Within this demographically and socioeconomically diverse patient population, we characterize factors associated with LTSC nonattendance, delayed LTSC visit initiation, and LTSC visit disengagement among survivors of cancer diagnosed in childhood and adolescence. Seventy-nine percent of survivorship-eligible survivors diagnosed 2011–2019 initiated LTSC at TXCH. This attendance exceeds rates reported by other similar childhood cancer survivorship programs in the United States that, similar to TXCH, lack a philanthropy-based payer system[5, 6, 8, 20,21,22,23,24] and approaches the 85% attendance rate reported by the After Completion of Therapy Clinic at St. Jude Children’s Research Hospital[25], which provides substantive financial resources to patients to support their travel to participate in survivor-focused care. Many of our findings were similar to published studies indicating higher likelihood of LTSC attendance among Latino survivors[6], those treated with both chemotherapy and radiation (vs. surgery alone)[5, 6, 21, 26], and those who are privately insured[22, 24]. In our population, patients treated with radiation alone were less likely to attend LTSC, which may reflect fragmentation in care as radiation is provided to TXCH patients through a partner institution. Our findings were also concordant with published reports suggesting lower LTSC attendance among older survivors[6, 8, 20,21,22,23,24], non-White[20, 25] or Black survivors[5, 21], survivors with a non-leukemia diagnoses[8, 23], and survivors who are uninsured[6, 21,22,23, 25] or who have public insurance[5, 22, 23]. In contrast with published reports, our study did not find an association between LTSC attendance and distance traveled[5, 8, 21, 23, 26, 27] or with area-based deprivation[24, 26] and other indicators of socioeconomic status[27].
Our results also provide novel insight into follow-up patterns among survivors treated for cancer in childhood, demonstrating the negative impact of delayed initiation of survivorship care on continued survivor engagement with the clinic. In our study population, survivors who initiated survivorship care more than 5 years after the end of cancer treatment were more likely not to return for continued survivorship care. Moreover, survivors of childhood leukemia were among those most likely to initiate care early after treatment completion, and thus also most likely to remain engaged. Conversely, survivors of childhood solid tumors or CNS tumors were less likely to attend LTSC, initiate care early, or maintain engagement, which is consistent with findings from previous studies[7, 8]. Differences in survivorship care by cancer type may be influenced by system-level factors and institutional practices[7]. For example, survivors of CNS tumors may be directed to subspecialty clinics rather than survivorship clinics[8, 28]. Local institutional practice may also contribute to the superior attendance and engagement observed among leukemia survivors, i.e., a standard of practice adopted in 2018 that outlines a 5-year-long shared care model between the primary oncologist and the LTSC provider for the transition of patients with acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) from treatment to survivorship. Once children with ALL and AML complete treatment, they are moved to an institutional practice standard that specifically addresses the transitional time from leukemia treatment to survivorship. The treatment plan includes off therapy evaluations (such as complete blood counts and liver function tests) as well as a reminder to refer to the LTSC at 24 months from end of therapy. This approach is unique to leukemia survivors at our center and exemplifies characteristics marking successful care transitions in pediatric populations, e.g., having an established diagnosis and/or medication needs, initiating transition when patients are still requiring more frequent than annual follow-up, and introducing transition planning early[29,30,31]. Given the apparent benefits of this primary oncology/LTSC shared care approach to improving LTSC attendance and engagement, we plan to expand this practice to include other TXCH cancer populations, including solid tumors and CNS tumors, and recommend that pediatric oncology clinics consider adopting a similar model in transitioning patients from treatment to survivorship.
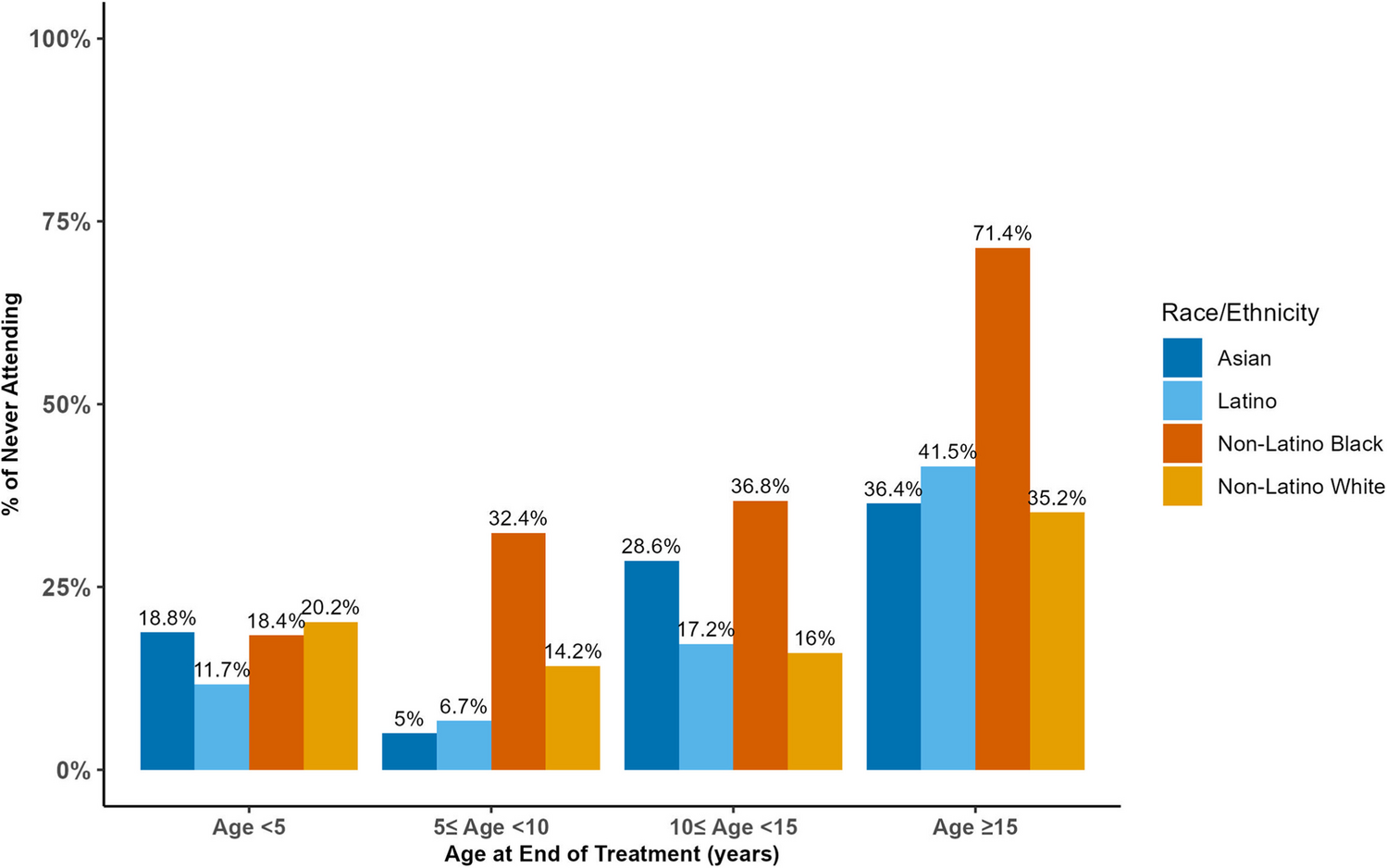
Several factors contributing to nonattendance in our population are well-known, such as older age at diagnosis or end of treatment. Adolescents and young adults are a highly mobile population and particularly vulnerable to the financial, social and psychological impacts of the cancer experience[32]. We also note that public insurance and uninsured status were associated with LTSC nonattendance and LTSC disengagement, recapitulating previous findings of lower LTSC attendance and engagement among older, publicly insured survivors[24]. Insurance-related disparities with respect to access to health services are most prominent in non-Medicaid expansion states such as Texas[33]. Moreover, while the Affordable Care Act offers protections to individuals aged 18 to 25 years old and to those with chronic health conditions[34], many survivors experience insurance instability and disruptions as they enter adulthood[33], which is known to impact survivor access to preventive care and treatment as well as their survival after cancer[35]. We also observed Latino survivors as most likely to attend LTSC. A prior study conducted in Latino survivors of childhood cancer identified two factors that were strongly predictive of intent to receive follow-up care in the next 2 years were greater self-efficacy and having health insurance[36]. One possible explanation for this effect in our study population is the prevalence of Spanish-speaking providers and staff as well as in-person language services that are available to support Latino access to care. Early entry to survivorship care, e.g., 2–5 years from end of treatment, provides a critical opportunity to promote self-efficacy as well as to identify and address anticipated changes in residence, insurance status or payer, vocational or educational status and financial wellness as survivors enter adulthood. As observed by other groups, non-Latino Black survivors, particularly older survivors, were least likely to be seen in LTSC. Qualitative assessment of factors driving this observation, including an evaluation of insurance related barriers, is needed to inform tailored approaches to engagement and education to address this disparity.
Study strengths include the large sample size, diverse population, lifelong access to survivorship care that promotes inclusion of cancer survivors across the lifespan, evaluation of a broad spectrum of factors contributing to LTSC attendance, e.g., language spoken, distance traveled, and area-based measures, and inclusion of factors predictive of survivor engagement beyond the first LTSC visit. This study also has some limitations. The study time frame was designed to begin with the year of EPIC® implementation at Texas Children’s Hospital to facilitate data abstraction: decades of LTSC data from years prior to 2011 were not available for analysis. Many of the patients diagnosed from 2011 to 2019 were seen in LTSC during the COVID-19 pandemic, during which time telehealth visits were more prevalent at our center and elsewhere[37]. Though we did not distinguish telehealth from in-person visits for this study, there are advantages to telehealth as a more accessible means for obtaining survivorship services[38], and this may have impacted attendance rates. We did not include survivors treated with surgery alone, nor did we include those who are treated with allogeneic transplantation and are at an exceptionally high risk for late effects, early morbidity, and mortality. Although this is a single institution study, TXCH is a referral center for childhood cancer, with 500–600 children diagnosed each year in a diverse population that is ~ 50% publicly insured and ~ 11% rural. Our internal referral practices and population may limit the generalizability of the findings to the broader pediatric cancer survivor population. Data utilized to determine payer status and area-based measures were collected from the electronic health record, which necessitates contact with the hospital system and may not reflect interim gaps in insurance coverage or changes in residence that occur between contact points with Texas Children’s. Limiting our analysis to the first and most recent LTSC visits precludes a more detailed understanding of adherence to annual follow-up, which would require a more in-depth investigation that includes longitudinal payer data, residence, and area-based assessment over time.


Comments (0)