
Remember me
Crowding in the lower anterior often causes plaque and calculus deposition, leading to periodontitis, particularly in untreated adult patients.[1] Anterior crowding is the most common malocclusion in adult patients, with higher plaque retention and increased difficulty in cleaning interdental areas.[2] Thin gingival biotype (GB) or gingival recession (GR) in the lower anterior region is commonly associated with dental crowding. Orthodontic treatment in such cases poses significant clinical challenges, highlighting the importance of proper preventive measures to ensure successful orthodontic therapy.[3] Periodontal pocket formation, gingival recession, and alveolar bone dehiscence are common concerns in adults before or during orthodontic treatment.[4]
GB refers to a soft-tissue measurement of the thickness and width of the gingiva, while bone morphotype pertains to the thickness of the buccal alveolar bone, and together, these are referred to as the periodontal biotype (PB).[5] It is crucial to examine PB to understand the underlying alveolar bone crest and thickness over the root surface before the initiation of orthodontic treatment.[5,6] Conditions with a thin PB are more prone to develop GR during orthodontic treatment.[7]
Measuring alveolar bone thickness (ABT) along with GB is crucial for predicting the condition of periodontal tissue and the potential development of GR. Crowded teeth with a space deficiency >3.5 mm can increase the risk of developing periodontal diseases.[8]
The most common complication with thin buccal bone plates is the development of GR, alveolar bone dehiscence, and fenestration problems.[9] A study by Huynh-Ba et al.[10] stated that the critical buccal bone thickness should be at least 2 mm to secure favorable functional and esthetic outcomes.
Cone-beam computed tomography (CBCT), a specialized dental imaging method, is influenced by the field of view (FOV) and voxel size. It provides detailed cross-sectional images across anatomical planes, offering precise anatomical relationships.[11]
The use of CBCT in dental specialties has gained significant popularity due to various advantages, such as reduced radiation exposure, cost-effectiveness, and the ability to visualize three-dimensional images of the alveolar bone.[12] CBCT enables clinicians to evaluate teeth and alveolar bone morphology, as well as alveoloskeletal discrepancies, with high accuracy before initiating tooth movement.[13]
Clinical evaluation of facial bone is an invasive procedure that requires flap elevation or sounding under local anesthesia. Hence, alternative advanced imaging techniques such as three-dimensional CBCT have been used to study facial bone thickness.[14-16]
With a lack of studies in the field of buccal bone thickness, especially in the lower anterior teeth with crowding, the present study was conducted to evaluate PBs and GR in malpositioned mandibular anterior teeth.
MATERIAL AND METHODSIn the present study, subjects of both genders with anterior mandibular crowding were examined. Dental models were used to measure the degree of crowding, and the sum of the linear displacements of anatomical contact points of six mandibular anterior teeth was calculated in millimeters (mm).[17] Subjects with a crowding score of ≥4 mm were included in the study. After explaining the study in detail, written informed consent was obtained from those who were willing to participate. The study received approval from the Institutional Ethical Committee (Pr.232/IEC/SIBAR/2020).
Sample size calculation was done using G power 3.1.9.2 software version* (Heinrich Heine University Düsseldorf, Germany) with an effect size of 0.25, alpha error of 5%, and power of 95%. A total sample size of 30 subjects with mandibular crowding was considered for this study.
Inclusion criteria were as follows: (1) subjects who were systemically healthy and (2) aged between 20 and 30 years with moderate to severe malposition lower anterior teeth. Exclusion criteria were as follows: (1) subjects with a history of previous orthodontic treatment, parafunctional habits, attrition in the lower anterior teeth, crowns or extensive restorations in the lower anterior teeth, pregnant or lactating women, individuals under medications that could affect gingival thickness (GT), and those with tobacco use habits.
Most buccal malposition mandibular anterior tooth was considered to assess the PB. Parameters such as GT and GR are measured clinically, whereas crown form (CF) and buccal ABT were measured using CBCT† (Carestream CS9300, Carestream dental, USA) 90 kV, resolution of 200 microns with a FOV of 5 × 5 cm for mandibular anterior sextant.
GR was measured from the cementoenamel junction to the most apical extension of the free gingival margin using UNC-15¶ (Hu-Friedy Mfg. Co., LLC, Chicago, IL, USA) graduated periodontal probe. The measurement value of 0.5 mm was rounded to the nearest mm.
GT was measured at 1.5 mm apical to the free gingival margin on the facial side of most buccally placed lower anterior teeth. A 10-mm endodontic spreader Mani. Inc., Tochigi, Japan with a 3-mm silicone disc was inserted perpendicularly into the gingiva until the hardness was felt. A digital caliper ‡ (VTECH, carbon fiber composites, India) (0-150 mm digital calliper) with 0.1 mm sensitivity is used to measure the distance from the tip to the inside of the disc. The obtained value of <1 mm is considered a thin biotype, and >1 mm is a thick biotype.[18]
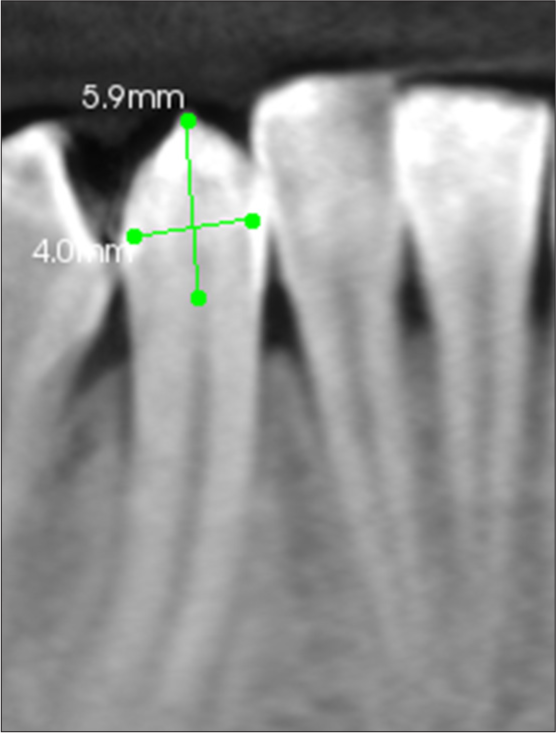
CF was measured as the ratio between crown length (CL) and crown width (CW) at the cervical and middle portions of the crown. These reference points were identified using CBCT in the coronal plane, with slicing cuts set at 0.25 mm intervals for accuracy. CL is measured in the middle of the crown extending from the incisal edge to cemento enamel junction (CEJ), and CW is measured from the mesiodistal distance at the level of one-third of the CL [Figure 1].[18] Short and wide crowns have a crown ratio close to 1, while long and narrow crowns have a lower crown ratio.
Export to PPT
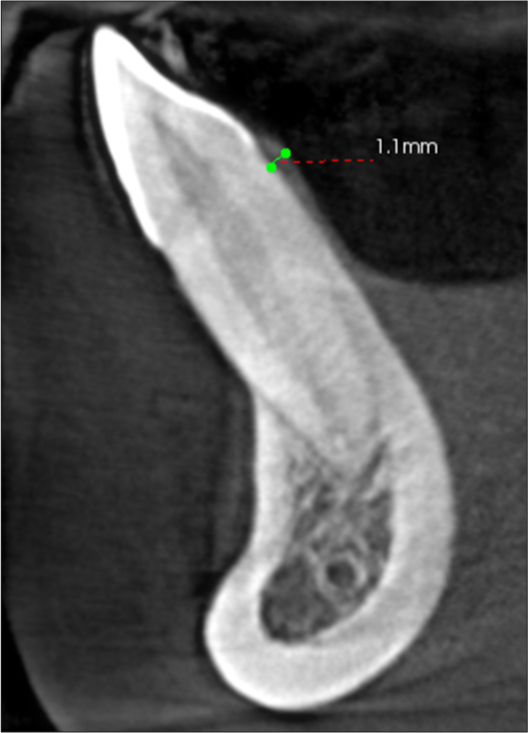
ABT was measured on the labial surface, perpendicularly from the outer wall to the inner wall, at 2 mm apical to the bone crest. These measurements were obtained using CBCT in the sagittal plane, with slicing cuts set at 0.25 mm intervals for precise evaluation [Figure 2].[19]
Export to PPT
The same examiner took all the measurements to ensure consistency in results (kg). Intra-examiner reliability was assessed by taking three measurements on each subject in a single session. The consistency between these repeated measurements was analyzed using the intraclass correlation coefficient to determine reliability. All the subjects received oral prophylaxis, and oral hygiene instructions were given.
RESULTSA total of 75 malposition teeth were evaluated in 32 subjects with a mean age of 23.5 ± 5.5 years. Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 20 software‡‡ (SPSS version 20 software, Chicago, IL, USA). Spearman’s correlation coefficient (k) was used to assess the affiliation between GT, CF, ABT, and GR. P < 0.05 was considered to be statistically significant. The mean descriptive statistical values of GT (1.01 ± 0.53), CF (0.85 ± 0.32), ABT (0.4 ± 0.3), and GR (1.6 ± 1.6) with maximum and minimum values are shown in [Table 1]. The correlation between the GT, CF, ABT, and GR is shown in [Table 2].
Table 1: Descriptive statistics
Parameter Mean (mm) Standard deviation (mm) Minimum (mm) Maximum (mm) Range (mm) GT 1.017333 0.535086 0.3 2 1.7 CF 0.857333 0.328869 0.2 1.5 1.3 ABT 0.409333 0.369138 0 1.2 1.2 GR 1.626 1.625 0 5 5Table 2: Correlation between GT, CF, ABT, and GR
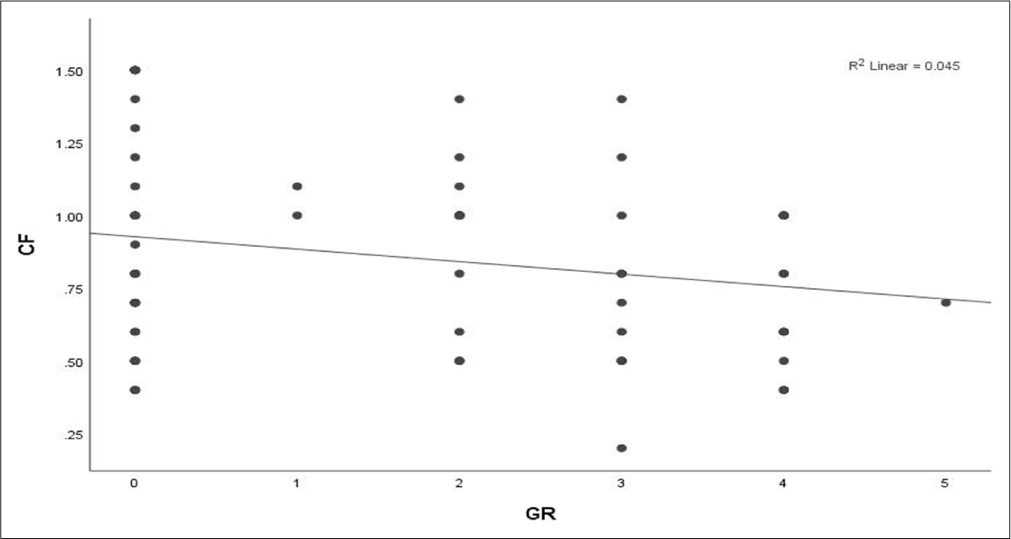
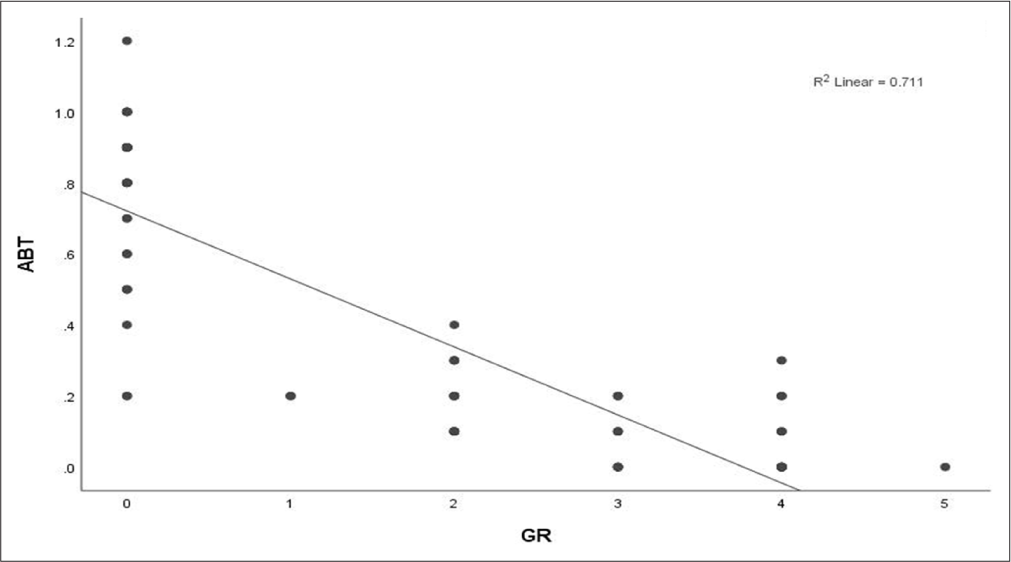
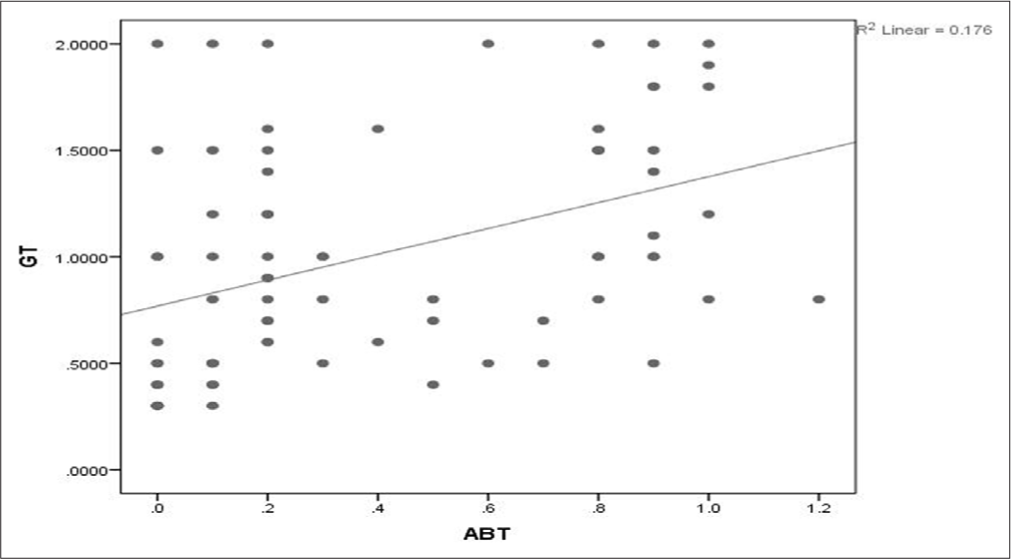
GT CF ABT GR GT Correlation Coefficient 0.124 0.467** −0.374** Sig. (2-tailed) 0.289 0.000 0.001 CF Correlation Coefficient 0.124 0.138 −0.169 Sig. (two-tailed) 0.289 0.237 0.146 ABT Correlation Coefficient 0.467** 0.138 −0.861** Sig. (two-tailed) 0.000 0.237 0.000 GR Correlation Coefficient −0.374** −0.169 −0.861** Sig. (two-tailed) 0.001 0.146 0.000The associations between GT, CF, and ABT with or without GR are shown in [Table 3]. The GT and GR showed statistical significance (P = 0.005) with a mean and standard deviation (SD) of 0.86 ± 0.5 in sites with GR and 1.20 ± 0.52 in sites without GR [Figure 3]. GR and CF show a weak negative correlation with a correlation coefficient of -0.215, indicating that as Gingival Recession (GR) increases, the CF slightly decreases. However, the correlation is very weak, as seen from the low R2 value (0.046) [Figure 4]. The ABT showed a statistical significance (P = 0.001) with GR with a mean and SD of 0.12 ± 0.1 in GR sites and 0.77 ± 0.22 in the sites without GR [Figure 5]. GT and ABT show a moderate positive correlation with a correlation coefficient of 0.467 with a statistical significance of P = 0.000 [Figure 6]. GT and GR’s correlation is statistically significant (P = 0.001) with a correlation coefficient of −0.374, which shows a weak negative correlation. The ABT and GR show a robust negative correlation with a correlation coefficient of −0.86 with a statistical significance of P = 0.00, which shows that ABT exhibits with GR.
Table 3: Difference in GT, CF, and ABT scores with GR
Parameter GR P-value Yes No GT (mean±SD) 0.869048±0.5 1.206061±0.52 0.005* CF (mean±SD) 0.816667±0.28 0.909091±0.37 0.22 ABT (mean±SD) 0.121429±0.1 0.775758±0.22 0.001*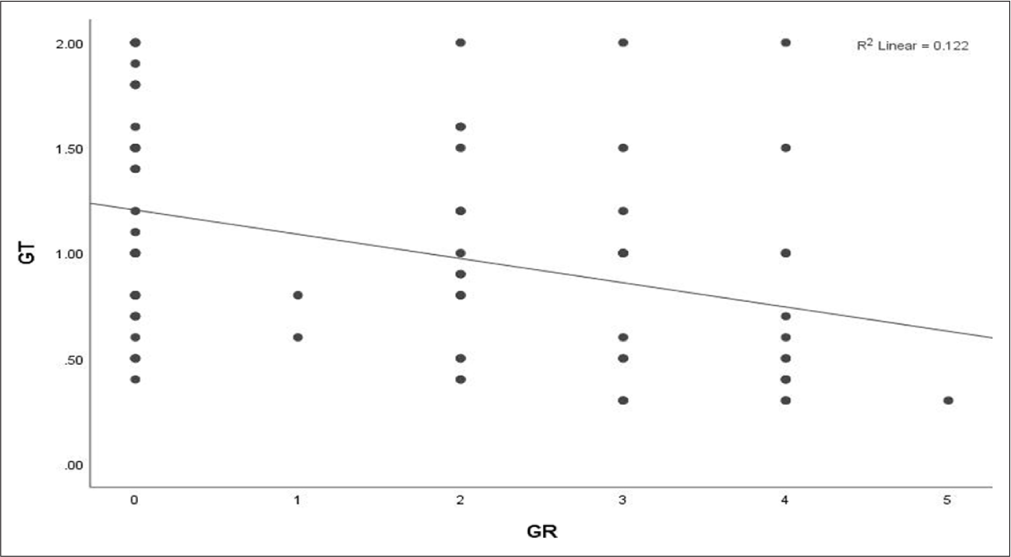
Export to PPT
Export to PPT
Export to PPT
Export to PPT
DISCUSSIONPB is mostly associated with the underlying alveolar bone morphology, GT, and CF. The severity of periodontal conditions depends on different PBs.[20] Identification of GT is vital for estimating osseous architecture clinically, as differences in gingival and osseous morphology significantly impact disease progression and treatment outcomes.[21,22] GT on the buccal or facial aspects can be measured using both invasive and non-invasive methods, including injection needles, trans gingival probing, histologic sections, ultrasonic devices, cephalometric radiographs, and CBCT. Among the non-invasive methods, ultrasonic devices and CBCT have gained importance due to their high consistency in producing reliable and reproducible results. These methods offer accurate measurements for clinical applications, particularly in assessing gingival and bone thickness.[23,24]
In this study, GT was determined using a simple and non-subjective method with an endodontic reamer under local spray anesthesia. Muller et al.[22] measured the GT using an ultrasonic device and stated that GT is strongly associated with the gingival width and tooth type. Periodontal health is mostly associated with a thick GB because thin GBs are less stable, often resulting in papillary and marginal recession.[25] Januario et al. stated that decreased GT is a significant factor that can lead to periodontal attachment loss and marginal tissue recession.[26] Another study by Zawawi and AlZahrani[27] reported no association between crowding and GT in the anterior maxillary teeth.
In the present study, the lower anterior, particularly canines and lateral incisors, exhibited a thin GB compared to central incisors. This observation is consistent with previous studies, which suggest that GT varies with the location of the teeth in the dental arch.[16,24]
Olsson and Lindhe[28] were the first to examine the relationship between CF (CW/CL) and the morphological characteristics of the gingiva. Later, Eger et al.[29] and Fischer et al.[30] have observed a relationship between CF and GT and found no significant association between them, Stein et al.[31] compared clinical measurements CL and CW with GT and ABT using parallel profile radiographs. They found that CF is a significant predictor for GT and ABT. Januario et al.[32] measured tissue dimensions clinically and radiographically using CBCT in maxillary central incisor teeth and found that CL and CW are determinants of GT and ABT factors.
Measurement of hard tissue thickness by CBCT was considered a superior method in comparison with other direct measurement techniques.[31] In the present study, CBCT was utilized to measure ABT and CF due to its accuracy in measuring hard-tissue thickness. The results of this study show that the square-shaped CF was associated with both thick and thin GT; there was no consistent relationship between GT and CF. The results of this study are in accordance with a previous study by Olsson et al., which reported that larger and more apically located contact points in square-shaped teeth tend to be associated with a thick GB.[33] GT and ABT are considered significant risk factors for GR in mandibular anterior teeth with varying levels of malocclusion and crowding. Cook et al.[34] observed a strong association between PB with labial bone thickness in maxillary anteriors measuring with CBCT.
A moderate association was observed in a study conducted by Fu et al., where they compared the thickness of soft and hard tissues in traumatically extracted anterior maxillary teeth from cadaver heads, both clinically and radiographically, using CBCT.[14]
Both the above studies found that facial GT and ABT had a moderate association with CBCT measurements and were accurate compared to clinical values. This is the first study carried out to evaluate the relationship between GT and ABT with GR in mandibular anterior teeth with crowding using CBCT. The results of the present study showed a weak association between GT and ABT. This observation was likely due to the fact that crowded teeth were usually positioned more buccally or lingually, leading to variations in ABT, whether thin or thick.
Although bacterial plaque is considered the main etiological factor for periodontal disease, other factors, such as malpositioned teeth, can also lead to pathological changes in the periodontium.[28] Lee et al.[35] stated that a thin GB often indicates a deficiency or absence of buccal bone, which can result in GRs. Silva et al.[36] observed an association between GR and ABT in anterior maxillary teeth using CBCT. They found that thin or absent buccal bone was associated with GR. Understanding the relationship between GR and ABT is crucial for procedures such as implant placement, periodontal esthetic surgeries, and orthodontic treatments, as it helps predict treatment outcomes and prevent complications such as GR and bone loss.[37]
Previous research focused on maxillary anterior teeth, highlighting that GR was commonly associated with thin ABT and thin PB. In this study, results indicated that buccally placed mandibular anterior teeth exhibited a thin PB with both thin GT and ABT. GR was observed irrespective of whether the PB was thin or thick. This suggests a weak association between GR and both GT and ABT in mandibular anterior teeth. Thus, GR can occur in both thin and thick PBs, indicating that factors other than just GT and ABT might also influence the presence of GR.
The present study results indicate significant differences in gingival and alveolar bone dimensions between patients with thin and thick PBs. It is also observed that GR tends to increase with the severity of malocclusion.
The limitations of the present study include:
The absence of an assessment of crowding severity caused by malpositioned teeth.
The study focused solely on buccally erupted anterior teeth, disregarding the potential influence of lingually positioned teeth on buccal bone thickness.
Minor occlusal discrepancies and skeletal variations were not taken into account, which may have influenced the findings.
Future studies incorporating these factors could offer a more comprehensive understanding of the relationship between periodontal biotype, alveolar bone thickness, and gingival recession.
CONCLUSIONCrowding can significantly impact PB parameters. The present study found that gingival and alveolar bone dimensions differed notably between patients with thin and thick PBs. Although GR tends to increase with the severity of malocclusion, understanding the underlying alveolar bone morphology is crucial for accurate diagnosis. This knowledge is essential to prevent adverse outcomes in future periodontal and orthodontic treatments, particularly in cases involving malpositioned mandibular anterior teeth.
Comments (0)