
Remember me
This before-and-after retrospective cohort study was conducted at an urban level-2 trauma center and teaching hospital in the Netherlands. At this institution, a VFC review protocol was introduced in April 2020. All Dutch or English speaking ED patients who required follow-up treatment were reviewed according to the VFC review protocol. Exclusion criteria for VFC review were: invalid phone number, Glasgow Coma Scale < 15 at presentation, cognitive impairment, and initial treatment or follow-up elsewhere. Patients who were excluded from the VFC workflow were treated following the pre-VFC workflow protocol.
Ethical approval was obtained by the institutional review board of the hospital (WO.23.073.)
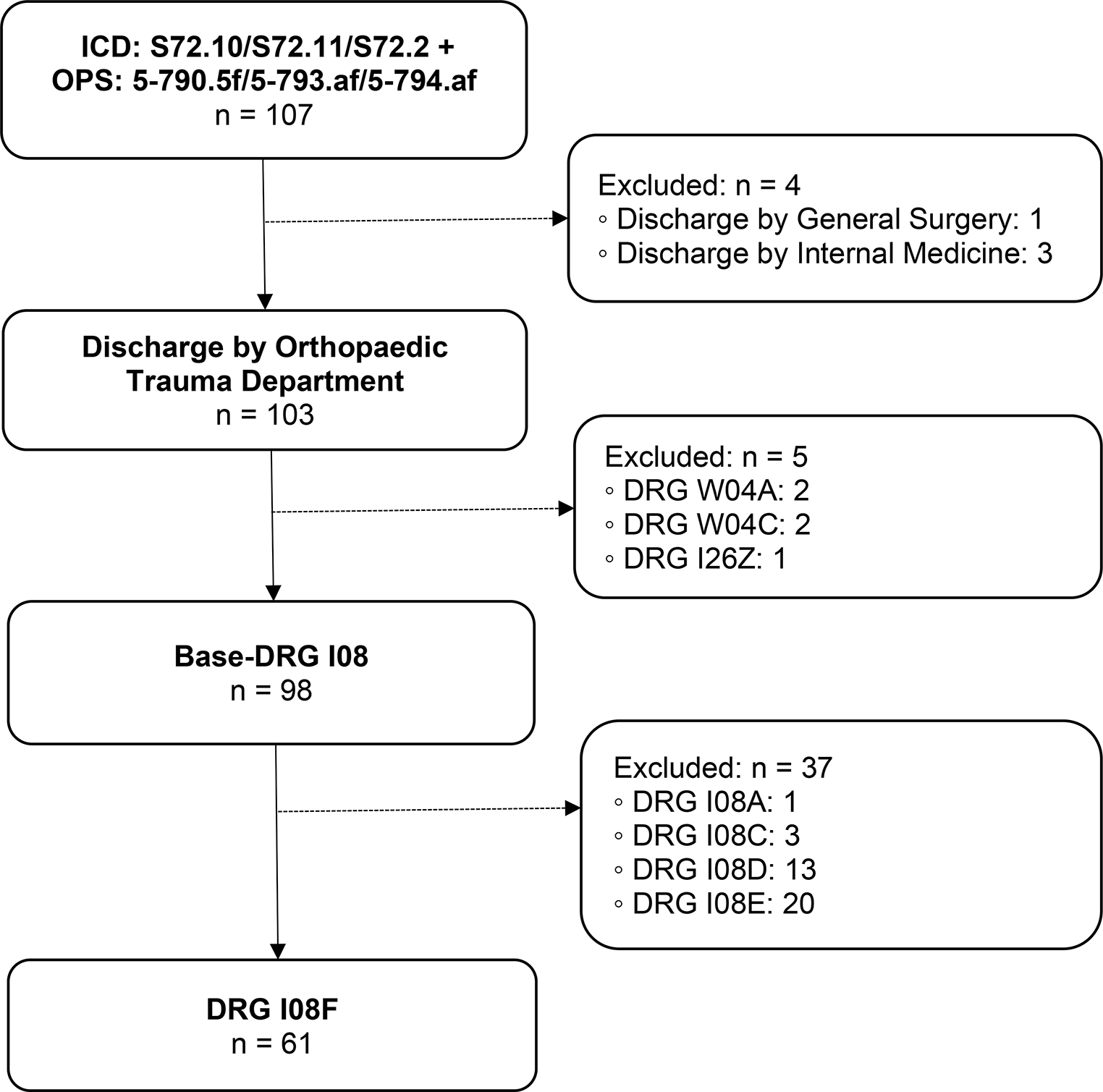
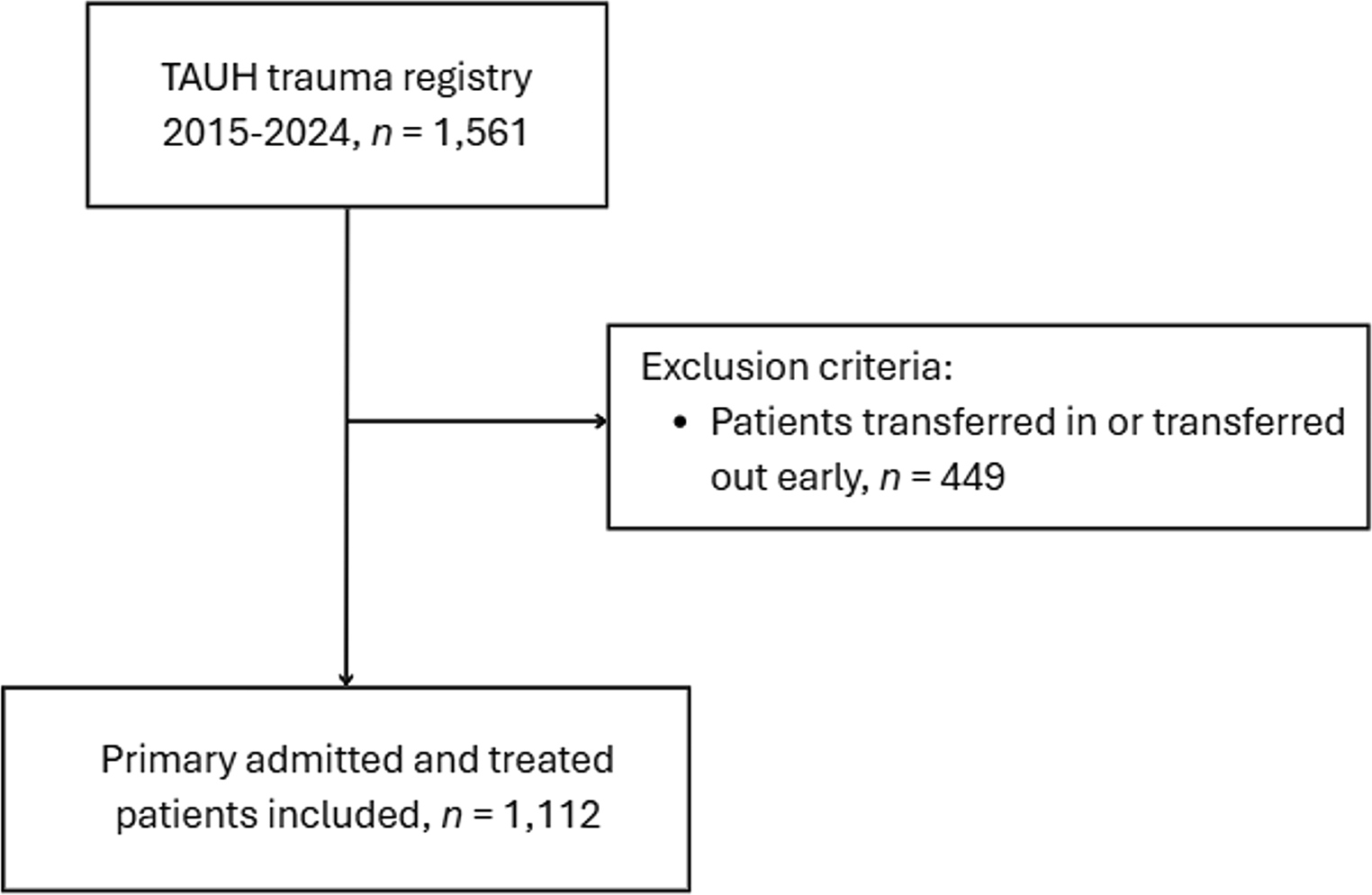
Study populationPatients were included if they were diagnosed with a DRF between April 1 2017 - March 31 2019 (pre-VFC cohort) and April 1 2021– March 31 2023 (VFC cohort), if they received operative treatment with ORIF, and if operative treatment was either directly decided upon or at the first outpatient clinic follow-up visit within one week (e.g., in case of secondary displacement). Patients were excluded if they were operated in an acute setting (i.e. open fractures, nerve or vessel damage), if they were operated over 14 days due to patient delay (i.e. insurance problems, no show), if they received another type of fixation than a dorsal or volar, or dorsal and volar plate (i.e. external fixator, k-wires) (Fig. 1).
Fig. 1 Pre-VFC workflow
Pre-VFC workflowPrior to the implementation of the VFC review, treatment decisions in the ED were predominantly made by residents, with varying degrees of oversight from surgical staff. While radiographs were reviewed by the radiology department, this typically did not occur immediately after imaging. As a result, residents were initially responsible for interpreting the radiographs themselves. Treatment options were either discussed directly with the patient in the ED or deferred to an appointment at the outpatient clinic or casting room shortly after the ED visit. These follow-up appointments were usually handled by residents and a subsequent new follow-up appointment (with additional radiographs) was decided on per visit. To minimize the risk of misdiagnoses (i.e. missed (additional) fractures, underestimations of fracture severity), musculoskeletal ED radiographs from the previous day were reviewed again during a daily radiograph assessment meeting, which included a radiologist, ED staff, and an orthopaedic surgeon. If a misdiagnosis was identified, the patient was scheduled for a follow-up appointment at the outpatient clinic to discuss further treatment. Once surgery was determined as the appropriate course of action, an administrative planner would schedule the procedure and inform the patient within three working days.
VFC review workflowPatients with a trauma-related extremity fracture, who entered the VFC-workflow, received initial treatment at the ED or plaster room without receiving a confirmed diagnosis or a treatment strategy. On the next workday, they were discussed in a multidisciplinary review (attended by an orthopedic surgeon, surgical resident, casting technician, outpatient clinic secretary, operation planning secretary). During this VFC-review, a diagnosis was set followed by a tailor made treatment plan under direct supervision of an experienced orthopedic surgeon. For surgical treatment protocols, the VFC review pathways included information on the surgical procedure, the complete follow-up treatment and the recovery process. The VFC team could adjust treatment protocols for each patient based on expert opinion. Directly after VFC review, patients were informed by phone and consent for definitive treatment was discussed. If there was any hesitancy regarding consent or the choice of treatment, patients were scheduled for an outpatient clinic appointment to discuss treatment options. For patients needing surgery, an administrative planner scheduled the surgical procedure and all follow-up appointments once consent was obtained, and informed the patient the same day through mail or their electronic patient record. Additionally, during the VFC period, patients could also directly visit the plaster room after receiving radiological confirmation of a fracture after referral from a general practitioner. They entered the VFC-workflow.
Data collectionStudy data included age, gender, injured side, weekday of hospital presentation, number and types of hospital contacts (i.e. ED-visit, outpatient clinic visit, telephone consultation), number and type of diagnostic imaging (radiograph, MRI, CTs, ultrasound), number of immobilization materials (casts, braces or ‘other’), initial treatment (operative or non-operative), pathway of initial presentation (ED, outpatient clinic, plaster room), complexity of injury scored by a trauma surgeon pre-operatively (simple or complex) and registered complications. The time to operation was determined by calculating the difference between the date and time of the initial hospital registration and the date and time of the operation. If the injury occurred before the registration date (presentation delay), the difference in dates was added based on the history obtained during the first visit. Additionally, all patients were allotted an extra 12 hours (equivalent to 0.5 days) to account for any potential underreporting of delay between the injury and presentation.
Data analysisThe primary outcome of this study was the exact number of days between the onset of injury and operation. A subgroup analysis was conducted excluding patients who presented through the outpatient clinic and plaster room. The plaster room route was not available in the pre-VFC period, and outpatient clinic patients were not subjected to the VFC workflow.
Additionally, the primary outcome was assessed distinctively for simple versus complex injuries, for female versus male patients, for patients in different age categories; 18–35, 36–65, 66 years and older, and descriptively for weekday of hospital presentation.
The secondary outcome was the quality of planning of semi-acute surgery; within 1–7 days after injury, within 8–14 days after injury, within 15–21 days after injury, and over 21 days after injury.
Exploratory outcomes included the number and types of hospital contacts, diagnostic imaging tests and used immobilization materials. Recorded complications were also reported.
Statistical analysisBaseline characteristics between the pre-VFC and VFC cohorts were compared using independent samples T-tests or Mann-Whitney U-tests for continuous data, based on data distributions. Normality of the data was assessed through visual inspection and the Shapiro-Wilk test. For normally distributed data, the mean and standard deviation were reported, while for non-normally distributed data, the median and interquartile range were provided. Categorical data were analyzed using Chi-square tests, or Fisher’s exact tests when there were zero cell counts.
The difference in days until semi-acute surgery between the pre-VFC cohort and the VFC cohort, considered the primary outcome, was assessed using the log-rank test following Kaplan-Meier survival analysis. The results were plotted as the cumulative probability of having undergone the operation. Since all patients eventually received the operation, the mean days until elective surgery along with its two-sided 95% confidence interval (95% CI) were reported. Consistency of the difference in days between injury and semi-acute surgery across weekdays of presentation was described in the Supplemental material.
Cox regression analyses were conducted to further quantify the impact of VFC implementation by estimating the corresponding mean hazard ratio (HR) for elective surgery following DRF along with its bias-corrected and accelerated 95% non-parametric confidence interval (BCa 95% CI) following bootstrapping, drawing 1000 samples of the same sizes as the original samples with replacement, stratified by VFC-period [25, 26]. Similarly, Cox regression analyses were performed to estimate the HR for semi-acute surgery after substratification by injury severity, gender, and age category respectively. Difference in the secondary outcome quality of timely surgical planning was detected using Chi-square tests or Fisher’s exact tests. A p-value < 0.05 indicated statistical significance for differences in primary and secondary outcomes for DRFs. Exploratory outcomes were documented descriptively.
Comments (0)