
Remember me

In this randomized, open-label exploratory study, participants were assigned in a 1:1 ratio to one of two groups: daily biofeedback therapy (BF) alone or a combined daily intervention of biofeedback therapy with cognitive training (BF + COG). Eye movement data were obtained both before and after the 6-week intervention period (refer to Fig. 1).
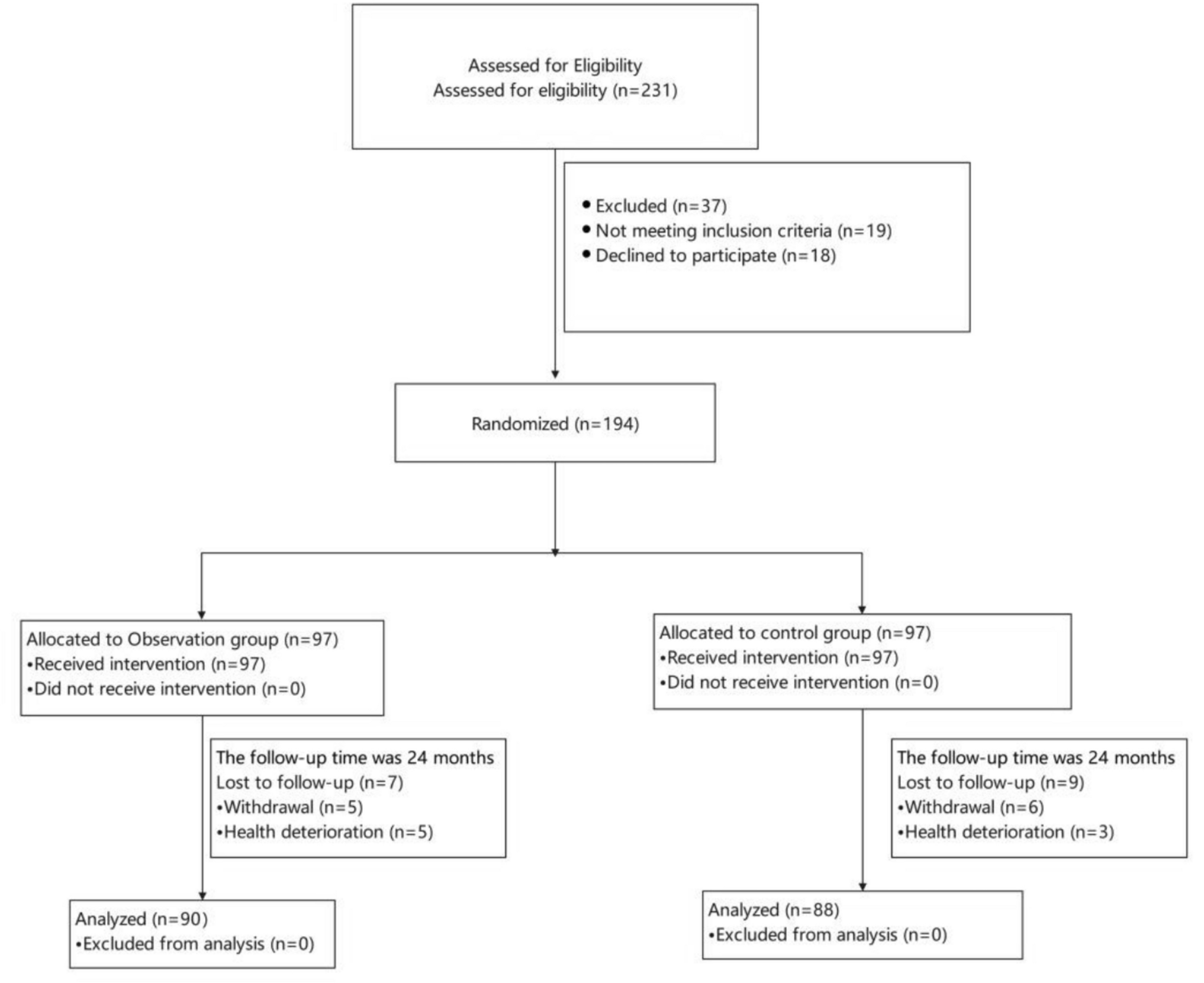
Fig. 1 Participants
ParticipantsThe eligibility criteria for participants were as follows: (1) female breast cancer patients aged 18–70 years, (2) a confirmed diagnosis of invasive carcinoma through pathology, (3) a history of breast-conserving surgery with the need for adjuvant radiation therapy, (4) completion of at least 4–6 cycles of standard neoadjuvant and/or adjuvant chemotherapy that included paclitaxel and/or anthracyclines, and (5) subjective complaints of cognitive impairment. Participants were excluded if they (1) had previous or concurrent malignant tumors, (2) had undergone prior breast or chest radiation treatment, (3) had been diagnosed with bipolar disorder, schizophrenia, or other mental disorders, (4) were illiterate, colorblind, or severely impaired in listening, speaking, reading, or writing, and (5) could not guarantee attendance at the intervention and follow-up sessions.
Assuming a 5% probability of unforeseen problem occurrence in pilot study, priori research recommended a sample size of 59 to reliably detect such problem [23]. However, the final sample size was impacted by the COVID-19 lockdowns in Shanghai, as they overlapped with both the recruitment and intervention phases, making it difficult for many eligible participants to reach the cancer center. Consequently, despite extending data collection beyond the planned timeline, only 52 eligible participants were recruited, and after the follow-up period, only 36 remained in the study.
ProcedureAll procedures were approved by the Institutional Review Board of Fudan University Shanghai Cancer Center (SCCIRB), and written informed consent was obtained from all participants.
From December 2021 to December 2022, participants were recruited from the Department of Radiotherapy and screened for eligibility by a project coordinator from the Medical Psychology Department. Eligible participants were randomly assigned via IVRS/IWRS to either the BF or BF + COG group before undergoing baseline eye-tracking assessments. All participants received 30 intervention sessions (five weekly sessions over 6 weeks) synchronized with radiotherapy. The BF group performed daily 20-min biofeedback therapy targeting physiological regulation through abdominal breathing and progressive muscle relaxation. The BF + COG group additionally completed adaptive cognitive training (20–25 min per session) using the tablet-based ACE software, as described in the cognitive training protocol. Follow-up eye movement data was collected on the final day of the intervention.
Biofeedback therapyBiofeedback therapy utilized real-time physiological signal monitoring to train participants in self-regulation of stress responses [24]. Sessions were conducted in a sound-attenuated treatment room with dim lighting, where participants reclined in semi-supine positions. Therapists positioned a wireless biosensor headband (Vishee Inc., Freemind-S) equipped with forehead electrodes and earlobe clips to record electromyography (EMG), electroencephalography (EEG), and heart rate. The collected signals were transmitted via WLAN to Freemind software (V4.0, Vishee Inc.) for processing and were visualized on an interface displaying an avatar. The avatar’s color spectrum dynamically reflected the participant’s physiological state, with shades of purple and red indicating heightened tension, transitioning to blue and green upon successful relaxation.
Each 20-min session consisted of two sequential components: (1) a 5-min-guided abdominal breathing exercise with standardized audio prompts directing inhalation and exhalation at a default rate of six breaths per minute, and (2) a 15-min progressive muscle relaxation exercise, during which participants received auditory instructions to tense and release muscle groups sequentially, progressing from the toes to the head.
Cognitive trainingCognitive training is grounded in the theory of neuroplasticity, which seeks to restore impaired cognitive functions by targeting specific cognitive domains through repetitive, standardized, and problem-oriented tasks [6]. Our intervention targeted cognitive control, a process of employing executive functions, which refers to the ability to focus on goal-relevant information and regulate thoughts and behaviors to achieve internal objectives [25]. Cognitive control encompasses several key components, including attention, working memory, and goal management [26].
This study implemented cognitive training via the Adaptive Cognitive Evaluation (ACE) software, named in Chinese as Jiyibao, which held a Software Copyright Registration Certificate from China (Registration Number: 2025SR0243028). This tablet-based application included 12 modules designed to train attention, working memory, and goal management. Attention training incorporated stroop test, boxed, and sustained attention modules to improve focus under both distracting and non-distracting conditions. Working memory, the ability to actively maintain task-relevant information, was targeted through modules such as delayed working memory, mental rotation, spatial span, and spatial cueing. Goal management, which involves adapting goal-directed behaviors in response to situational changes, was trained using flanker, task switch, and tap and trace. Additionally, the basic reaction time module assessed and trained response speed, while the discrimination module evaluated and enhanced object differentiation ability.
To ensure the effectiveness of the training, the ACE software dynamically adjusted task difficulty based on an 80% accuracy threshold. The primary variable for adjustment was the response time window: incorrect or delayed responses triggered an extension of the response window, while correct responses resulted in its reduction. This adaptive mechanism mitigated practice effects, ceiling effects, and floor effects, ensuring optimal cognitive load throughout training.
Each session included two modules, following a rotation schedule outlined in Table 1, covering multiple cognitive domains while preventing tasks fatigue. Cognitive training was conducted five times per week for 6 weeks, with each session lasting 20–25 min.
Table 1 The routine of cognitive trainingMeasuresEye-tracking technology was conducted to compare cognitive function before and after the intervention in both groups. One consideration was selecting appropriate ET tasks to assess CRCI. ET tasks generally fall into five basic types: saccades, fixation, smooth pursuit, visual search, and social cognition, with saccades and fixation being the most commonly used [16]. Previous research on Alzheimer’s disease has shown that saccade task parameters primarily reflect impairments in executive function [18]. Furthermore, the cognitive domains assessed by the selected ET paradigms needed to align with the targeted intervention areas of this study. Therefore, the fixation stability test and the pro/anti-saccade test were chosen as the primary comparison tasks, with metrics derived from these tasks serving as the main outcome measures. The smooth pursuit and free-viewing were included for exploratory purposes, as they offer additional understanding of visual processes.
Fixation stability testParticipants were required to maintain their gaze on a white dot at the center of the screen while ignoring distracting signals. Fourteen trials included an interference dot, while another fourteen did not. Each trial lasted for 5 s, with trials alternating between interference and no interference.
Three indicators were generated: (1) fixation number, which counts the total number of fixations in a trial, a higher number indicates poorer gaze continuity; (2) fixation time, which calculates the average duration of all fixations in a trial, a shorter duration suggests poorer fixation stability; and (3) saccade distance, is the average of total saccade amplitude in a trial and a larger value indicates a greater deviation from the target.
Pro/anti-saccade test (PS/AS)Participants were asked to fixate on the center of the screen. When a solid dot appeared, they continued looking at it; when a hollow dot appeared, they looked in the opposite direction. The test included four pro-saccade trials followed by four anti-saccade trials, repeating the sequence.
Two indicators were generated: (1) starting speed, the time from the appearance of the target to the initiation of the saccade; and (2) moving speed, the average speed of eye movement after initial saccade.
Smooth pursuit testParticipants were instructed to focus on a black dot on the screen and follow its trajectory with their eyes while keeping their head still. Two indicators were generated: (1) breakaway time, which adds up the duration in each trial when the fixation was 100 pixels away from the moving stimulus; a longer duration indicates poorer pursuit performance; and (2) start-up speed, the speed during the initial 100 ms of a trial, a lower value indicates impairment in the initial tracking phase.
Free-viewing test (FV)Participants were presented with 35 still images, each displayed for 10 s. Six indicators were generated: (1) fixation number, (2) saccade number, (3) average fixation time, (4) total fixation time, (5) average saccade distance, and (6) total saccade distance total saccade distance.
Statistical analysisAnalyses were performed in R (version 4.4.1; R Core Team, 2024). Feasibility was assessed by the participation rate. To evaluate the preliminary efficacy of the intervention, within-group changes were analyzed using paired t-tests or Wilcoxon signed-rank tests, depending on the data distribution. Between-group differences were compared using independent t-tests or Mann–Whitney U tests, as appropriate. All statistical tests were two-tailed, with a p-value of 0.05 considered statistically significant. To control for multiple comparisons and reduce the risk of type I error, the false discovery rate (FDR) correction was applied where necessary.
Comments (0)