In this study of women aged 40 years and older living in Mombasa, Kenya, we found that most women, regardless of HIV status, had inadequate medical coverage and faced financial insecurity. SVI-Kenya scores did not differ significantly by HIV status. While we found significant differences in CFS between HIV status groups, the small difference (i.e., a 0.4-point higher mean CFS among WWH) may not be clinically meaningful. The SVI-Kenya was not associated with age but was positively associated with WHODAS score, never being married, and a history of sex work.
While we hypothesized that older WWH would have increased social vulnerability compared to HIV-negative women, the SVI-Kenya scores and most responses were very similar in the two groups. Although WWH reported that they were less likely to interact with family members regularly, this difference was not statistically significant after p-values were adjusted for false discovery rate. The social isolation that some older individuals with HIV face, even from family members, is well documented in the literature (23, 24), although many studies include no control group in contrast to this analysis. The relationship between social determinants and HIV status in African settings is not clearcut, with at least one publication demonstrating an inverse relationship between poverty and HIV status (25). It is possible that a social inventory such as the SVI-Kenya may not capture the social determinants of health that correlate most closely with prevalent HIV in older adults. Of interest, we excluded marital status from the SVI-Kenya, despite it being included in the original SVI, because married women often live separately from their husbands in Kenya for economic reasons. Instead, we asked whether women lived alone (17). We found in our exploratory analysis that women who had never married (i.e., single women) had significantly higher SVI-Kenya scores than women who had ever married (i.e., married, separated, divorced, or widowed women). Because WWH were more likely to have never married, including marital status in our SVI-Kenya score could potentially have increased the disparity in SVI-Kenya scores between WWH and their HIV-negative counterparts.
The association we found between SVI-Kenya and WHODAS may be in part due to some overlap in concepts between SVI-Kenya items and three domains of the WHODAS— namely participation, life activities and getting along. However, while the SVI-Kenya focuses on an individual’s social situation in general, the WHODAS specifically asks individuals to reflect upon difficulties they have experienced in the past 30 days due to health conditions, including “diseases or illnesses, other health problems that may be short or long lasting, injuries, mental or emotional problems, and problems with alcohol or drugs.” For example, while the SVI questions ask, “Do you participate in any social groups, such as ‘merry-go-rounds’?” (i.e., a social group that helps members save money), and “How often do you attend religious services?” without reference to physical health, the WHODAS asks whether an individual has had difficulty performing activities such as maintaining friendships or joining in community activities as a result of their health conditions. In addition, the SVI-Kenya captures information on aspects of social support, perceived safety and financial security that are unrelated to items in the WHODAS. These two measures focus on different constructs and were only associated in our regression analyses after adjustment for potential confounders.
While both older age and higher SVI-Kenya score were associated with higher WHODAS score, it was interesting that women recruited from the Mombasa Cohort had lower WHODAS scores, after adjustment for age and SVI-Kenya score. This may reflect selection bias, with women who continue participating in the Mombasa Cohort being generally healthier than the women we recruited from the general population, who were also older on average and required more assistance with transportation to the clinic. Alternatively, the availability of regular outpatient care to members of the Mombasa Cohort at no cost may contribute to their lower disability scores. During the initial phase of COVID-19 lockdowns in Kenya, the Mombasa Cohort was permitted to continue visits, since it was seen as an important source of healthcare for its participants. As COVID restrictions relaxed, we recruited women from the community using outreach at local health centers and through word-of-mouth. This change in recruitment method or the difference in timing since onset of the COVID pandemic may have also contributed to the enrolment of women with higher mean WHODAS scores (45.2 for the general population vs. 30.7 for the Mombasa Cohort) on average.
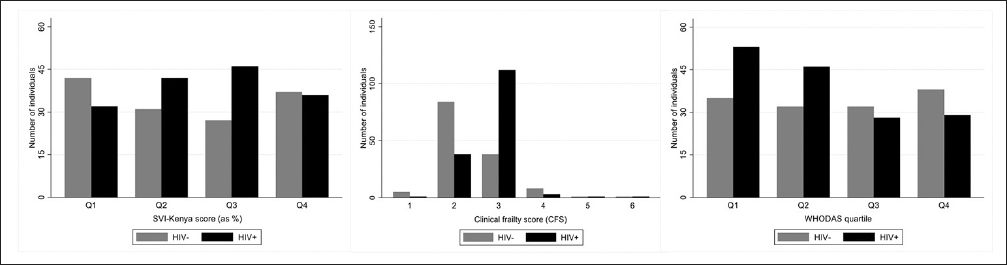
We found no relationship between the CFS, a clinician-assessed measure of the physical frailty phenotype, and the SVI-Kenya, which uses a deficit accumulation approach to assess social vulnerability (15). This may be a function of conducting this study in an outpatient rather than a hospital setting and including many women who were still in their 40s and 50s (77.8% of the study population) and relatively healthy. While the CFS scores in this study ranged from 1 (“very fit”) to 6 (“moderately frail”), only 5.1% of the sample had CFS scores over the median, which was 3 (“managing well”). That said, SVI-Kenya scores in the most frail women were similar to those in the least frail (mean score 31.4 if CFS = 1 versus 28.8 if CFS = 6). A recent paper by Amieva et al. posits that social vulnerability may be more related to stably poor social status and unfavorable social conditions rather than to an ongoing process of decline (26), which supports our finding that social vulnerability is a distinct concept from physical frailty.
We did find that HIV, age, and their interaction were all associated with physical frailty in this sample. Of note, the CFS was assigned by clinicians who may have been aware of participants’ HIV status; in addition, women who have taken ART often have visible stigmata of lipoatrophy and lipodystrophy, which may represent side effects of earlier medication regimens or consequences of HIV itself, leading to higher scores. Consequently, the significant age-by-HIV-status interaction term as a predictor of CFS and the extrapolation of predicted CFS scores above the median in our graph should be interpreted with caution due to the paucity of CFS values in this range.
In the exploratory analysis of predictors of SVI score, we found that being single was associated with a higher SVI-Kenya score in this study population. Single women in this age group may have fewer social contacts or more constrained social support than women who have ever been married, regardless of whether their spouse is still with them, either due to having fewer children or to differences in social status in the community related to never having married (23). The higher SVI-Kenya scores among participants recruited from the Mombasa Cohort may reflect sex work stigma and be related to the increased risk of violence and HIV acquisition that current and former women who engage in sex work in Kenya face (27, 28). Although women recruited from the Mombasa Cohort were nearly a decade younger, on average, than women recruited from in the general population, the SVI-Kenya score was not associated with age in this study. A more detailed analysis of egocentric social networks among this study population is underway and may further elucidate differences in social vulnerability between women with different HIV status, marital status and sex work histories.
The question of whether the SVI-Kenya also holds prognostic value in predicting future adverse health outcomes is one that our current cross-sectional study design was not designed to answer. Prior work using the original SVI inventory in a Honolulu-based cohort of older Japanese American men showed that higher SVI scores predicted cognitive decline and mortality, even among individuals who scored low on physical frailty measures (13, 29). Similar findings have been noted in work done among older individuals in several European nations (13, 15, 29, 30). Applying the SVI-Kenya in prospective cohort studies of older adults in Kenya and similar settings in sub-Saharan Africa could help determine how social vulnerability predicts health outcomes in resource-limited settings. Interestingly, a recent study in Tanzania derived an SVI for the Tanzanian context from existing cohort data for 235 individuals with a mean age of 75.2 years (14). In contrast to the Honolulu-based study’s findings, the association between the Tanzanian SVI and mortality lost significance after controlling for a frailty index that included measures of physical frailty (14). The adapted SVI used in the Tanzanian study differs from the SVI-Kenya in several ways. First, demographic factors (e.g., education, marital status) are included in the adapted SVI used in Tanzania, whereas we chose to capture these factors as sociodemographic variables rather include them in the SVI-Kenya index. Second, the SVI-Kenya captures elements of personal safety and social interactions in a more detailed manner than in the adapted SVI used in Tanzania. Consequently, further prospective work on our index is needed to assess how it will perform with regards to longitudinal outcomes and whether it or the adapted SVI used in Tanzania performs better.
Our study supports the SVI-Kenya as a measure that captures information on social vulnerability that is distinct from measures of physical frailty and from age. In fact, the importance of social factors in Kenyan society, such as attending social groups and having children available for support as one ages, arose in our qualitative work as something that older women often lack, regardless of HIV status (17). While we were unable to assess longitudinal outcomes in this cross-sectional study, the factors associated with increased social vulnerability that could be a focus of targeted interventions to decrease social vulnerability, including for women who never married and those with a history of sex work. Such interventions to increase the strength and depth of social support may be most effective when delivered before physical frailty or significant disability occurs, at an age closer to those of the women in our study.
We acknowledge several limitations of this study. First, recruitment was initially constrained to Mombasa Cohort participants early in the COVID pandemic, a group that was likely skewed towards healthy women since they were able to attend a research clinic at that time. When we broadened recruitment from the cohort to the general population, our community outreach likely reached women who were more socially connected. These sources of bias limit the generalizability of our findings. Future work to reach older women with greater degrees of social vulnerability may require different recruitment approaches, such as using lists of elders known to live in a given community or doing house-to-house surveys. Second, the study is cross-sectional and as such, cannot identify temporal sequence or causal relationships. Finally, there were significant differences in participants recruited from the Mombasa Cohort and those recruited from the general population. Although we attempted to mitigate these differences by controlling for source of recruitment in our models, unmeasured differences may result in residual confounding of the relationships found.



Comments (0)