
Remember me
All injured adult patients admitted to the trauma intensive care unit (TICU) at Hamad Trauma Center (HTC) were prospectively enrolled for a 12-month period from June 2022 to May 2023 (post-P). HTC is the only adult level 1 trauma center in the state of Qatar. Serving a population of approximately 2.7 million, the center operates with a policy of delivering care at no cost to patients, ensuring equitable access to advanced trauma services.
The new VTEp protocol was implemented as a performance improvement project on June 10, 2022. Enoxaparin dosages in the study group (post-P) were calibrated based on peak plasma anti-Xa levels measured after the administration of the third enoxaparin dose. The outcomes of this group were compared with a historical control of trauma patients (pre-P). The pre-P group was admitted to the TICU over a one-year period directly before the new protocol implementation (June 2021- May 2022). For the pre-P group, the VTEp protocol was fixed dose dalteparin given in a single daily dose. The total number of TICU admissions during these two years was 1064 patients.
The HTC Registry and electronic medical records were reviewed. Additionally, all performance improvement reports auditing VTE cases and suspected bleeding episodes were examined. The HTC registry is regularly validated at the internal and external levels. It reports quarterly to the Trauma Quality Improvement Program–American College of Surgeons (TQIP-ACS).
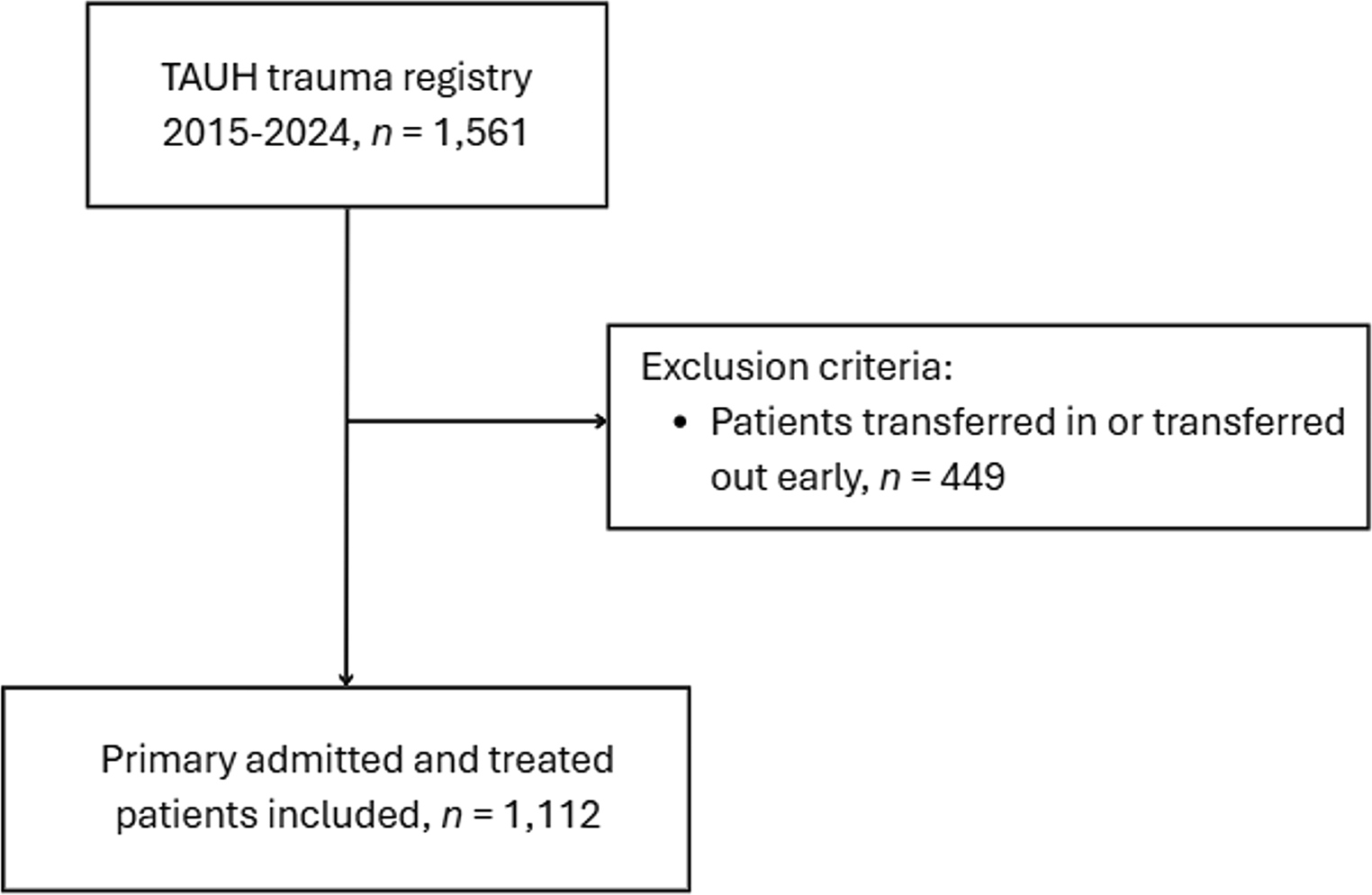
The exclusion criteria were patients who stayed < 72 h at the hospital, pediatric patients, pregnant, renal failure, a known history of malignancy, patients admitted while on anti-coagulation or anti-platelets therapy, presence of a pulmonary artery blood clot within 24 h of admission, and patients transferred from another facility. Figure 1 shows the study design.
All patients had lower limb pneumatic sequential compression devices unless the condition of the lower limbs precluded device application. As for chemoprophylaxis, the pre-P received once daily dalteparin dosing (5000IU and 7500IU for patients with a body mass index (BMI) of 40 or more), which was started at the discretion of the trauma attending. For all patients with TBI, the opinion of the neurosurgeons was considered. There was no anti-Xa monitoring in the pre-P group. The post-P were the patients who complied with the new protocol after its implementation.
Fig. 1
Flow chart for the study design
The new VTEp protocolBetween June 10, 2022, and May 10, 2023, adult patients admitted under the trauma intensive care service were prospectively enrolled into the post-P cohort upon the initiation of enoxaparin prophylaxis. All enrolled patients were administered an initial prophylactic dose of 30 mg enoxaparin subcutaneously twice daily. The dose was weight-adjusted to 0.5 mg/kg in patients with BMI ≥ 30, except in cases of TBI, age above 65, or creatine clearance of 30–60 ml/m. VTEp for non-TBI patients was initiated 24–48 h after admission. In TBI patients, VTEp was started 24–48 h post-admission only if the 24 h follow-up brain CT scan was stable, and no neurosurgical intervention was planned within 12 h. Otherwise, VTEp was held for another 24 h, followed by a repeat CT scan. The neurosurgical team always cleared the initialization of VTEp in TBI patients.
VTEp was withheld in cases of bleeding, suspected bleeding, and suspected or confirmed coagulopathy. Interruptions of VTEp for any invasive procedure or surgery were minimized.
The enoxaparin dose adjustment was based on the peak anti-Xa level measured 3–5 h after the third consecutive dose. The target anti-Xa range was 0.2 to 0.4 IU/ml.
Titration of dosage was based on a predetermined strategy. For peak anti-Xa levels < 0.15 IU/ml, the enoxaparin dose was increased by 10 mg/dose. For peak anti-Xa levels > 0.45 IU/ml, the enoxaparin dose decreased by 10 mg/dose. For anti-Xa levels 0.15–0.19 or 0.41-045, the dose was adjusted by 5 mg. For Anti-Xa level > 0.5, one dose of enoxaparin was held, then restarted with a smaller dose. Anti-Xa level was followed up after adjustments. Enoxaparin continued until the patient was discharged from the hospital (Fig. 2).
Fig. 2
Enoxaparin dose titration per Anti-Xa level
Variables collected included demographic characteristics, BMI, history of chronic illness, previous venous thromboembolism, mechanism of injury, prehospital time, injury severity score (ISS), head abbreviated injury score (AIS), spinal cord injury, unstable spinal fractures, pelvic and long bone fractures, and laboratory parameters on admission. Also recorded the administration of blood products, prothrombin complex concentrate, fibrinogen concentrate, Tranexamic acid, intubation, femoral line insertion., ventilatory days, length of stay in the ICU, time of initiation of enoxaparin, anti-Xa levels, number of dosing interruptions, total hospital stays, and mortality.
Outcome data were the incidence of VTE, PE, DVT, or concomitant PE and DVT, as well as significant bleeding episodes that occurred after initiating VTEp. Diagnosis of DVT was based on duplex ultrasonography, and diagnosis of PE on chest computed tomographic angiography (CTA) of the pulmonary artery upon clinical suspicion; sub-segmental PE was excluded. Proximal Lower limb DVT screening was performed by trauma intensivists using bedside compression ultrasound along with standard Duplex confirmation for any positive or suspicious screening result. Screening bedside compression ultrasound was performed routinely in all TICU patients on the day of admission, then on days 3,7,14, 21, and 28 post admission. Screening was stopped when patients became fully ambulatory, fully anti-coagulated for any reason, or were discharged from the hospital before day 28. Upper limb and distal lower limb DVTs (below the trifurcation of the Popliteal vein) were excluded. Significant bleeding was defined as any bleeding episode requiring blood transfusion, surgical or radiological intervention, Hemoglobin drop of more than 2 gram/dl, new intracranial bleeding or progression of a previous bleed, paraspinal or intraocular bleed. Compliance with timely sampling of the anti-Xa blood level was measured. Anti-Xa levels were studied in relation to the patient’s weight, BMI, creatinine clearance, and Injury severity score (ISS).
The institutional medical review board (Medical Research Center, MRC) (MRC-01-23-872) approved the study protocol at Hamad Medical Corporation, Qatar. A waiver of consent was granted as the data were collected retrospectively and anonymously without direct contact with patients.
Statistical analysisData were expressed as numbers, percentages, and means with standard deviation or medians with range for categorical variables, whenever appropriate. Demographic, clinical, and laboratory parameters and outcomes were compared among the pre-P and post-P groups. Subgroup analysis was also performed among severe TBI patients (AIS 3–5) in the pre-P and post-P groups. The chi-square test was performed to analyze differences in categorical variables between groups, and the Fisher exact test was used when observed cell values were less than 5. Continuous variables were compared using Student’s t-test for two groups for parametric data. The Mann–Whitney U-test was used for non-parametric data whenever applicable.
Furthermore, data were also expressed as odds ratio (OR) and 95% confidence interval (CI). A post hoc power analysis was conducted to determine the study’s statistical power. Two-tailed p < 0.05 was considered as statistically significant. Data analysis was conducted using the Statistical Package for Social Sciences version 21 (SPSS Inc., Chicago, IL).
The Shewhart T-chart was utilized to monitor the time intervals between consecutive PE events and to assess trends before and after implementing the new protocol. The T-chart, designed for rare events, plots the time intervals (Y-axis) against the dates of events (X-axis). Trend is statistically significant when more than six consecutive data points fall on the same side of the centerline, two out of three successive points on the same side of the centerline are farther than two σ, or a single point farther than the upper control limit [10].
Comments (0)