
Remember me








The disposition of participants is shown in Supplemental Fig. 2. In Study 1489, 314 and 315 participants were randomized to receive B/F/TAF or DTG/ABC/3TC, respectively, and are included in this analysis. In Study 1490, 320 and 325 participants were randomized to receive B/F/TAF or DTG + F/TAF, respectively. Six participants in the B/F/TAF treatment group of Study 1490 did not have postbaseline data available and were excluded from the analyses of weight. Overall, 506 participants from the B/F/TAF treatment groups across both studies received B/F/TAF in the OLE (Supplemental Fig. 2).
Baseline characteristics of participants in both studies, shown in Supplemental Table 1, were generally balanced across treatment groups and studies. The median HIV-1 RNA levels ranged from 4.4 to 4.5 log10 c/ml across treatment groups; median CD4 count ranged from 440 to 450 cells/µl. The majority of PWH (≥ 89%) were asymptomatic, and median BMI was 25 kg/m2 in all treatment groups and studies.
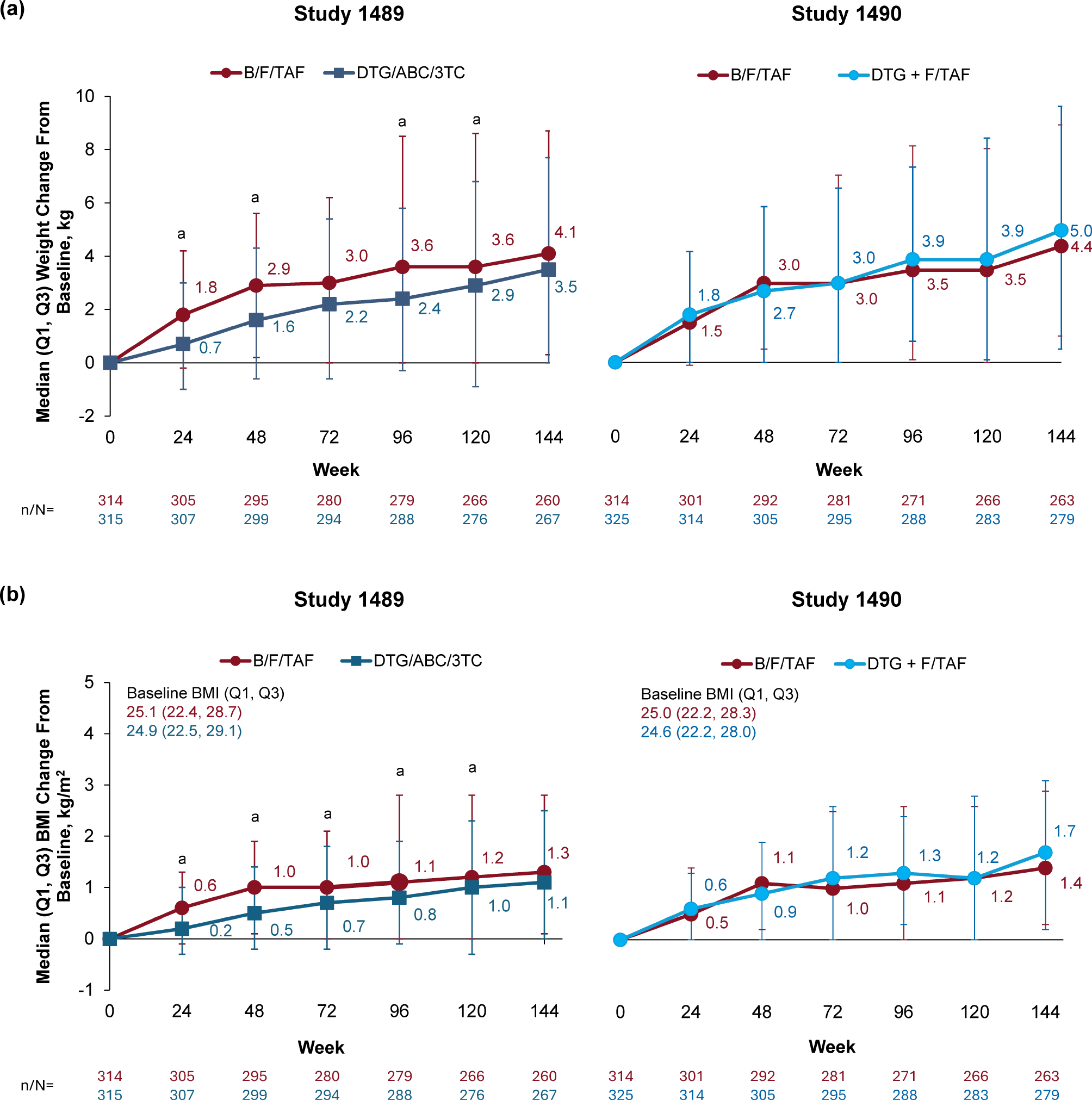
As-randomized analyses through Week 144Median weight and BMI changes over time by randomized group assignment for both trials are shown in Fig. 1. Both median weight and BMI increased over time in all treatment groups in both studies. In each trial, there was no statistically significant difference in change from baseline in weight or BMI at Week 144 in participants randomized to B/F/TAF versus DTG-based regimens (DTG/ABC/3TC in Study 1489 and DTG + F/TAF in Study 1490); the difference in median weight change between treatment groups ranged from 0.6 to 1.3 kg (Fig. 1A). The proportion of participants with ≥ 10% weight gain at Week 144 was similar between B/F/TAF and DTG/ABC/3TC (29.2% [76/260] and 24.7% [66/267], respectively; p = 0.28), and between B/F/TAF and DTG + F/TAF (30.4% [80/263] and 31.9% [89/279], respectively; p = 0.71).
Fig. 1
Change from baseline in (a) weight and (b) BMI through Week 144 in Study 1489 and Study 1490. ap < 0.05 from 2-sided Wilcoxon rank sum test to compare two treatment groups in each study. 3TC, lamivudine; ABC, abacavir; B, bictegravir; BMI, body mass index; DTG, dolutegravir; F, emtricitabine; Q, quartile; TAF, tenofovir alafenamide
Treatment-emergent diabetes mellitus occurred in 1.6% (19/1196) of participants, and treatment-emergent hypertension occurred in 7.4% (79/1073) of participants, across both studies (Fig. 2). The incidence of both conditions was similar between the B/F/TAF (diabetes mellitus: 0.7%; hypertension: 10.0%) and DTG/ABC/3TC (diabetes mellitus: 1.3%; hypertension: 6.9%) groups (Study 1489), and the B/F/TAF (diabetes mellitus: 2.1%; hypertension: 5.8%) and DTG + F/TAF (diabetes mellitus: 2.3%; hypertension: 6.5%) groups (Study 1490).
Fig. 2
Treatment-emergent diabetes mellitusa and hypertensionb through Week 144 in (a) Study 1489 and (b) Study 1490. aParticipants with medical history of diabetes mellitus were excluded. bParticipants with medical history of hypertension were excluded; events defined using search list “hyperglycemia/new onset diabetes mellitus (SMQ)– narrow scope” and “hypertension (SMQ)” in MedDRA version 23.1. 3TC, lamivudine; ABC, abacavir; B, bictegravir; DTG, dolutegravir; F, emtricitabine; MedDRA, Medical Dictionary for Regulatory Activities; SMQ, Standardized MedDRA Query; TAF, tenofovir alafenamide
Median fasting blood glucose levels remained relatively stable over time in all treatment groups, and median changes from baseline at Week 144 were not significantly different when compared between treatment groups (Study 1489: p = 0.64; Study 1490: p = 0.96; Supplemental Fig. 3).
Fasting lipid parameters were similar between treatment groups through Week 144, with minor increases from baseline observed in all groups (Fig. 3). The proportions of participants who initiated lipid-lowering therapy were also similar across treatment groups, and the impact of all three regimens on the TC:HDL ratio was minimal. Similar percentages of participants in each group in both studies experienced treatment-emergent graded laboratory abnormalities in fasting lipid parameters (Supplemental Fig. 4).
Fig. 3
(a–e) Fasting lipid parameters and (f) initiation of lipid-lowering agents through Week 144 in Study 1489 and Study 1490. 3TC, lamivudine; ABC, abacavir; B, bictegravir; DTG, dolutegravir; F, emtricitabine; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; Q, quartile; TAF, tenofovir alafenamide; TC, total cholesterol; TC: HDL, total cholesterol to high-density lipoprotein cholesterol ratio
Analyses through Week 240Baseline characteristics of the pooled B/F/TAF group, stratified by baseline viral load and CD4 count, are shown in Supplemental Table 2. Participants with a baseline viral load > 100,000 c/ml, CD4 count < 200 cells/µl, or both, were slightly older and less likely to be asymptomatic compared with participants in the other groups.
Analysis of change in weightWeight change over 240 weeks of B/F/TAF treatment according to baseline viral load and CD4 count is shown in Fig. 4A. The greatest weight gain was observed in participants with the highest viral load and lowest CD4 count at baseline, with the largest weight changes occurring in the first 48 weeks of treatment, followed by smaller weight changes every year thereafter. Between Weeks 48 and 240, weight change was similar for all groups, irrespective of baseline viral load and CD4 count.
Fig. 4
(a) Weight change from baseline over time and (b) absolute weight according to baseline viral load and CD4 count among participants receiving B/F/TAF up to Week 240 (pooled B/F/TAF groups). Includes participants with weight data at baseline and Week 240. B, bictegravir; c, copies; F, emtricitabine; Q, quartile; TAF, tenofovir alafenamide; VL, viral load
Multivariate regression modeling of weight change at Week 48through Week 240 (Supplemental Table 3) confirmed that the lower baseline CD4 count category (< 200 cells/µl) was strongly associated with weight gain at Week 48 and every timepoint thereafter up to Week 240. Except for Week 48, the higher baseline viral load category (> 100,000 c/ml) was significantly associated with weight gain at all timepoints. Higher baseline BMI and more advanced HIV disease status (AIDS or symptomatic) were also associated with weight gain at earlier timepoints.
Analysis of absolute weightParticipants with baseline viral load > 100,000 c/ml and/or CD4 count < 200 cells/µl at baseline had lower baseline weights. By Week 48, their weight was comparable to those who initiated B/F/TAF without high viral load or low CD4 cell count at baseline (range: 76.8–80.0 kg; Fig. 4B). This was consistent with multivariate linear regression modeling (Table 1), which identified lower CD4 count and higher viral load as independent risk factors for lower baseline weight, alongside Hispanic ethnicity, non-Black race, female sex, and younger age. From Week 48, baseline CD4 count and HIV-1 RNA levels were no longer associated with absolute weight, unlike Hispanic ethnicity, non-Black race, and female sex, which remained significant at most timepoints.
Table 1 Effect of baseline characteristics on absolute weight at baseline and Weeks 48–240Analysis of ≥ 10% weight gainTo understand factors associated with more clinically relevant weight gain, we stratified pooled participant data into those gaining ≥ 10% of their body weight at Week 240 versus those gaining < 10%. At Week 240, 40.6% of participants receiving B/F/TAF experienced ≥ 10% weight gain (median weight gain: 16.9%), while at any timepoint up to Week 240, 52.2% of participants receiving B/F/TAF experienced ≥ 10% weight gain.
In multivariate logistic regression modeling (Supplemental Table 4), a lower baseline CD4 count, higher baseline viral load, and baseline BMI categorized as underweight/normal were significant risk factors for greater odds of ≥ 10% weight gain at Week 240, compared with a higher CD4 count, lower viral load, and BMI classed as overweight, respectively.
Efficacy analysisEfficacy outcomes up to Week 240 have been published previously [25]. In the current analysis, virologic suppression occurred in the first 48 weeks for most participants in all viral load and CD4 count groups (Supplemental Fig. 5), coupled with a rapid increase in CD4 count through Week 48 (Supplemental Fig. 6), mirroring the time-course of weight gain.
Comments (0)