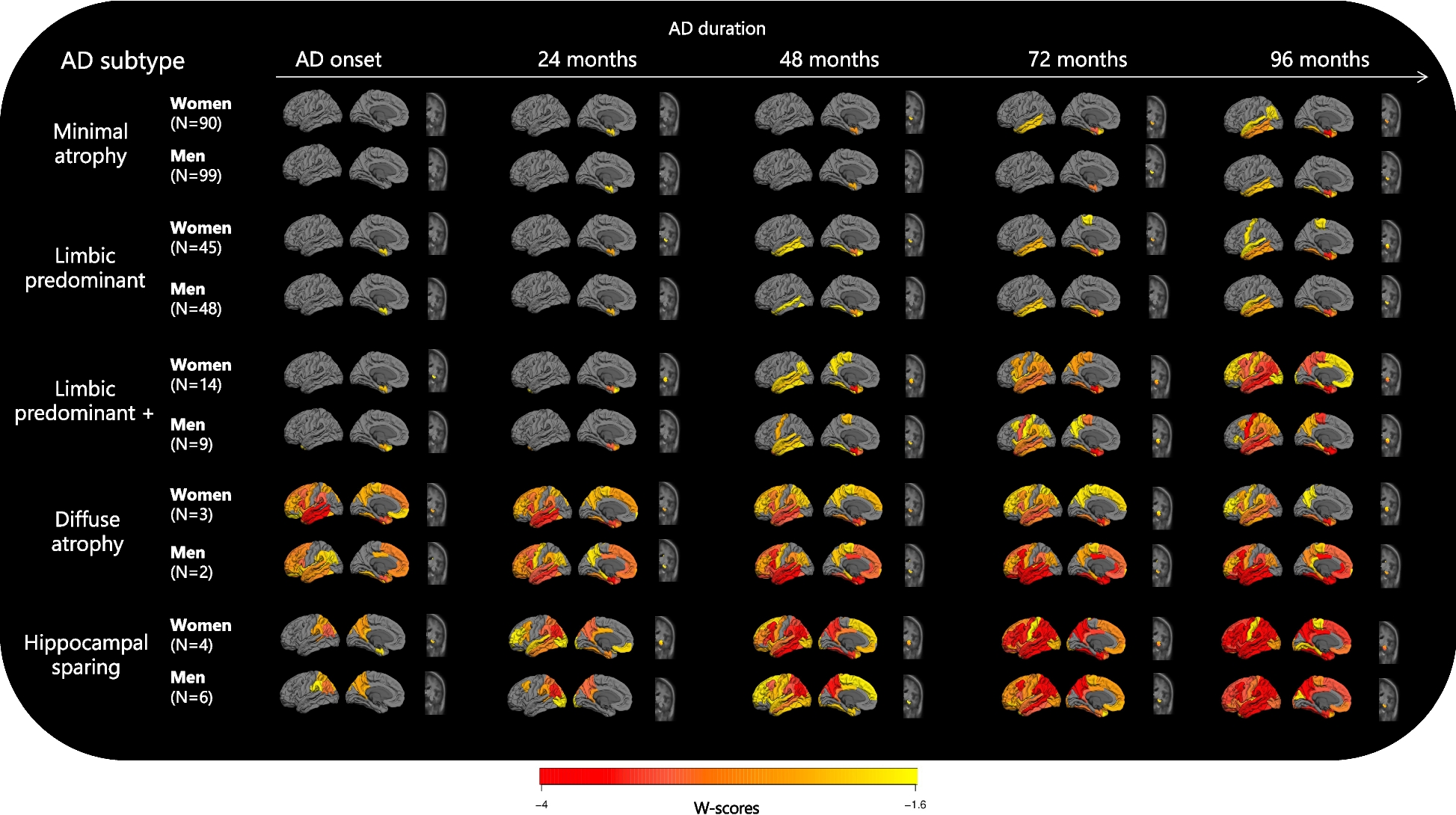
In our study, we investigated sex differences within five AD trajectories along with cognitive trajectories characterizing such patterns in a sample comprising three international cohorts. Our findings demonstrated that, although men and women can present with a similar AD trajectory characterized by a distinct pattern of brain atrophy over time, there are persistent sex differences, emphasizing the importance of discerning features intrinsic to the AD trajectories from those influenced by sex-related factors.
Regardless of sex, men and women assigned to the same subtype according to Poulakis et al. [12] followed a shared trajectory of atrophy. However, women with AD have been described to present with faster atrophy rates compared to men [9] and, accordingly, women across the AD trajectories presented faster atrophy progression over time compared to men. Lee et al. [21] described more rapid cortical thinning in AD signature regions in women. This observation remains noteworthy, especially considering that there were no differences in cortical thickness between sexes at baseline [21]. These findings are in line with the MA, LPA, and LPA+ trajectories of the mediotemporal pathway, where women and men within the same trajectory displayed comparable patterns of cortical atrophy at disease onset, with women showing faster progression of atrophy over time. Regarding the hippocampus, in our AD sample, which consisted entirely of amyloid-β positive individuals, women showed atrophy earlier in the disease than men, this faster rate of hippocampal volume loss is consistent with Koran et al. [22], who described women to exhibit a faster rate of hippocampal volume loss in the presence of high CSF total tau and low CSF Amyloid-β 42. Remarkably, women in our overall sample had significantly higher CSF total tau. Specifically, in our study, the LPA trajectory exhibited a trend of elevated CSF total tau levels in women compared to men. Interestingly, hippocampal sclerosis and TDP-43 have been suggested to be more frequent in the LPA subtype of AD, along with a higher prevalence of women [2]. Upon stratifying the AD trajectories by sex, we found the hippocampal atrophy to be a consistent characteristic of women independently of the AD trajectory. Additionally, hippocampal volume has been described to be a significant predictor of progression to mild cognitive impairment (MCI) and AD in women, but not men, regardless of AD biomarker status [23]. Women in the LPA+, DA and HS showed hippocampal atrophy already at disease onset, which may suggest that hippocampal atrophy at MCI stage may predict progression to AD in these specific subtypes.
WM hyperintensities have been consistently related with an increased risk of dementia later in life [24, 25]. In our study, we employed WM-hypo, which have been strongly correlated with WM hyperintensities [3, 14], to assess WM abnormalities. We found that women consistently exhibited a higher burden of WM-hypo across trajectories compared to men. Significant negative correlations between WM alterations and education have been reported [26], accordingly, women in the MA and LPA trajectories, who happen to be less educated than men, showed higher WM-hypo burden. Additionally, individuals with higher WM hyperintensities burden have been described to present with more GM atrophy in the temporal lobe expanding to frontal regions, hippocampus, insula, amygdala and cingulate [26], which aligns with the more extended atrophy presented in women compared to men in our trajectories. Lohner et al. [27] described that WM hyperintensities burden between men and women did not differ before menopause but it did differ after menopause, being then higher and more accelerated in women compared to men.
The prevalence of LPA has been described to be higher in women compared to men, a subtype also characterised by older age. Interestingly, upon stratification of the LPA+ trajectory, it was observed that men were predominant in the older age group within this subtype, potentially leading to an overestimation of age in LPA+. Low education is a recognized risk factor for dementia in both men and women [28]. However, historical disparities in educational opportunities have led to a higher prevalence of this risk factor among women compared to men [7]. Accordingly, we observed that women had significantly lower levels of education than men, particularly in the MA and LPA trajectories. While cross-sectional studies have identified MA as a subtype associated with lower education [2], this observation may be influenced by the lower educational level of women within the MA subtype. Despite lower education levels, women with AD have been described to experience a slower cognitive decline compared to men with AD [10], which aligns with the LPA+ trajectory, and is consistent with trends observed in the MA trajectory. Moreover, previous research within the ADNI cohort has shown a verbal memory advantage in women, both in normal ageing and MCI [7]. Notably, women in the LPA+ trajectory exhibited less decline in a verbal memory task compared to men. This advantage in verbal memory among women may delay the diagnosis of AD, potentially contributing to the higher burden of atrophy observed in women at the time of disease diagnosis, including the hippocampal atrophy already present at disease onset within the LPA+, HS and DA trajectories, but not in MA and LPA which are characterised by significantly fewer educated women. Studies have shown that women with MCI tend to demonstrate better verbal memory function than men, despite having similar levels of AD pathology [29]. This suggests that women may have a greater resistance to pathological burden before the clinical onset of AD; however, once clinical symptoms manifest, women exhibit a faster rate of progression [21]. Furthermore, the sustained advantage in verbal memory among women, even in the presence of hippocampal atrophy, may be influenced by hormonal effects. Estrogen, in pre-menopausal women, has been associated with protective effects against amyloid-β toxicity through the upregulation of antioxidant enzymes, effects that diminish post-menopause, making women more vulnerable to amyloid-β toxicity [30]. Additionally, earlier age at menopause and late initiation of hormone therapy have been associated with increased tau vulnerability [31].
While cognitive function is typically the focus of most AD research, it is essential to acknowledge the presence of neuropsychiatric symptomatology that accompany the disease, with some symptoms exhibiting sex-specific prevalence rates [32]. Our study identified trends within the LPA+ trajectory, where men displayed a higher propensity to apathy compared to women, a trend consistent with findings from previous literature [5, 10, 32]. Apathy, a common non-motor symptom in Parkinson’s disease (PD), has been associated to atrophy in the precentral gyrus [33], which was observed earlier in men within the LPA+ trajectory. Interestingly, alpha-synuclein burden may have contributed to the steeper cognitive decline observed in LPA+ men, as it has been linked to worsen cognitive decline in AD [34]. Notably, although men within the MA trajectory did not present with more atrophy than their female counterparts in any specific region, they displayed a tendency towards increased motor symptomatology compared to women. This increased motor symptomatology may be attributed to a higher burden of alpha-synucleinopathy, a hallmark of PD and Dementia with Lewy bodies (DLB), both characterised by motor alterations. Additionally, men with DLB have been described to be more likely to present with parkinsonism compared to women [35]. These findings underscore sex-specific differences in neuropsychiatric symptoms within AD trajectories.
This study contributes with new insights to the existing body of literature on sex differences, as it represents the first exploration of sex differences in AD atrophy trajectories, while also considering cognitive performance over time and clinical symptomatology. However, we were not able to examine which factors might influence such trajectories due to the lack of women health data, including reproductive lifespan, and other estrogen exposure-related factors such as number of pregnancies and use of hormone replacement therapy [5]. The strict inclusion criteria employed in the ADNI cohort may have restricted the heterogeneity within the study population, but to mitigate this limitation and enhance sample heterogeneity and population representation, we incorporated data from AIBL and J-ADNI cohorts. Working with a large sample enabled us to identify smaller subtypes that may have otherwise been overlooked [36]; however, the DA and HS trajectories were too small to draw meaningful conclusions regarding sex differences. In the future, including MCI amyloid-positive individuals would help tracking the disease from its earlier stages, enabling to observe trajectories over longer periods of time, as well as increasing the sample size, particularly for LPA+, DA and HS trajectories. In addition, incorporating alpha-synuclein measures could provide deeper insights into the distinct AD trajectories.








Comments (0)