
Remember me





An observational case–control study was conducted with patients diagnosed with sciatica due to LDH and individuals of similar age, sex, and Body Mass Index (BMI) without the condition. The study was conducted at Valme University Hospital (Área de Gestión Sanitaria Sur de Sevilla) and the Clinical Podiatry Area of the University of Seville, Spain, between March 2022 and May 2024. The study was approved by the Clinical Research Ethics Committee of Valme University Hospital (Code 2449-N-21). All patients voluntarily participated but were informed of the study details and potential risks and provided signed informed consent.
The inclusion criteria were a diagnosis of chronic (three months minimum duration) radicular low back pain (sciatica) with a minimum score of 5 using the Numeric Pain Rating Scale 11 (NPRS-11) caused by non-traumatic LDH. Patients with other spinal pathologies causing radicular pain, conditions affecting walking (e.g., neuromusculoskeletal, vestibular, and cardiopulmonary diseases), neuropathic pain related to diabetes or other conditions, pregnancy, cognitive impairment, prior foot surgery, inflammatory rheumatic disease, use of walking aids, or current foot orthoses were excluded.
The control group included healthy individuals with similar demographics but without sciatica, LDH, lumbar pathology, trauma, surgery, musculoskeletal or neurological diseases, diabetes, or foot deformities. These individuals were companions of patients attending the Clinical Podiatry Area.
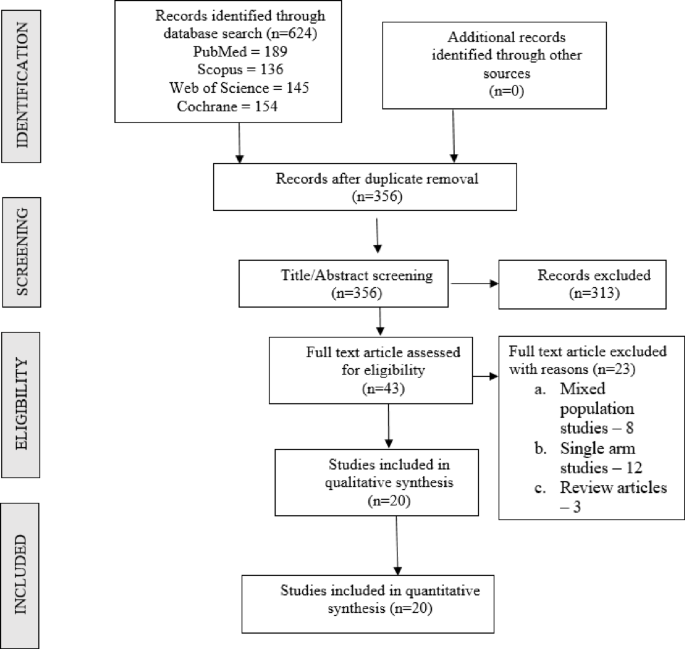
Patients were recruited by two clinicians specializing in Anesthesiology, Resuscitation, and Pain Management. Eligible patients were invited to participate and were referred to the Clinical Podiatry Area at the University of Seville for data collection. (Fig. 1). The examinations were always conducted in the morning between 10:00 and 13:00 a.m. The pharmacological treatment was not altered so as not to interfere with the results. Clinical and demographic data, including age, sex, weight, and height, were collected. Pain in the foot, lower limb, or lower back was recorded and quantified using the Numeric Pain Rating Scale 11 (NPRS-11). Disability was assessed using the Oswestry Disability Index (ODI), Manchester Foot Pain and Disability Index (MFPDI), and the SF-12 quality of life questionnaire.
Fig. 1
Image of the study laboratory
The foot joint range of motion was measured, including ankle dorsiflexion (knee extended and flexed), hindfoot and forefoot pronation and supination, first ray dorsiflexion and plantarflexion, and first toe dorsiflexion. Extrinsic foot muscle strength (dorsiflexors, plantarflexors, supinators, pronators) was evaluated using manual muscle testing, graded per the Medical Research Council classification (0–5 scale) [19], which assigns values between 0 and 5, where 0 represents no muscle activity and 5 represents normal muscle strength. The foot posture was assessed using the Foot Posture Index (FPI), a clinical tool, and the foot was classified as neutral, pronated, or supinated.
Plantar pressure examination during gait was performed using the FootScan platform®(RSscan International, Olen, Bélgica), which has been proven to have good reliability and repeatability [20]. The platform dimensions were 2093 × 469 × 18 mm, with 16,384 resistive sensors arranged in a 256 × 64 matrix with a resolution of 4 sensors/cm², an active sensor area of 1950 mm × 325 mm, data acquisition frequency of 125 Hz, and pressure range of 1–200 N/cm². The platform was embedded flush with the ground on a 2-meter-wide by 10-meter-long wooden walkway to simulate walking on a regular, even surface and to prevent the targeting effect. Following the manufacturer’s instructions, the system was calibrated before each data collection. During calibration, the participant’s body weight and foot size were entered into the software, and then the participant was asked to walk over the platform. The analysis software then determined the recalibration factor for future measurements for the same participant.
The platform is connected to a computer that transmits and processes all information using the Scientific FootScan® software. This system provides plantar pressure data by automatically dividing the foot image into 10 zones: medial heel (MH), lateral heel (LH), midfoot (MF), first metatarsal (M1), second metatarsal (M2), third metatarsal (M3), fourth metatarsal (M4), fifth metatarsal (M5), big toe (T1), and lesser toes (T2-5). For statistical analysis, the following plantar pressure variables were selected for each of these 10 zones: contact time (ms), mean pressure during total contact time (N/cm²), peak pressure (N/cm²), and time of peak pressure occurrence (% of the stance phase). These values were examined across the 3 functional rockers of the stance phase: [21] heel contact to forefoot contact (first rocker), forefoot contact to heel lift-off (second rocker), and heel lift-off to toe-off (third rocker). In addition, the foot-progression angle was also considered. In total, 121 parameters were recorded for each foot (4 variables x 10 zones x 3 rockers + foot progression angle).
Participants walked on the platform for 2 min at a comfortable speed for acclimatization. Data were then collected for five passages over the platform. The three most consistent footprints for each foot (complete footprints, heel-strike pattern, no adjustments) were selected by two experienced researchers. The average values of the pressure variables were used in the statistical analysis.
The variable mean pressure was taken as a reference, and the sample size was calculated to compare two means. The formula used is as follows:
Here, s is the estimated standard deviation, α is the type I error, β is the type II error, and d is the minimum detectable difference.
Thus, the final equation is as follows:
$$\begin n = \frac}} + )}^2}}}}} \hfill \\= \frac \cdot \:} + })}^2}}}}}^2}}} \hfill \\= } \approx \:41 \hfill \\ \end$$
A minimum of 41 cases per group was required to perform a comparison meeting these criteria.
In this study, the unit of analysis was the foot, rather than the individual participants. In the control group, both feet were analyzed to determine the sample size required for statistical comparisons. However, in the sciatica group, only the affected limb was considered. Because plantar pressure variables were the primary outcome measures, the non-affected limb was excluded from the analysis to avoid potential bias.This decision was based on the premise that compensatory biomechanical and antalgic adaptation could alter the kinetics and kinematics of the unaffected foot during the gait cycle, potentially confounding the interpretation of results.
Data analysisStatistical analysis was performed using IBM SPSS Statistics 27 (IBM, Armonk, NY, USA). For the descriptive analysis, absolute frequency (N), relative frequency (%), mean values, standard deviation (SD), 25th, 50th, and 75th percentiles, and interquartile ranges (IQR) were calculated. For the comparative analysis of qualitative variables, the chi-square test was used to determine whether there was any relationship (dependence) between the variables through cross-tabulations. To analyze the differences between the control and sciatica patient groups, normality tests were first performed using the Kolmogorov-Smirnov test. When the variable values followed a normal distribution, the independent samples T-test was used to compare the two groups; when the data did not follow a normal distribution, the Mann-Whitney U test for independent samples was used. For the inferential analysis, a 95% confidence level was considered by comparing the experimental p-value with a 5% significance level.
Comments (0)