
Remember me







The SDOH score was derived from self-reported data in the NHANES dataset, which utilizes a stratified, multistage probability sampling design. This approach ensures the sample accurately represents the U.S. population across diverse demographic and socioeconomic groups. Data collection follows a standardized process with stringent quality control measures, ensuring the reliability and consistency of the self-reported information. The use of standardized questionnaires and trained interviewers helps minimize measurement errors, thereby strengthening the validity of the SDOH score as a comprehensive measure of social determinants of health.
The NHANES, conducted by the National Center for Health Statistics (NCHS), assesses the health and nutritional status of the U.S. population. All participants provided written informed consent, ensuring their voluntary participation and adherence to ethical research standards. Additionally, the study protocol was rigorously reviewed and formally approved by the NCHS Ethics Review Committee, ensuring compliance with ethical guidelines and safeguarding participant rights and welfare throughout the research process [18].
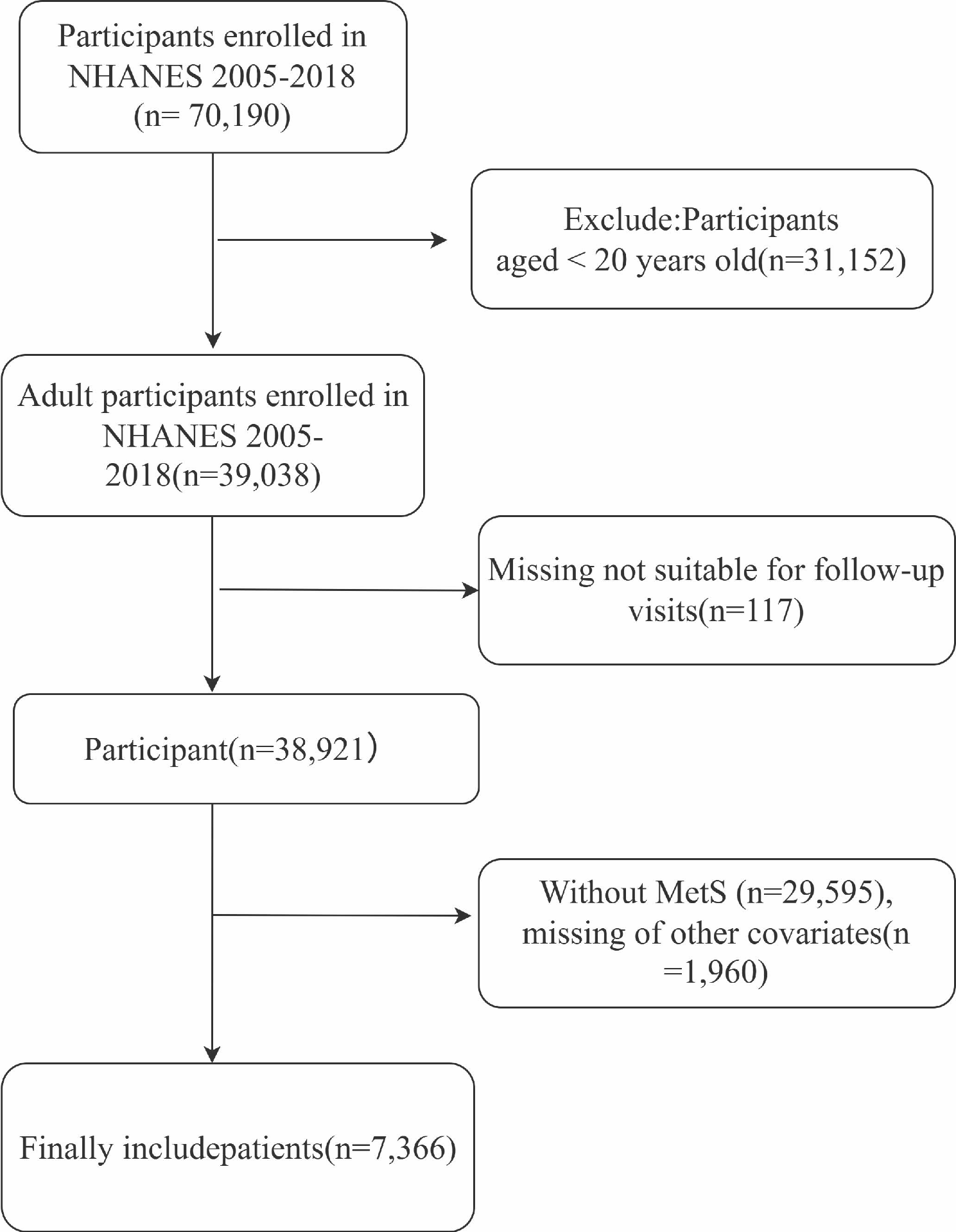
Study populationIn this cohort study, we initially considered 70,190 participants from NHANES between 2005 and 2018. To refine the sample and ensure its relevance, we applied specific exclusion criteria. Participants under the age of 20 were excluded, as were those without MetS or individuals missing key covariate data required for the analysis. After applying these criteria, the final sample consisted of 7,366 eligible participants, with the selection process outlined in Fig. 1.
Fig. 1
The flow chart of the included participants in this study
Definition of SDOH scoreSelf-reported data on 8 sub-items of SDOH across 5 domains were operationalized according to the criteria outlined in the U.S. Healthy People 2030 initiative and two previous studies, with a cumulative measure of unfavorable SDOH calculated for analysis [11, 19]. These domains include economic stability (employment status, family poverty-income ratio, and food security), education access and quality (education level), healthcare access and quality (health insurance coverage and type of health insurance), neighborhood and built environment (homeownership), and social and community context (marital status). The specific definitions of these SDOH domains and sub-items are provided in Table S1. To simplify the analysis, these SDOH items were dichotomized into favorable or unfavorable levels based on conventional cutoff points. The cumulative number of unfavorable SDOH was determined by summing the 8 dichotomized SDOH items, with a value of 0 representing a favorable level and a value of 1 representing an unfavorable level. To more effectively assess the association between SDOH and mortality in the MteS population, SDOH was categorized into quartiles: Q1 (0–1), Q2 (2–3), Q3 (4), and Q4 (≥ 5) [20]. Additionally, sensitivity analyses were conducted using three-quarter spacing [21].
Definition of MetSMetS in adults was defined based on the criteria established by the National Cholesterol Education Program’s Adult Treatment Panel III report [22], which has been extensively validated in epidemiological studies, including those related to NHANES [23]. A diagnosis of MetS requires the presence of at least three of the following conditions: 1.Hyperglycemia, fasting blood glucose level ≥ 100 mg/dL (5.6 mmol/L) or the use of antidiabetic medications; 2.Reduced high-density lipoprotein cholesterol (HDL-C) levels, HDL cholesterol < 40 mg/dL (1.0 mmol/L) for men and < 50 mg/dL (1.3 mmol/L) for women, or the use of lipid-lowering medications; 3.Hypertriglyceridemia, triglyceride level ≥ 150 mg/dL (1.7 mmol/L).; 4.Abdominal obesity, waist circumference ≥ 102 cm for men and ≥ 88 cm for women; 5.Hypertension, systolic blood pressure ≥ 130 mmHg, diastolic blood pressure (DBP) ≥ 85 mmHg, or the use of antihypertensive medications. These criteria provide a standardized approach for identifying MetS in clinical and research settings.
Mortality outcomesThe NCHS provided the Public-Use Linked Mortality Files, which were used to determine mortality outcomes in this study. The primary outcomes assessed included all-cause mortality, as well as mortality due to cardio-cerebrovascular diseases (ICD-10 codes I00-I09, I11, I13, I20-I51 and I60-I69) and cancer (ICD-10 codes C00-C97).
CovariablesThe variables analyzed in this study included a range of demographic and socioeconomic factors. Age, sex, and ethnicity were recorded, with ethnicity categorized into four groups: Mexican American, Non-Hispanic Black, Non-Hispanic White, and Other. Smoking status was classified based on lifetime cigarette use into three categories: never (fewer than 100 cigarettes), former (more than 100 cigarettes but not currently smoking), and current (more than 100 cigarettes and actively smoking). Alcohol use was classified based on daily and binge drinking frequency: never (consumed < 12 drinks in a lifetime), former (consumed ≥ 12 drinks in one year but not in the last year, or did not drink in the last year but consumed ≥ 12 drinks in a lifetime), mild (≤ 1 drink per day for females and ≤ 2 drinks per day for males), moderate (≤ 2 drinks per day for females and ≤ 3 drinks per day for males), or heavy (≥ 3 drinks per day for females and ≥ 4 drinks per day for males) [24, 25]. Body mass index (BMI) (kg/m²) was calculated by dividing weight (kg) by height squared (m²) and categorized into three groups: <25 kg/m², 25–29.9 kg/m², and > 29.9 kg/m² [26]. Hyperlipidemia was defined as having elevated triglyceride levels of 150 mg/dL (1.7 mmol/L) or higher, total cholesterol levels of 200 mg/dL (5.18 mmol/L) or higher, low-density lipoprotein (LDL) levels of 130 mg/dL (3.37 mmol/L) or higher, or high-density lipoprotein levels below 40 mg/dL (1.04 mmol/L) in men and below 50 mg/dL (1.30 mmol/L) in women [27]. Additionally, individuals taking cholesterol-lowering medications were classified as hyperlipidemic. Hypertension was diagnosed using a combination of factors, including the use of antihypertensive medication, self-reported history of hypertension, and the average of three blood pressure measurements. A diagnosis of hypertension was made if the average systolic blood pressure was ≥ 130 mmHg or the average diastolic blood pressure was ≥ 80 mmHg, ensuring that both clinical measurements and self-reported data were considered in the diagnosis of hypertension [28]. Type 2 Diabetes mellitus (DM) was determined by self-reported diagnosis or current use of antihyperglycemic medications [29]. A diagnosis of cardio-cerebral vascular disease (CCVD) was indicated by any affirmative answer to having been informed of congestive heart failure, coronary heart disease, angina, a heart attack, or a stroke [30].
Statistical analysesSample weighting, clustering, and stratification were systematically applied throughout all analyses, which is essential for ensuring the results accurately represent the national population. This methodology accounts for the multi-stage probability sampling of NHANES. In the baseline analysis, the MetS population was categorized according to SDOH levels. Continuous variables were expressed as mean ± standard error (SE), and differences between groups were assessed using weighted anova. Categorical variables were presented as numbers (percentages) and compared using weighted chi-square tests. Kaplan-Meier (KM) survival analyses were conducted to estimate survival probabilities over time for all-cause and cause-specific mortality, stratified by SDOH status in the MetS population. Differences between groups were tested using log-rank tests. Multivariate Cox proportional hazards regression models were used to examine the relationship between SDOH and all-cause and disease-specific mortality in the MetS cohort. Multiple models were constructed with varying levels of adjustment: the crude model did not adjust for any covariates; model 1 adjusted for age, sex, ethnicity, alcohol use, smoking, and BMI; and model 2 (fully adjusted) further included DM, hypertension, CCVD, hyperlipidemia, cancer, and depression. To assess the stability of the model, we conducted sensitivity analyses by categorizing the SDOH into tertiles: Q1 (0–2), Q2 (3–4) and Q3 (≥ 5). A fully adjusted Restricted Cubic Spline (RCS) model was used to evaluate the non-linear associations between SDOH and mortality outcomes. The RCS analysis tests for non-linearity by comparing the fit of a linear model to one that includes spline terms. Specifically, a P-value for non-linearity < 0.05 suggests that the relationship between SDOH and mortality is non-linear and cannot be adequately represented by a linear model. Conversely, a P for non-linearity > 0.05 indicates that the relationship is linear and requires further testing.
In addition to the RCS analysis, we conducted a trend test (P for trend) to evaluate the linear relationship between mortality outcomes and increasing levels of SDOH. A significant P for trend < 0.05 suggests a consistent linear relationship, indicating that mortality risk increases progressively with higher SDOH scores. This combination of RCS and trend analysis enables a comprehensive evaluation of both non-linear and linear trends in the data.
In addition to evaluating the main effects of SDOH on mortality outcomes, we conducted subgroup analyses to identify potential effect modifiers. These analyses aimed to determine whether specific demographic and clinical factors—such as age, sex, race, alcohol use, BMI, and hyperlipidemia—might influence the relationship between SDOH and mortality risk. This approach is commonly used in epidemiological studies to understand how various factors may modify the impact of exposures on health outcomes.
All statistical tests were two-sided and P values less than 0.05 were considered statistically significant. Analyses were performed using R software.
Comments (0)