
Remember me
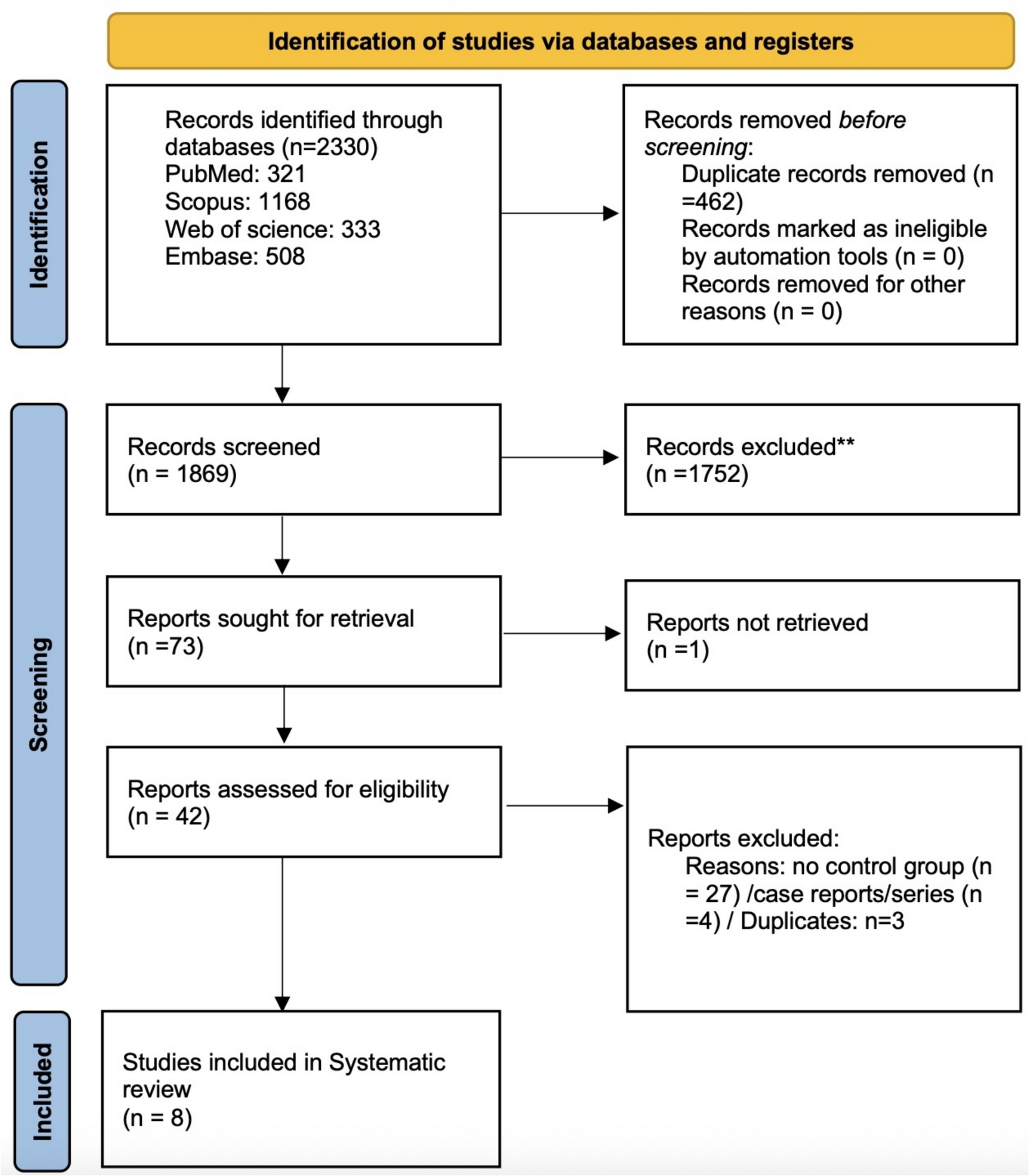
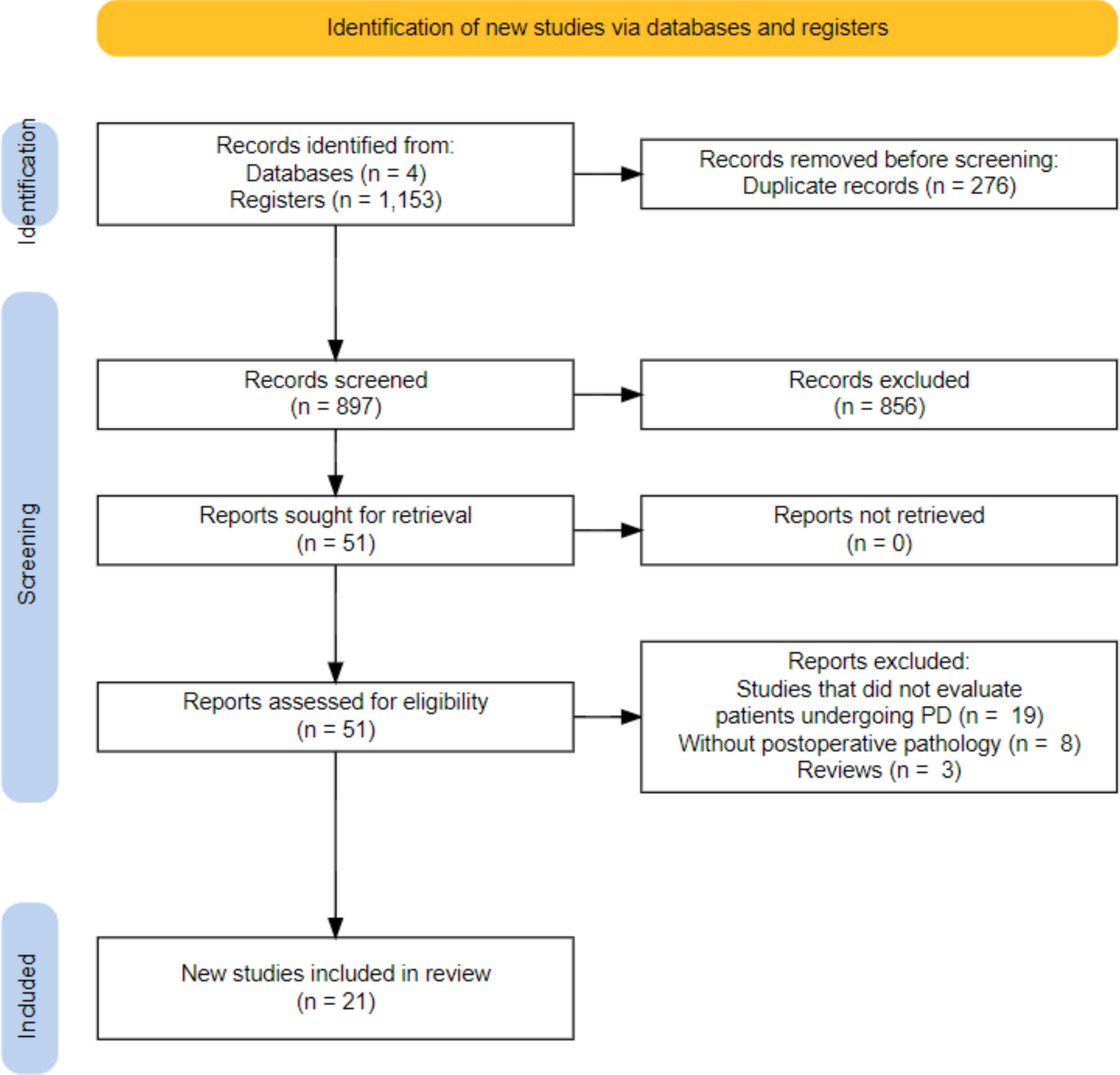
Using our search strategy, we identified 4744 references from the Cochrane Library (n = 265), PubMed (n = 2962), CINAHL (n = 493), Scopus (n = 965), and PsycINFO (n = 59). We removed duplicates automatically (n = 898) and manually (n = 15). Out of the 3831 references initially considered, we deemed 3633 references irrelevant after screening their titles and abstracts. Following full-text screening, we excluded 155 references that did not meet the inclusion criteria. Ultimately, we included 43 studies. Figure 1 shows the PRISMA flow diagram depicting the reference screening and selection processes.
Fig. 1
PRISMA flow diagram of the reference screening and selection processes
Overview of the Included StudiesThe 43 included studies spanned publication years from 2006 to 2024, with 13 conducted in the USA. Of these, 33 were descriptive studies, including qualitative (n = 19), mixed methods (n = 9), and quantitative (n = 8) designs; ten were experimental. Ten studies occurred in cancer centers or hospitals. Additionally, 20 studies included both patients with pancreatic cancer and their informal caregivers. Eleven studies had a sample size exceeding 100 patients and/or their informal caregivers. These included studies covered all cancer stages. Table 1 contains details of the included studies.
Table 1 The study characteristics (N = 43)The Supportive Care NeedsWe categorized the supportive care needs of pancreatic cancer patients and/or their informal caregivers based on the Fitch’s Supportive Care Framework for Cancer Care (Table 2) [18]. The descriptive studies examined the needs of both patients and informal caregivers (n = 11), patients only (n = 18), and informal caregivers only (n = 9). Only one descriptive study used a theoretical framework, the Stress Process Model, to guide the selection of study variables and instruments [51].
Table 2 Supportive care needs of pancreatic cancer patients and their family caregivers (descriptive studies, N = 33)Supportive Care Needs of Both Patients and Their Informal CaregiversAmong the studies reviewed, 11 identified supportive care needs shared by both pancreatic cancer patients and their informal caregivers. Ten of these studies included both patients and informal caregivers as participants, while one study focused solely on informal caregivers to explore the supportive care needs of both patients and informal caregivers. The most frequently reported need was informational support (n = 6), encompassing concerns related to disease, medication, nutrition, self-management, symptoms, treatment options, and delivery modes. Emotional needs (n = 4) were characterized by negative emotions, such as anxiety. Physical needs (n = 3) centered on issues like nutrition, pain, fatigue, gastrointestinal symptoms, and treatment complications. Practical needs (n = 3) included financial concerns and ethical/legal issues. Social needs (n = 2) included connections, family-related issues, and other general concerns, while spiritual needs (n = 2) focused on prayer. In contrast, psychological needs were not commonly reported in either group.
Patients’ Supportive Care NeedsEighteen studies identified the unique supportive care needs of patients with pancreatic cancer. Of these, 14 focused exclusively on patients, three examined both patients and informal caregivers, and one explored supportive care needs solely from the perspective of informal caregivers. Informational needs were the most frequently reported (n = 13), encompassing areas such as decision-making, disease management, diet, symptom management, treatment-related issues, and delivery methods. Physical needs (n = 8) primarily involved pain, fatigue, nutrition, digestive problems, and other general health concerns. Psychological needs (n = 4) included anxiety, body image, depressive states, and sexual concerns. Emotional needs, though less frequently documented (n = 2), involved feelings of fear, shock, sadness, being overwhelmed, uncertainty, and worry. Practical needs (n = 2) centered on daily living assistance and exercise. Notably, social and spiritual needs were not identified in the reviewed studies.
Informal Caregivers’ Supportive Care NeedsNight studies examined informal caregivers’ supportive care needs, with the majority identifying informational needs (n = 5), such as caregiving and decision-making, disease management, treatment, and symptom management. Practical concerns (n = 4) were also frequently reported, including challenges related to daily life, caregiving responsibilities, training, and financial issues. Emotional needs (n = 4) encompassed fear and the need for emotional support. Physical (n = 1) and psychological needs (n = 1) focused on the physical issues and stress associated with caregiving, respectively, while spiritual needs (n = 1) highlighted informal caregivers’ search for meaning. Notably, social needs were not reported in these studies.
Interventions to Meet the Supportive Care NeedsTen experimental studies examined the effectiveness of various interventions on the supportive care needs of patients with pancreatic cancer and/or their informal caregivers. These interventions were categorized based on the services or activities following the Supportive Care Framework for Cancer Care by Fitch [18]. Among the ten experimental studies, two implemented interventions that simultaneously addressed the needs of both pancreatic cancer patients and their informal caregivers.
Interventions Targeting Both Patients and Informal CaregiversAs presented in Table 3, the most targeted areas were psycho-educational support (n = 2), orientation/ongoing patient and family education (n = 1), adjustment/supportive counseling (n = 1), nutritional intervention (n = 1), and pain/symptom management (n = 1). One of the two studies developed interventions based on a theoretical framework and involved at least two types of professionals, such as nurses, social workers, oncologists, and dieticians (Table S2). Standard measures assessed included feasibility, distress levels (using a distress thermometer), components of intervention sessions delivered, care plans and referrals, and interviews. Interventions were delivered either in-person (n = 1) or via phone/video (n = 1), and were administered individually, to couples, or in group settings. The duration of the interventions varied, ranging from a single session to nine sessions. One study reported dosages of once per week or fortnightly, with sessions lasting between 20 and 99 min.
Table 3 Intervention strategies to meet supportive care needs of pancreatic cancer patients and their family caregivers (Experimental studies, N = 10)Interventions Targeting Patients OnlyMost interventions targeting patients have focused on pain/symptom management (n = 7), followed by adjustment/supportive counseling (n = 5), orientation/ongoing patient and family education (n = 3), psycho-educational services or activities (n = 2), and practical and functional assistance (n = 2) (see Table 3). One of the eight studies developed interventions using a theoretical basis. Four studies included interventions implemented by at least two types of professionals, such as physicians, nurses, chaplains, social workers, and oncologists. Eight studies had control groups. Standard measures assessed included quality of life, symptoms, and feasibility. Notably, four of the eight studies demonstrated statistically significant improvements in outcomes in intervention groups compared to control groups, as outlined in Table S2. The studies delivered the interventions in-person (n = 6) or through a hybrid approach combining in-person and phone/video methods (n = 2). Almost all interventions were delivered individually. The duration of the interventions ranged from a single session to an unlimited number of sessions until death. Most studies did not report the dosages of the interventions.
Comments (0)