
Remember me
The systematic search led to the identification of 493 papers from CINAHL, Cochrane Library, Medline (Ovid), Embase (Classic), and Web of Science. The non-systematic search of the PubMed database resulted in 42 studies, while Google Scholar and citation searching led to two results.
A total of 109 duplicates were eliminated electronically (53 papers) and manually (56 papers).
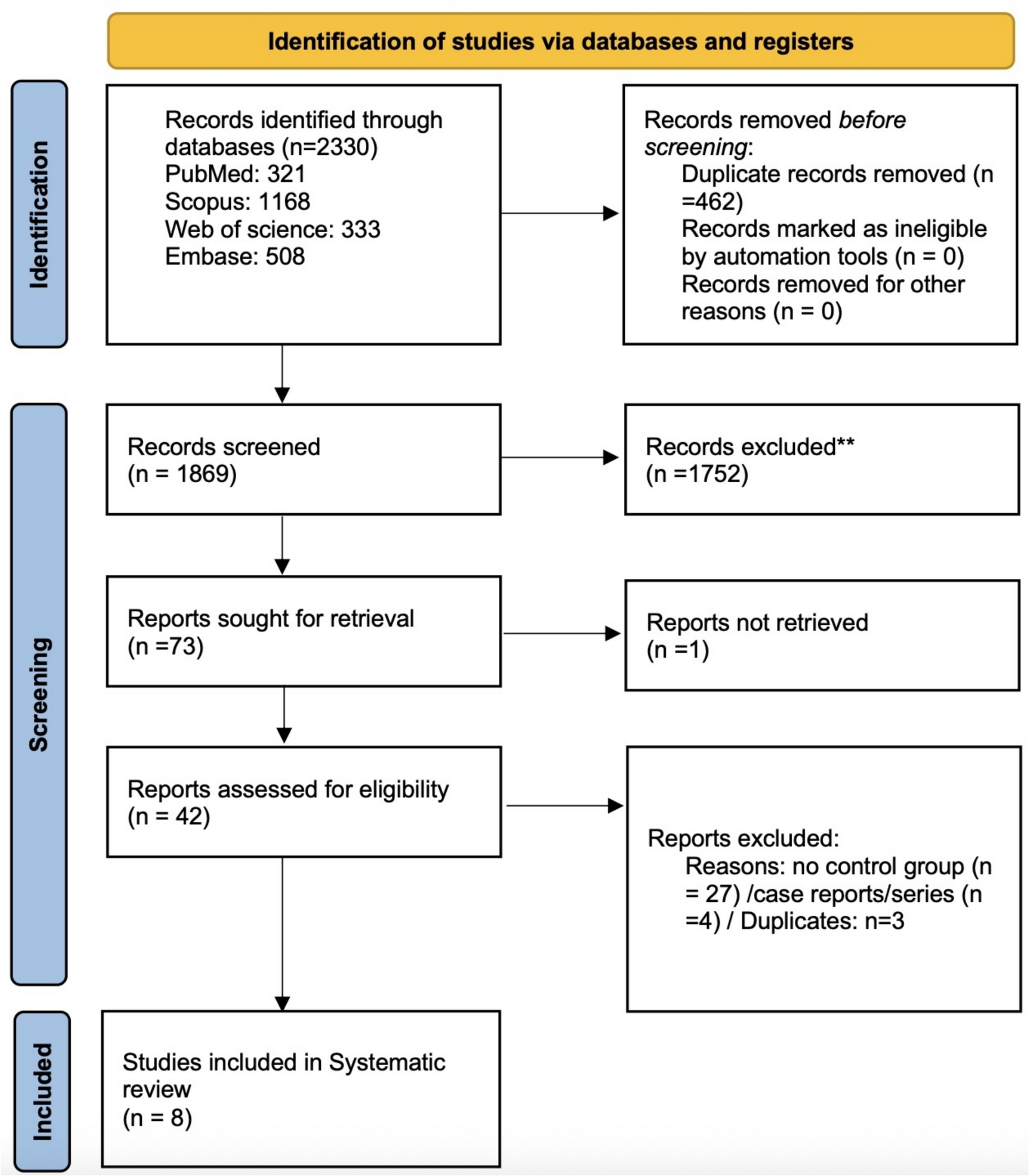
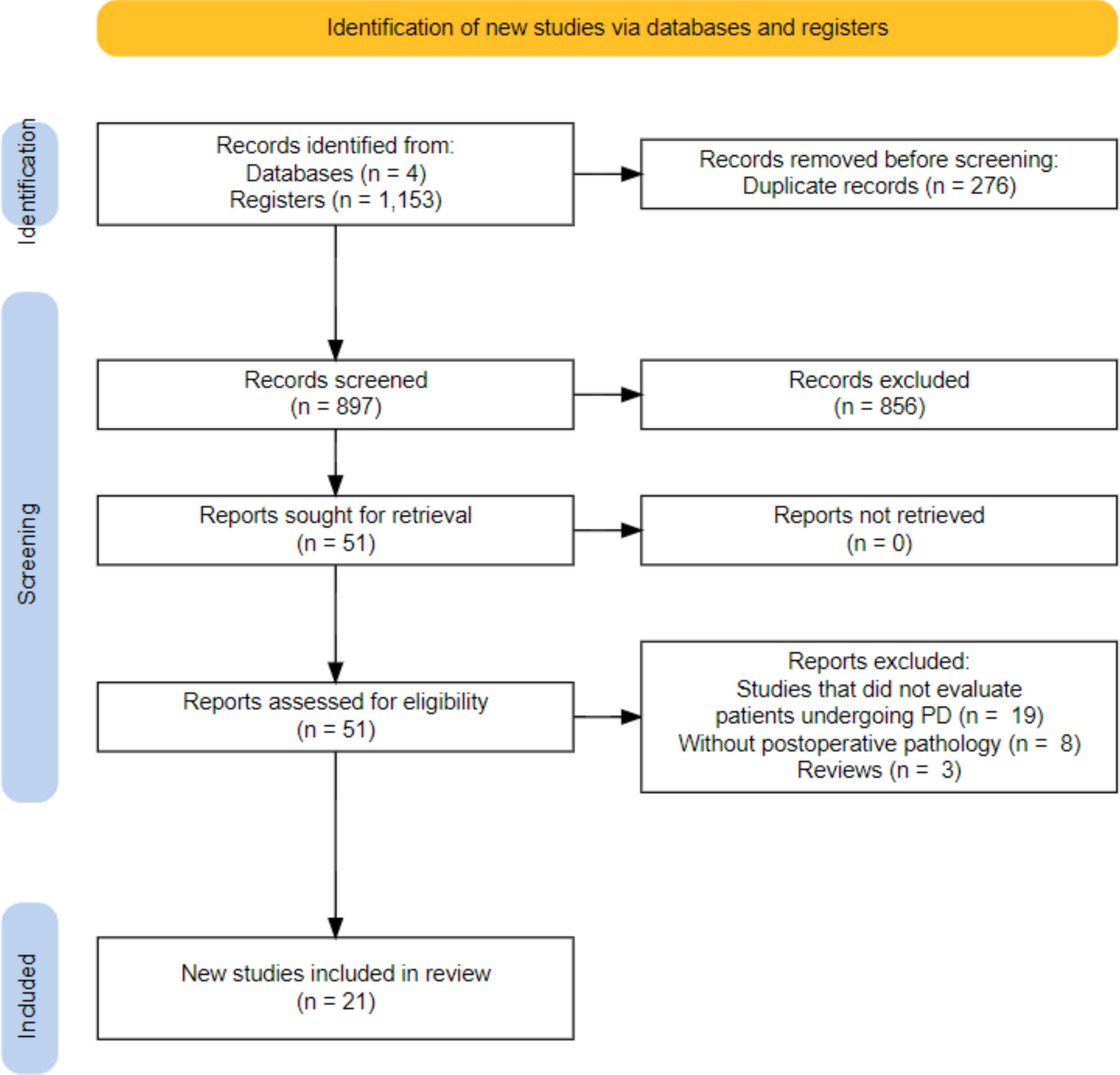
Screening the title and abstracts of 426 papers according to the inclusion and exclusion criteria led to removing 331 results. The remaining 95 papers were sought for retrieval, only 35 papers were found in full-text. The PRISMA flow diagram [76] illustrates the study selection process (Fig. 2). A total of 18 studies were eligible to be included in this review. It is important to note that no real-world studies were included in the analysis.
Fig. 2
PRISMA flow chart [76] showing the study selection procedure for this systematic review
Included Studies to Evaluate FGFR as a Predictive Marker in GI CancersThe following tables are the study and patients’ characteristics followed by the data extracted from each study (Tables 3 and 4).
Table 3 Study and patient characteristics of the clinical trials included in the systematic reviewTable 4 Extracted data from included studiesCCAll studies were single-arm phase 2 studies, except for the Ahn et al. study [83], published between 2020 and 2023. Three trials were multinational [79,80,81]—one study was conducted in China [82] and one in the USA [83]. Participant numbers ranged from 12 to 146 with a similar median age (48.5–59 years), predominantly including women.
Genomic testing has been performed by all studies. Most trials used NGS with different kits, except for one study [81], leading to the conclusion that the FGFR2 fusion and rearrangement is the most prevalent FGFR2 alteration in CC. Other methods including FISH [80, 82, 83] and RT-qPCR [80] were also used for FGFR2 detection. Two papers distinguished between fusion and rearrangements finding that most of the tumours have FGFR2 fusions [80, 81]. Testing for fusion partners showed in many studies that BICC1 is the main fusion partner [79,80,81]; yet, it did not correlate with the response rate [79]. However, Shi et al. found WAC as the most common fusion partner, namely in 10% of the cohort [82]. In the international trial of Goyal et al., this was the second most common fusion partner along with KIAA1217 in only 3.75% of the patients [81]. Abou-Alfa et al. conducted a molecular epidemiology study—9% of CC have FGFR2 alterations [79]. More specifically, Shi et al. tested 717 iCC tumour samples, 6.14% had detectable FGFR2 rearrangements by FISH [82].
The medications administered were pemigatinib, futibatinib, infigratinib, and ponatinib. The FIGHT-202 study investigated pemigatinib’s impact on patients with FGFR2 fusions or rearrangements, with other FGFR alterations and compared the outcomes with patients without FGFR alterations. The only responders were FGFR2 fusions and rearrangements patients with an ORR of 36%, three had CR and 35 had PR. This was the trial with the highest complete responders [79]. Shi et al. also administered pemigatinib to a smaller sample size (30 patients) in China. Comparing these two trials, Shi et al. had a higher investigator- (40%) and IRCC-assessed (50%) ORR [82]. Although the investigator-assessed median PFS was not reached, the IRRC-assessed median PFS was 6.3 months [82], being comparable to the FGFR2 fusion and rearrangement cohort in FIGHT-202 (6.9 months) [79]. The median OS in the FIGHT-202 study was majorly higher for patients with FGFR2 fusion and rearrangement (21.1 months) than other alterations (6.7 months) or no alterations (4 months) [79].
Javle et al. analyzed the FGFR2 status in 96 patients through NGS, FISH, or RT-qPCR. Eighty-one percent had FGFR2 fusions and 19% had other FGFR2 rearrangements. Administering infigratinib led to a comparable BICR-assessed and investigator-assessed median PFS (7.4 vs. 7.3 months) and median OS (11.8 months vs. 12.2 months). BICR observed 23.1% ORR, 1 CR and 24 PR, while the investigator-assessed ORR was 30.6% with only PR [80].
Goyal et al. performed genetic testing with a 324-gene-panel assay, discovering that 78% had FGFR2 fusions, and the rest had rearrangements. In those with FGFR2 fusions, fusion partners were found, 30% had BICC1 as fusion partner. Ten of 24 patients (42%) with BICC1 fusions and 25 of 56 patients (45%) with non-BICC1 fusions had a response. The ORR with futibatinib was 42%, including 1 CR and 42 PR. The median PFS was 9 months, and the median OS was 21.7 months, the highest among the reviewed CC studies [81].
Ahn et al. had the smallest cohort and intervened with ponatinib. Ten out of 12 patients had FGFR2 fusion or rearrangement tested by FISH or NGS. The trial resulted in the lowest ORR (9.1%) and lowest median PFS (2.4 months). The median OS was 15.7 months [83].
GC/OCStudies published between 2019 and 2023 explored gastric adenocarcinoma [85], gastro-oesophageal junction adenocarcinoma [87, 88], or both [86, 88]. Some trials were multinational [87, 88] and others in a single country [84,85,86]. Population size ranged from 21 to 155 patients and the median age spanned from 56 to 62 years.
Each study administered a different FGFR inhibitor except for Catenacci et al. and Wainberg et al. who administered bemarituzumab [87, 88]. Four papers concerned FGFR2 amplification and FGFR2b overexpression [84, 85, 87, 88], while Jiang et al. focused on FGFR2 mutation [86]. Detection methods used were NGS [84, 86, 88], IHC [85, 88], and FISH [85, 87]. In one case, there were inconsistencies between the testing method [85].
All studies performed genetic testing. Wainberg et al. analyzed 910 patients prior to enrolment. Thirty percent of those tested positive: 29% had FGFR2b overexpression, 4% had FGFR2 amplification, and 33% of those with amplification also showed FGFR2b overexpression. This study randomised 155 patients, 96% had FGFR2b overexpression, 17% had FGFR2 amplification, and 13% of the patients in the FGFR2b overexpression cohort had both FGFR2b overexpression and FGFR2 amplification [88].
Across all reviewed GC/OC studies, Won et al. achieved the shortest median PFS (3.5 months) along with reaching no response by administering the multi-kinase inhibitor, nintedanib. Nineteen percent of their 27 samples had FGFR2 amplification. Patients with FGFR2 amplifications tended to have a longer PFS than patients without such alterations (3.5 vs. 1.9 months, p = 0.92), but the difference was statistically insignificant. However, the three longest PFS (> 8 months) were in tumours without FGFR amplification. This study had the longest median OS among GC/OC studies being 13.5 months for the patients with FGFR2 amplification [84].
Tsimafeyeu et al. tested 17 tumour samples and found only one patient positive for FGFR2 amplification by both FISH and IHC. A percentage of 17.6 were positive by IHC and 11.8% were positive FISH. The study administered alofanib at different doses and reached an ORR of 5.26% at 50 mg/m2 among 19 evaluable patients (1 PR). The median OS was 7 months and the median PFS was 3.63 months like Jiang et al. (4 months) [85].
Combining anlotinib and a PD-1 inhibitor was done by Jiang et al., and they investigated regarding FGFR2 mutations. A percentage of 24.2 had FGFR2 mutations, and these tumours were significantly associated with target lesion reduction (OR = 14, p = 0.02). The ORR was 32.3% with 20 PR among all patients enrolled. Although it was statistically insignificant, there was a trend of FGFR2-M having a higher PFS and ORR than FGFR2-W after anlotinib [86]. The median OS was 11.1 months in the main, FGFR2-M and FGFR-W cohorts being the highest among the reviewed trials within this group [86].
Considering bemarituzumab, one multinational trial co-administered it with chemotherapy comparing it to sole chemotherapy agent mFOLFOX6. FGFR2b monoclonal antibody showed higher ORR (46.8% vs. 33.3%) and median PFS (9.5 months vs. 7.4 months); yet, these were statistically insignificant. They did not achieve a median OS in the intervention group; yet, in the placebo group, it was 12.9 months (p = 0.027) [88].
Catenacci et al. used FISH to differentiate the gradients of FGFR2b expression. Twenty-eight patients had high FGFR2b overexpression, four had moderate expression, 13 had low expression, and 11 had no or unknown expression. The ORR was 17.9% (5 PR) in high and 8.3% (1 PR) in low FGFR2b overexpression group. No response was seen in the moderate and no/unknown FGFR2b overexpression cohort [87].
HCCThe four studies on HCC were published between 2018 and 2022. Three studies were conducted internationally [27, 89, 90], one was in South Korea and Taiwan [91]. Participant numbers ranged from 95 to 954, with mainly male participants. Their median ages were comparable (59–62 years).
The two studies administering a predominantly FGFR4 inhibitor, performed genomic testing [27, 90]. Kim et al. utilized IHC and FISH to determine FGF19 positivity of the tumours retrospectively, followed by testing those positive tumours on FGFR4 and KLB expression. Out of 395 samples tested by IHC, 27% were positive for FGF19 staining (≥ 1%). They had 115 patients and 63% were IHC-positive for FGF19. Ninety-six percent of 53 IHC FGF19-positive tumours were assessed for FGFR4 and KLB mRNA expression. Ninety-six percent were positive [27]. Chan et al. conducted a dose escalation and dose expansion trial [90]. They only recruited patients positive for FGFR4 and KLB transcript expression by RT-qPCR. The FGF19 status was additionally tested by IHC. A trend for better response had been observed among the IHC FGF19-positive patients treated solely by FGF401. Again, here were inconsistencies between the testing methods. Seven IHC FGF19-positive samples were negative by RT-qPCR, and two FGF19 IHC-negative samples were positive by RT-qPCR. No statistically significant association was identified between FGF19-positive tumours and poor prognosis (p = 0.13) [90]. Fisogatinib resulted in 17% ORR (1 CR and 10 PR) in 66 FGF19-positive tumours. The patient experiencing a CR was in the 600-mg cohort. One patient experienced a PR in the 280-mg cohort, two in the 420-mg cohort, and seven in the 600-mg cohort. No response was seen in FGF19-negative patients or with an unknown FGF19 status confirming the FGFR4 pathway integration. Forty-one percent of IHC FGF19-positive patients had a radiographic tumour size reduction. The median PFS was longer for IHC FGF19-positive tumours (3.3 months) compared to IHC FGF19-negative tumours (2.3 months) [27]. In phase 1, a single agent FGF401 achieved an ORR of 6.8% (1 CR and 3 PR) among 59 HCC patients. The median OS was 5.72 months assessed in 45 patients. There was 1 PR in each of the combination arms of FGF401 + spartalizumab making an overall ORR of 8.33% [90]. During phase 2, in both Asian and non-Asian groups, two patients achieved a PR leading to the same ORR as the single agent in phase 1 [90].
No genetic testing was performed to determine the FGFR status in the RCTs [89, 91]. Kudo et al. randomized patients into a lenvatinib or sorafenib arm via a concealment method in a 1:1 ratio [89]. The masked independent review calculated the median PFS as 7.3–7.4 months in the lenvatinib arm, double that of the sorafenib arm (p < 0.0001). The ORR was statistically significantly (p < 0.0001) higher with lenvatinib (24.1% vs. 9.2%). The results for median OS were statistically insignificant [89]. Yen et al. performed a 2:1 randomization into a nintedanib and sorafenib arm [91]. The median OS was 10.2 months for nintedanib, which was comparable to sorafenib (10.7 months). The median PFS was 2.7 months for the nintedanib group, being lower than the sorafenib arm by a month. The ORR according to RECIST v.1.1 was calculated for nintedanib around 6.3% (2 CR and 2 PR) which was higher compared to sorafenib being 3.1% (1 PR). The mRECIST results were different as nintedanib had a lower ORR with 14.3% (2 CR, 7 PR), while sorafenib had 18.8% (6 PR) [91].
CRCBoth publications on CRC were RCTs [92, 93] published between 2018 and 2020. They were conducted in Germany [92] or internationally [93]. The number of participants varied from 53 to 768, predominantly male, with a median age of 62 to 63 years. None of the studies included results of FGFR status testing.
Ettrich et al. and Van Cutsem et al. investigated nintedanib’s effects randomizing patients into FOLFOX + nintedanib vs. FOLFOX + placebo [92] and nintedanib vs. placebo [93], respectively. Although the results were statistically insignificant, the median OS (difference of 7.2 months) and PFS (difference of 3.5 months) were numerically higher in the nintedanib + FOLFOX group. Unlike Van Cutsem et al., who did not have any responders [93], the ORR in Ettrich et al. study was 3.7% and 3.8% in the intervention vs. placebo cohort, respectively, with each 1 PR, yet statistically insignificant (p = 1.0) [92].
Van Cutsem et al. reported a statistically significant longer PFS in the intervention group according to the central review by 0.1 months (p < 0.0001) and to the investigator review by 1.2 months (p < 0.0001) [93]. The OS seemed numerically higher with nintedanib than with placebo; yet, it was statistically insignificant [93]. No association was identified between OS and either the baseline number of metastatic sites (1 vs. > 1) or the rectum as the primary tumour site. Nintedanib favours in cases with more than one metastatic site; yet, it cannot be ruled out that there is no difference at 95% Cl [93].
PCOnly two PC studies matched the inclusion and exclusion criteria. Both phase 1b studies were published in 2019. A Chinese neuroendocrine study administered surufatinib to 42 pancreatic NET patients [94]. Another trial co-administered dovitinib with gemcitabine and capecitabine to 24 pancreatic cancer patients in the USA [95]. The median age was 46 and 65.5 respectively. Both studies applied the ELISA kit to measure bFGF and FGF23 levels at baseline and during treatment. These trials enrolled predominantly men.
The pancreatic NET cohort had investigators’ and independent assessments [94]. They were variable regarding ORR of 19% vs. 12% (8 PR vs. 5 PR, respectively) [94]. A > 10% tumour shrinkage from baseline was observed in 61% of patients in the pancreatic NET cohort [94]. The investigator calculated a PFS of 21.2 months, while independent reviewers assessed it to be 19.4 months [94].
Ma et al. reported that the pancreatic cancer patients (n = 15) receiving dovitinib as first-line therapy, their median OS was 13.3 months, compared to the patients (n = 18) enrolled naïve to gemcitabine who had a shorter median OS, namely 9.5 months [95].
The plasma FGF23 levels increased in both studies. It increased significantly from baseline in best response patients with surufatinib (p < 0.0001) [94]. Dovitinib intervention resulted in four out of five patients having an increased FGF23 level from baseline during the first cycle of treatment [95]. However, both trials did not define how many of the patients had PC. Xu et al. examined 17 patients with pancreatic and 19 patients with extrapancreatic NETs finding no significant change in bFGF levels in best response or progressive diseases patients. However, lower baseline levels of bFGF were significantly associated with prolonged PFS rising from 16.7 to 21.15 months [94].
Quality AssessmentThe methodological quality assessment and risk of bias were divided into two groups, using CASP checklists for RCTs [
Comments (0)