
Remember me
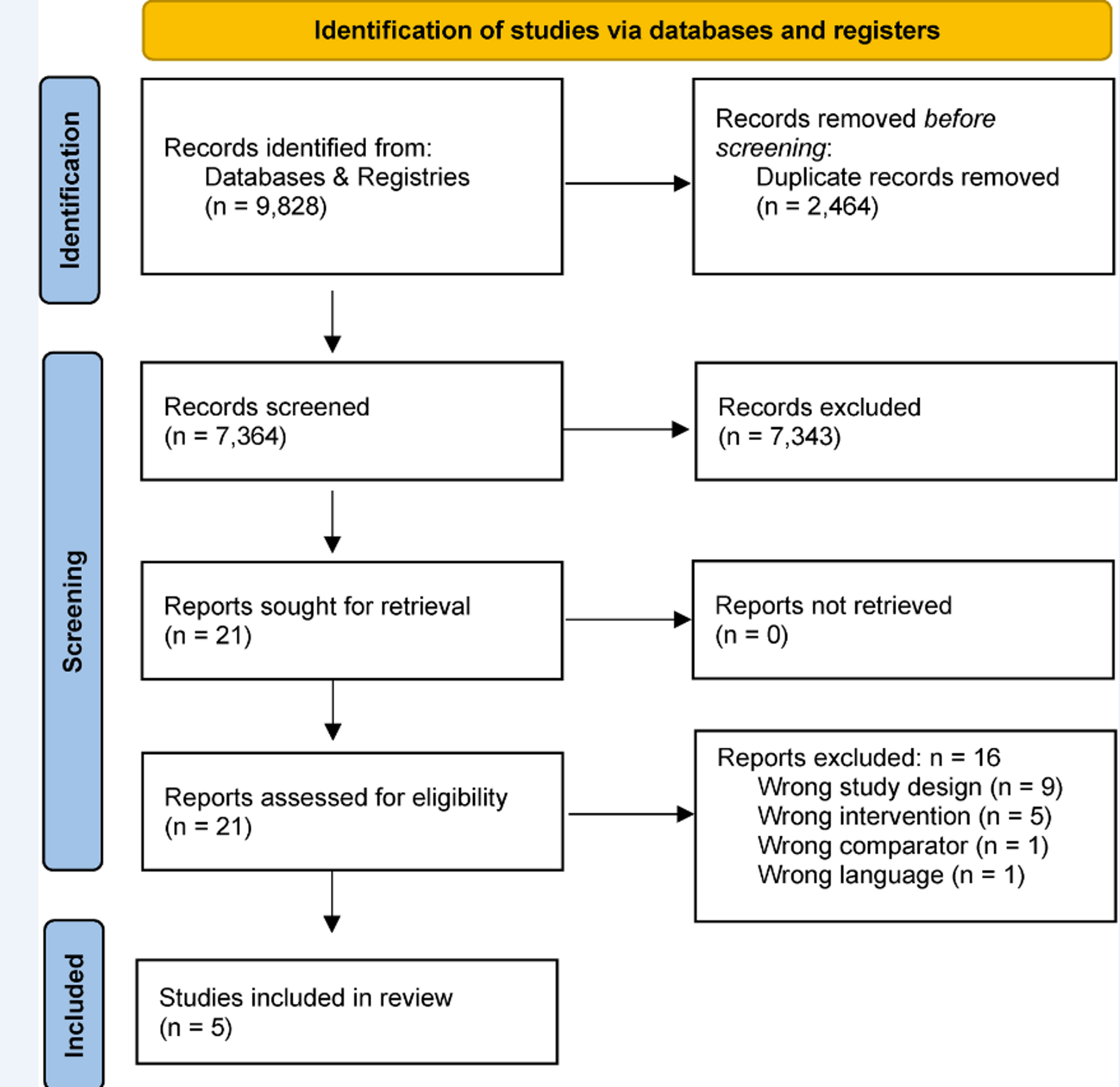
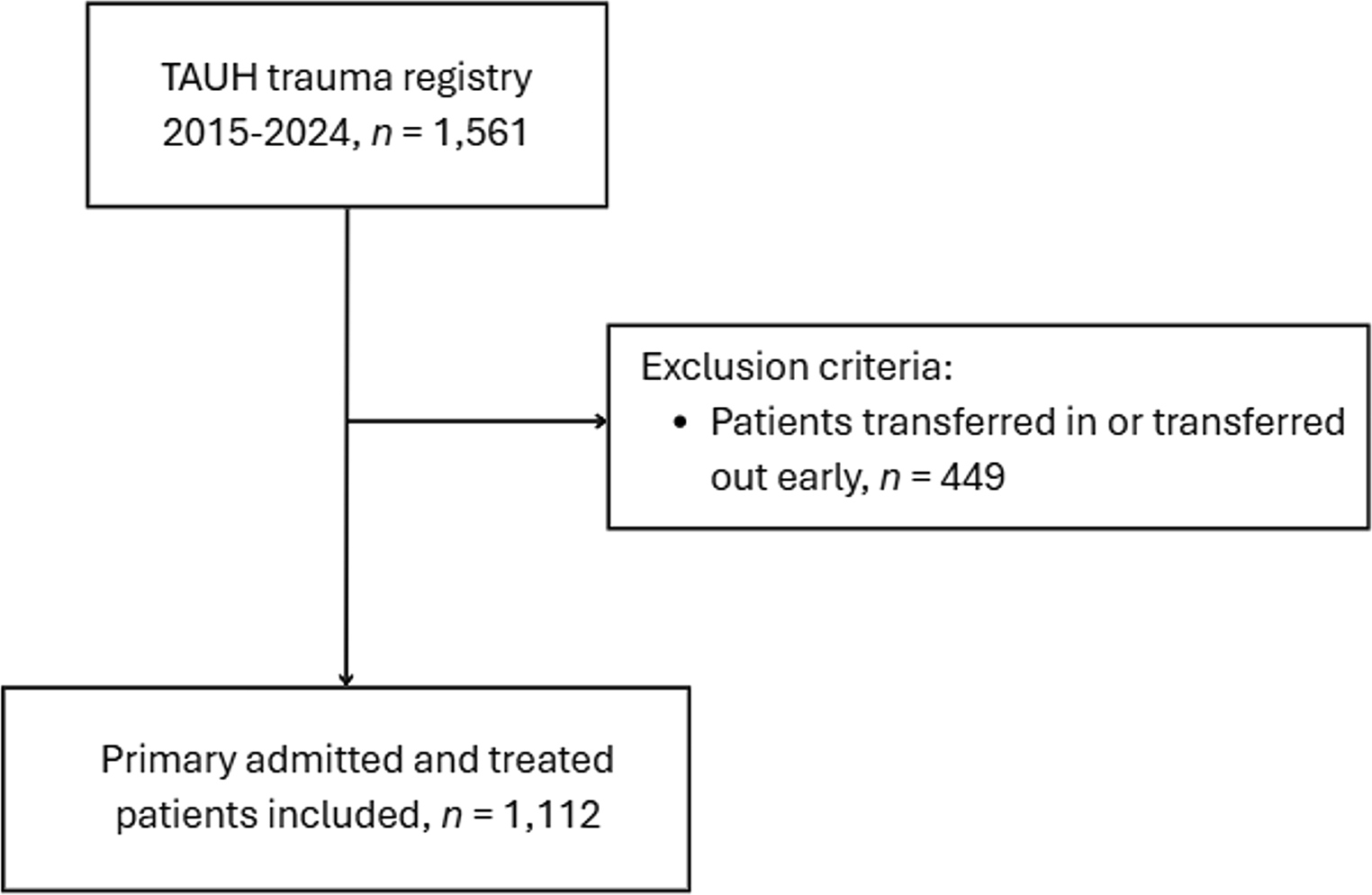
The systematic search identified 1,145 records. After removing duplicates, we screened 1,086 records based on title and abstract; 1,021 studies did not meet the pre-specified inclusion criteria and were therefore excluded. We screened the full texts, trial register entries, and reference lists of the remaining 65 references. Sixty-two records were excluded (Fig. 1). Finally, three RCTs, published between 1976 and 2002, were included in our meta-analysis: Pichler [16], Quinio et al. [17] and Pneumatikos et al. [18].
Within this search, two different concepts of antibiotic prophylaxis in polytrauma patients were identified: selective decontamination and the use of penicillin and ampicillin. The corresponding studies were grouped and analyzed separately.
Fig. 1
Flowchart of the systematic review selection process
Study characteristicsThree RCTs [16, 17, 18] with a total of 256 participants (mean age 37.4 years, 81.6% male) with polytrauma met the criteria for inclusion and were analyzed in our meta-analysis. All included RCTs used a parallel-group design. Two studies compared selective decontamination with placebo [17, 18], whereas one study compared the usage of ampicillin and penicillin to standard of care [16]. The characteristics of the included studies are presented in Table 1.
Table 1 Study characteristicsRisk of bias in studiesThe overall risk of bias among the three RCTs was high for all outcomes due to a lack of a pre-specified analysis plan, no - or no sufficient - information regarding an appropriate analysis method, concealment, or blinding.
Assessment of reporting bias was not possible as there were not enough studies included.
Results of individual studiesAntibiotic prophylaxis compared to placebo or standard care in adult polytrauma patients (Summary of findings Tables 2 and 3).
Table 2 Summary of findings table comparing of Ampicillin & Penicillin vs. standard careTable 3 Summary of findings table comparing of selective decontamination vs. placeboAll-cause mortalityAmpicillin & penicillin vs. standard careOne study reported all-cause mortality for 47 participants (Fig. 2). We found that penicillin and ampicillin contribute little or not to all-cause mortality compared to standard care (RR 1.04, 95% CI 0.57–1.92; risk difference (RD) 18 more per 1000, 95% CI 197 fewer to 422 more; 1 study, 47 participants; very low certainty of evidence). The reason for downgrading was imprecision due to only one study, small number of participants, and a high risk of bias.
Fig. 2
Forest plot describing the difference between antibiotics compared to standard care regarding all-cause mortality
Selective decontamination vs. placeboTwo studies reported all-cause mortality for 209 participants (Fig. 3). We found that selective decontamination makes little or no difference to all-cause mortality compared to placebo (RR 1.01, 95% CI 0.55–1.85; risk difference (RD) 2 more per 1000, 95% CI 79 fewer to 150 more; 2 studies, 209 participants; I2 = 0%; very low certainty of evidence). The reasons for downgrading were a high risk of bias, indirectness due to inconsistent direction of point estimates, and imprecision due to the small number of participants.
Fig. 3
Forest plot describing the difference between selective decontamination compared to placebo regarding all-cause mortality
Clinical status: duration of mechanical ventilationTwo studies reported duration of mechanical ventilation for 209 participants (Fig. 4). We found that selective decontamination makes little or no difference to duration of mechanical ventilation compared to placebo (mean difference (MD) 1.22 days higher, 95% CI 1.41 lower to 384 higher; 2 studies, 209 participants; I2 = 57%; very low certainty of evidence). The reason for downgrading was imprecision due to the small number of participants and a high risk of bias.
Fig. 4
Forest plot describing the difference between selective decontamination compared to placebo regarding duration of mechanical ventilation
ICU length of stayTwo studies reported ICU length of stay for 209 participants (Fig. 5). We found that selective decontamination makes little or no difference to ICU length of stay compared to placebo (MD -3.43 days lower, 95% CI -10.58 lower to 3.73 higher; 2 studies, 209 participants; very low certainty of evidence). The reason for downgrading was imprecision due to the small number of participants and a high risk of bias.
Fig. 5
Forest plot describing the difference between selective decontamination compared to placebo regarding ICU length of stay
Ventilator associated pneumonia (VAP)One study reported VAP for 61 participants (Fig. 6). We found that selective decontamination probably decreases the risk of VAP compared to placebo (RR 0.30, 95% CI 0.13–0.72; risk difference (RD) 373 fewer per 1000, 95% CI 464 fewer to 149 fewer; 1 study, 61 participants; very low certainty of evidence). The reason for downgrading was imprecision due to only one study, the small number of participants, and a high risk of bias.
Fig. 6
Forest plot describing the difference between selective decontamination compared to placebo regarding VAP
We found no data regarding serious adverse events, adverse events, and quality of life.
Comments (0)