
Remember me
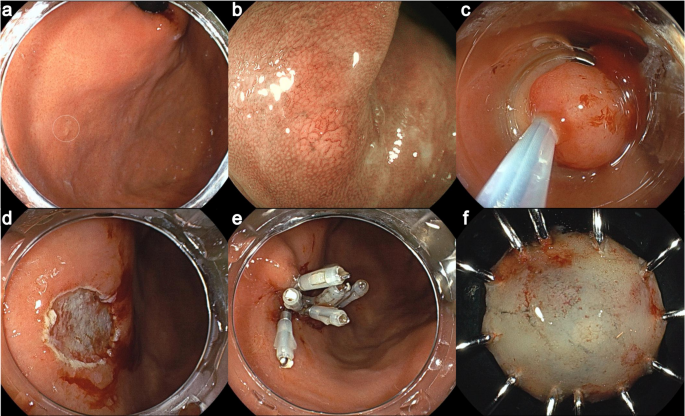
A 69-year-old man with a 3-year history of continuous PPI use (esomeprazole 20 mg daily) for Barrett’s esophagus. The patient underwent a follow-up upper endoscopy, which revealed a small whitish flat lesion on the non-atrophic fundic gland mucosa (lesion A) (Fig. 1a–c). Two years later, the lesion was markedly enlarged, and narrow-band imaging with magnifying endoscopy showed an irregular superficial microstructure that was clearly demarcated from the adjacent mucosa (Fig. 1d–f). A biopsy specimen showed histological evidence of low-grade foveolar-type gastric dysplasia.
Fig. 1
Changes in endoscopic findings over time (lesion A). A small flat whitish lesion was observed in the non-atrophic fundic gland mucosa (arrow) (a, b). Narrow band imaging with magnification endoscopy shows an irregularly shaped tubular structure (c). Two years later, the lesion was significantly enlarged (arrows, d). The lesion showed a course, flatly elevated shape (e) with a papillary-dominant superficial microstructure clearly demarcated from the adjacent mucosa (arrowheads, f), suggesting an epithelial neoplasm
The patient had never received Hp eradication therapy. His serum anti-Hp IgG antibody titer was < 3 U/mL, and a 13C-labeled urea breath test value was < 2.5‰, findings consistent with Hp-naïve status. The serum gastrin level was 1960 pg/mL, indicating hypergastrinemia due to continuous PPI use. As the endoscopic features of the lesion were similar to flat-type FGA, a colonoscopy was performed to rule out a syndromic FGA, but only a few colonic adenomas were found. There was no family history of familial adenomatous polyposis or gastric adenocarcinoma with proximal polyposis of the stomach. The tumor was therefore considered to be a sporadic tumor arising from Hp-naïve gastric mucosa. It was completely resected by endoscopic submucosal dissection.
The resected specimen showed a 67 × 48 mm lesion with a small satellite lesion (Fig. 2a). The lesion consisted mainly of atypical tall columnar cells resembling gastric-foveolar cells with tubular-dominant and superficial papillary structures (Fig. 2b). The nuclei, round to oval and slightly elongated in shape, were basically located (Fig. 2c). In the deep and peripheral areas of the lesion, there was a clear border with the normal gastric fundic gland mucosa epithelium (Fig. 2d–e). Consequently, the lesion was diagnosed as a low-grade FGA according to the WHO classification [3, 12].
Fig. 2
Resected specimen and histologic findings (lesion A). The resected lesion measured 67 × 48 mm (yellow arrow), with a small satellite lesion (blue arrow) (a). The lesion consisted mainly of atypical tall columnar cells resembling gastric-foveolar cells with tubular-dominant and superficial papillary structures (b). The nuclei, round to oval and slightly elongated in shape, were basically located (c). The fundic gland tissue was preserved under the neoplastic glands (d). In the periphery, the neoplastic epithelium showed thin, superficially spreading growth with a boundary distinct from the adjacent foveolar epithelium (arrow), suggesting a low-grade FGA. The fundic gland tissue showed parietal cell enlargement with protrusion into the lumen of the gland, suggesting a PPI-associated gastropathy (e)
Immunohistochemical analysis showed strong diffuse MUC5AC expression in neoplastic cells (Fig. 3a), partial MUC6 expression in the lower neoplasm layer (Fig. 3b), and sporadic MUC2 expression in the neoplastic epithelium (Fig. 3c), with no intestinal metaplasia in the surrounding epithelium. Other intestinal markers (CD10 and CDX2) were negative, supporting foveolar cell-dominant differentiation. Ki-67 and p53 were diffusely expressed in the lower to middle layers of the neoplasm, with reduced expression in the superficial layer (Fig. 3d, e). β-catenin was expressed in the cell membranes and cytoplasm, whereas its nuclear translocation was not confirmed (Fig. 3f). These findings were consistent with those of gastric foveolar-type dysplasia and adenoma.
Fig. 3
Immunohistochemical analysis (lesion A). MUC5AC was strongly, diffusely, expressed in the neoplastic cells (a), MUC6 was partly expressed in the lower layer of the neoplasm (b), and MUC2 was sporadically expressed in the neoplasm (c), exhibiting a gastric-dominant immunophenotype (foveolar cell differentiation). Ki-67 (d) and p53 (e) were diffusely expressed in the lower to middle layers of the neoplasm, and the expression was reduced in the superficial layer. β-catenin was expressed in the cell membranes and cytoplasm, but its nuclear translocation is not seen (f)
The patient was continuously treated with a PPI after endoscopic treatment. Two months later, a follow-up endoscopy revealed a new flat whitish lesion (lesion B) with indistinct contours near the initially resected lesion (Fig. 4a). Two more years later, lesion B was clearly demarcated from the surrounding mucosa (Fig. 4b), and two new lesions were detected in the lesser curvature of the gastric body (lesions C and D, Fig. 4c). Narrow-band imaging with magnification endoscopy showed an irregular superficial microstructure, suggesting neoplastic characteristics (Fig. 4d–f). Biopsy specimens from each lesion showed histologic evidence of low-grade foveolar-type gastric dysplasia.
Fig. 4
Changes in the endoscopic findings over time (lesions B, C, and D). Two months after the endoscopic resection of lesion A, an opaque flat lesion was newly identified near the scar of the resected specimen (lesion B, white arrows, a). Two years later, lesion B had thickened and was more clearly visualized (white arrows, b), and two more lesions had appeared de novo at the lesser curvature of the gastric body (lesion C, blue arrows; lesion D, red arrows, c). Narrow-band imaging with magnification endoscopy of each lesion showed irregularly shaped, papillary-dominant superficial microstructures (d, lesion B; e, lesion C; f, lesion D), suggesting multiple metachronous recurrences
All three lesions were resected endoscopically. Histologically, they were all diagnosed as low-grade FGAs, which were consistent with the findings of the first resected lesion. Lesion B was 97 × 76 mm (Fig. 5), lesion C was 26 × 23 mm (Supplementary Figs. 1a-1d), and lesion D was 50 × 15 mm (Supplementary Fig. S1e–h). The lamina propria mucosae is thickened due to hyperplastic changes in parietal cells, characterized by cellular enlargement and protrusion into the dilated glandular lumen, consistent with PPI-associated gastropathy. The whole-exome sequencing was performed on lesion B with the approval of the hospital’s ethics committee and the patient's informed consent, comparing neoplastic and normal mucosa using the NovaSeq system. Variants with a variant allele frequency (VAF) greater than 10% were classified as mutations. A KRAS mutation (p.G13C) and a CTNNB1 mutation (p.Leu366Phe) were identified, with VAFs of 43.5% and 10.1%, respectively. No mutations were identified in the APC or TP53 genes.
Fig. 5
Resected specimen and histologic findings (lesion B). The resected lesion measured 97 × 76 mm and was completely resected (a). Neoplastic tissue was seen growing over the non-atrophic fundic glands that show cystic dilation (b), and the findings were diagnosed as a low-grade FGA (c). The lesion exhibits lateral spreading growth of neoplastic glands in a superficial layer across the lamina propria mucosae, which is thickened by hyperplastic changes in parietal cells (d), characterized by cellular enlargement and protrusion into the dilated glandular lumen (e), consistent with PPI-associated gastropathy. In the periphery, the neoplastic epithelium showed thin, superficially spreading growth with a boundary distinct from adjacent foveolar epithelium (arrow, f). MUC5AC was diffusely expressed in the neoplastic cells (g), and MUC6 was partly expressed in the lower layer of the neoplasm (h), as seen in lesion A
After endoscopic resection, PPI treatment was adjusted to on-demand use to reduce the potential risk of tumorigenesis due to chronic PPI use. Serum gastrin levels normalized, and periodic follow-up endoscopy showed improvement in wall thickening and fold meandering, while histological findings remained largely unchanged (Supplementary Fig. S2). The patient has been undergoing regular follow-up endoscopy, with no evidence of metachronous recurrence observed over the past 4 years.
Comments (0)