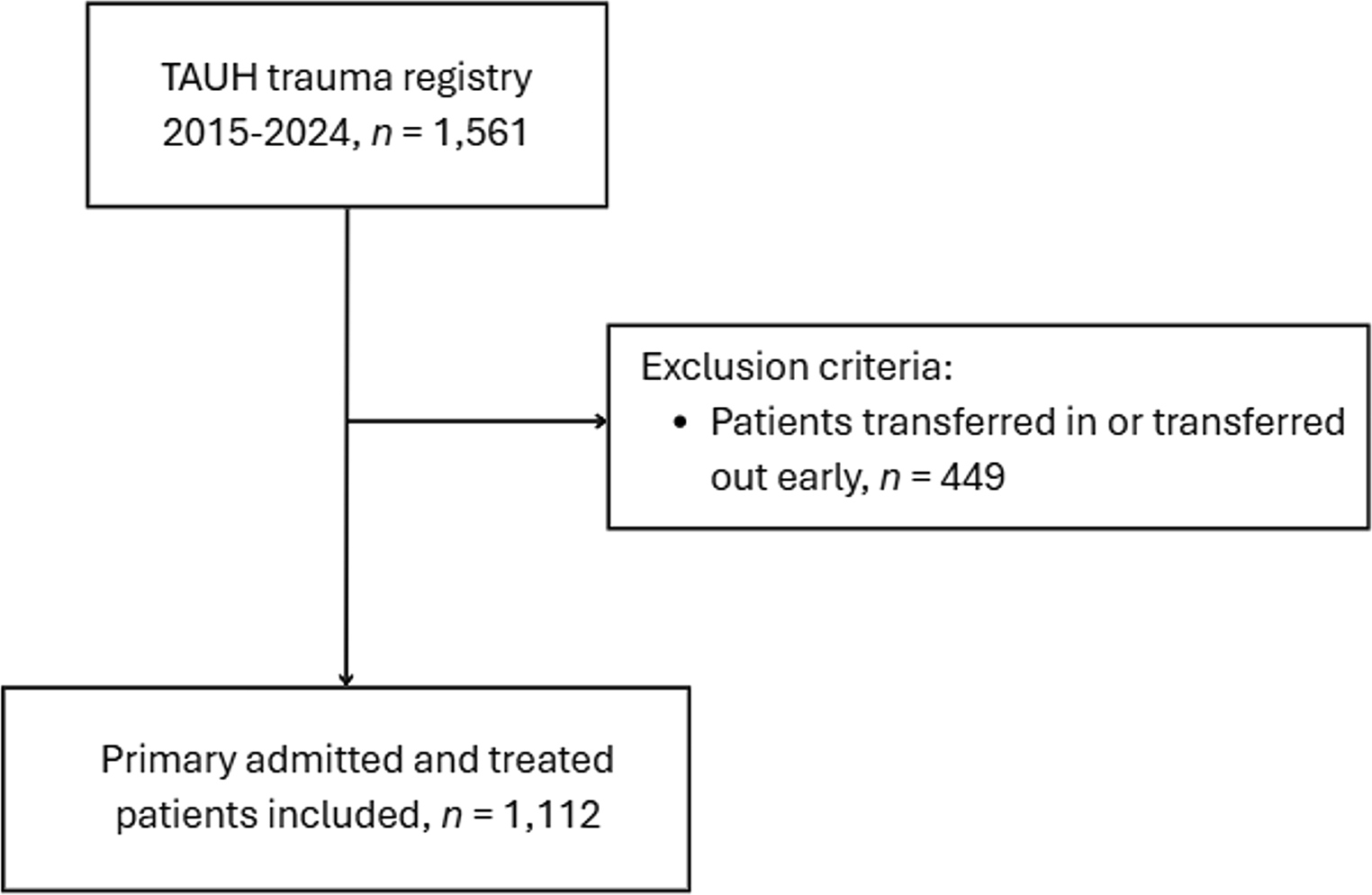
Over the study period, 3,667 adult major trauma patients were identified, of whom 324 (8.8%) met clinical criteria for traumatic shock. Among shocked patients, 138 (42.6%) underwent an urgent surgical or endovascular intervention, representing 3.8% of the total major trauma cohort (Fig. 1). Polytrauma was present in 24.6% of the overall major trauma cohort, 63.6% of shocked patients, and 65.9% of those undergoing urgent intervention.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.CONSORT flow diagram of major trauma patients by clinical shock status and urgent intervention (December 2022–December 2024)
Within the shocked cohort, patients requiring urgent surgical or endovascular intervention were younger and had similar injury severity compared with those managed without urgent intervention (Table 1).
Table 1 Baseline characteristics of major traumaa patients with clinical signs of shock by urgent intervention status (December 2022–December 2024)Critical care utilisation and outcomesICU admission was common among shocked patients and occurred more frequently in those requiring urgent intervention (94.9% vs. 83.9%) (Table 1). Among ICU-admitted patients, ICU length of stay was longer in those requiring urgent intervention, with a median ICU LOS of 8.0 days compared with 5.9 days among those managed without urgent intervention (Table 1).
In-hospital mortality differed between shocked patients with and without urgent intervention, with lower mortality observed among patients undergoing urgent surgical or endovascular intervention (13.8% vs. 29.0%). Notably, 22 deaths occurred in the emergency department prior to operative decision-making, all among patients who did not undergo urgent intervention (Table 1).
Blood product and fluid resuscitationPre-hospital blood product administration occurred in approximately one-third of shocked patients, with similar rates among those who did and did not undergo urgent intervention. In-hospital blood product use was common, occurring in 85.2% of shocked patients and 93.5% of those requiring urgent intervention (Table 2).
Table 2 Blood product resuscitation characteristics major traumaa patients with clinical signs of shock by urgent intervention status (December 2022–December 2024)Median early PRBC transfusion volumes were modest, with a median of 2 units within the first 5 h among shocked patients without urgent intervention and 4 units among shocked patients requiring urgent intervention. However, a substantial minority received high-volume transfusion. Delivered massive transfusion (≥ 5 units PRBC within 5 h) occurred in 42.8% of shocked patients undergoing urgent intervention, and ≥ 10 units PRBC within 24 h occurred in 25.4% of this group, compared with 15.4% among shocked patients managed without urgent intervention (Table 2, Appendix Table A2). Median PRBC: FFP ratios approximated 1:1 in both groups, consistent with balanced transfusion practice during early resuscitation (Table 2).
Transfusion burden and heterogeneity among shocked patientsDespite modest median transfusion requirements, marked heterogeneity in blood product utilisation was observed within the shocked cohort. Cumulative 24-hour PRBC transfusion volumes were significantly higher among shocked patients requiring urgent surgical or endovascular intervention compared with those managed without urgent procedures (Wilcoxon rank-sum test, p < 0.001).
High-volume transfusion (≥ 10 units PRBC within 24 h) occurred more frequently in the urgent intervention group (25.4% vs. 8.1%; odds ratio 3.87, Fisher’s exact test, p < 0.001). Visualisation of transfusion distributions demonstrated substantial overlap in early transfusion volumes between groups, with progressive divergence over time. High cumulative transfusion volumes at 24 h were predominantly observed among patients requiring urgent operative or endovascular intervention, consistent with more profound haemorrhage in this subset of shocked patients (Supplementary Figure S1).
Index resuscitation, surgical and endovascular proceduresIn-hospital resuscitative adjuncts were common across the shocked cohort, with 59/324 (18.2%) patients undergoing pleural decompression. Bilateral pleural decompression occurred more frequently than unilateral decompression (12.3% vs. 5.9%). Emergency department resuscitative thoracotomy was performed in 6/324 (1.9%) shocked patients (Table 3).
Table 3 Index resuscitative, surgical and endovascular interventions in shockedb major traumaa patients undergoing urgent interventionc*Among patients undergoing urgent intervention (n = 138), laparotomy was the most common index surgical procedure (23.2%), followed by neurosurgical and thoracic procedures. Endovascular interventions were less frequent and predominantly involved pelvic and splenic arterial embolisation. Patients undergoing both surgical and endovascular procedures were included in multiple categories as appropriate (Table 3).
Operative pathways and timingCombined urgent interventions involving more than one surgical or endovascular specialty occurred in 37.7% of patients requiring urgent intervention. Multiple operative episodes were common, with 74.6% of patients undergoing urgent intervention requiring two or more procedures within the first 7 days (Table 4).
Table 4 Operative pathways and timing in shockedb major traumaa patients undergoing urgent interventionc (patient-level, n = 138)+The median time from hospital arrival to commencement of the index urgent procedure was 150 min (IQR 91–230). Among patients undergoing urgent surgery (n = 109), only 22.0% of procedures commenced during weekday in-hours. The majority occurred out-of-hours (66.1%), and 31.2% occurred on weekends (Table 4).
Operative burden by specialityA total of 518 procedures were performed within the first 7 days among patients undergoing urgent intervention. Orthopaedic surgery accounted for the greatest procedural burden (46.4% of all procedures), followed by plastic surgery (18.2%) and general surgery (14.1%). Procedural intensity varied by specialty, with orthopaedics and burns surgery demonstrating higher mean numbers of procedures per involved patient (Table 5).
Table 5 Operative burden by surgical specialty within the first 7 days among shockedb major traumaa patients undergoing urgent interventionc (procedure-level, n = 518)^Operative timing by specialtyTime to index urgent procedure varied by specialty, with earlier intervention observed for cardiothoracic and neurosurgical procedures and longer times for spinal surgery and interventional radiology cases (Appendix Table A1).
Comments (0)