
Remember me






The target population for the MHLS, conducted as a part of the FHMS, consisted of 211,615 residents of any age in the fiscal year (FY) 2012 who lived in the nationally designated Evacuation Order Zone (FY 2012 survey period from 7 February 2013 to 31 October 2013). This zone included 13 municipalities: Hirono Town, Naraha Town, Tomioka Town, Kawauchi Village, Okuma Town, Futaba Town, Namie Town, Katsurao Village, Iitate Village, Minamisoma City, Tamura City, Kawamata Town, and parts of Date City specifically recommended for evacuation [7]. The survey was conducted annually by mail to the 211,615 residents who registered as original residents in the areas designated as the Evacuation Order Zone as of April 1, 2012, even if they had moved out of these areas. Furthermore, the survey included those who were newly registered as residents in the above-mentioned zones after April 1, 2012 [7].
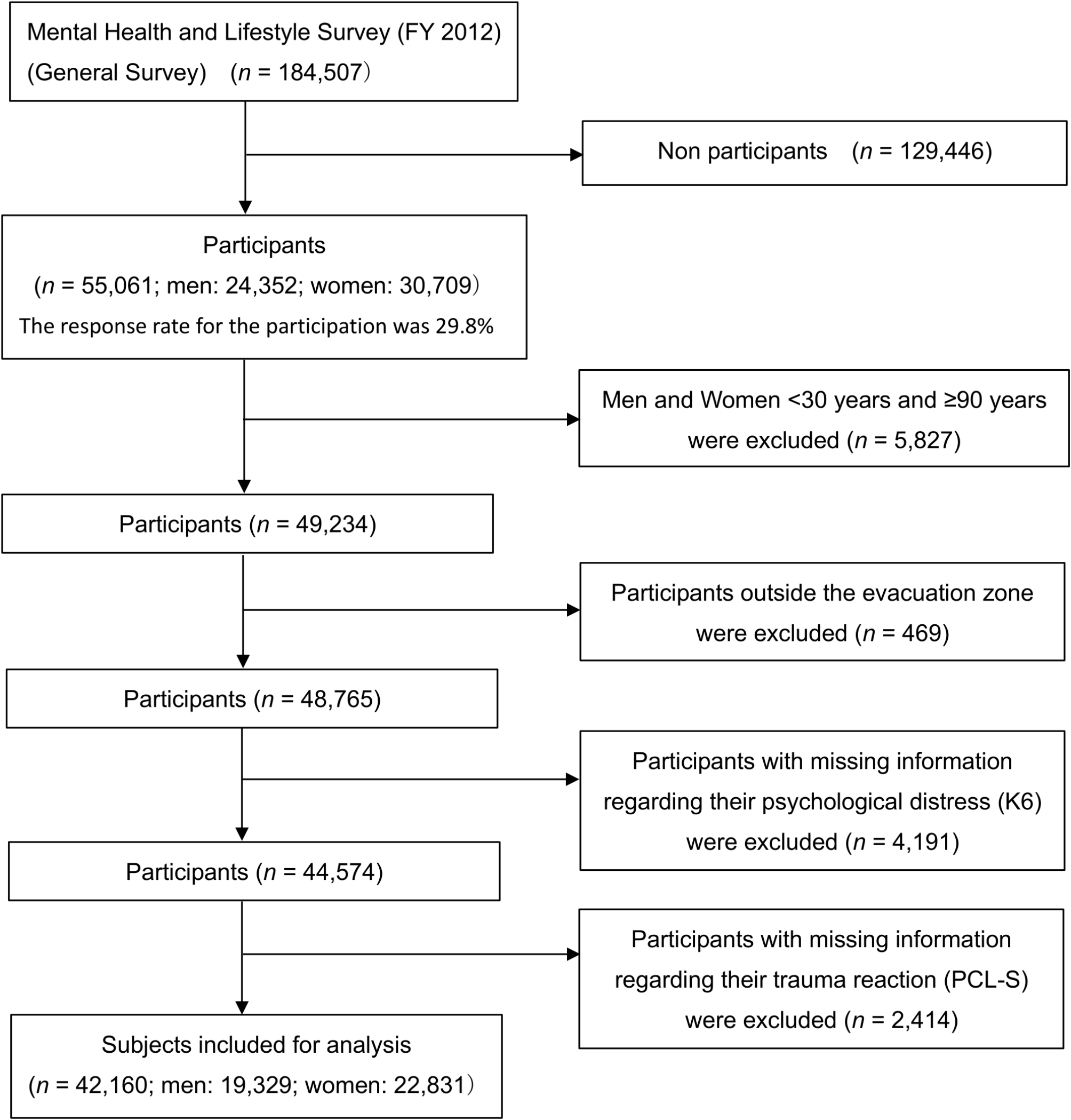
In this study, the mental health status of the participants was measured using the Kessler Psychological Distress Scale (K6) and the PTSD Checklist―Stressor-Specific Version (PCL-S) [9]. Figure 1 depicts the selection process for the subjects in this study. Of the 211,615 residents, 184,507 were targeted for the general survey (aged 15 years or older), of which 55,061 responded (response rate: 29.8%).
Fig. 1
Flowchart of participant selection for this study two years after the Great East Japan Earthquake
To ensure the study’s focus on specific age groups, individuals younger than 30 years and those aged 90 years or older were excluded from the analysis (n = 5,827). Participants who resided outside the evacuation zone (n = 469) were also excluded. Additionally, individuals with missing information about psychological distress (K6; n = 4,191) and the reaction to trauma (PCL; n = 2,414) were excluded from the study. Finally, a total of 42,160 participants (19,329 men and 22,831 women) were included in this study.
The participants’ evacuation status was determined based on the categories of living situations reported by the participants. In this study, there were six categories of living situations: “evacuation shelter,” “temporary housing,” “rental housing or apartment,” “a relative’s home,” “their own home,” and “others.” Participants who resided in the Evacuation Order Zone, where the entire area of municipalities was designated for evacuation, were classified as evacuees. Participants living in the Evacuation Order Zone where only part of the town or village was designated were considered evacuees if they were currently residing in or had previously lived in either an “evacuation shelter” or “temporary housing.” Participants who did not meet these criteria were classified as non-evacuees.
Participants who returned the self-administered questionnaire were deemed to have provided their consent to participate in the study. The study protocol was approved by the Ethics Review Committee of Fukushima Medical University (approval numbers: 1316, 2148, and 2020239).
Dietary intake assessmentThe food frequency questionnaire (FFQ) was used to assess dietary intake. The FFQ used in this study was a modified version of the FFQ previously used in the Hiroshima/Nagasaki Life Span Study [9]. The FFQ consisted of 19 items, which were divided into 12 food groups: rice, bread, fish (sashimi, grilled/boiled/fried fish), meat (chicken, beef, pork, ham, sausages), green and yellow vegetables, light-colored vegetables, vegetable juice, fruits, fruit juice, soybean products (natto, miso soup, tofu dishes, boiled bean dishes, soy milk), milk, and dairy products (yogurt and lactobacillus drinks).
Participants were asked about the average number of times per week that they consumed each of the 12 food groups during the previous several days. The response options included “none,” “less than once per week,” “once or twice per week,” “3 or 4 times per week,” “5 or 6 times per week,” and “every day.” In this study, a frequency of “5 or 6 times per week” for each of the 12 food groups was considered high-frequency intake. The modified FFQ used in this study has been previously validated [14].
As mentioned earlier, 42,160 participants (19,329 men and 22,831 women) were included in this study. Among them, further exclusions were made for individuals who did not provide their responses regarding their food intake frequency, leaving a final sample size ranging from 37,833 to 41,554 participants.
Mental health status assessmentTo assess the participants’ mental health status, the aforementioned K6 scale and PCL-S were used. In the K6 scale, participants were asked about their experience of various symptoms over the past 30 days: “feeling so sad that nothing could cheer you up,” “feeling nervous,” “hopeless,” “restless or fidgety,” “feeling everything was an effort,” and “feeling worthless.” Each question was scored on a 5-point Likert scale, ranging from 0 (none of the time) to 4 (all of the time), with higher scores indicating a worse mental health status. The Japanese version of the K6 scale has been validated [15, 16]. In this study, nonspecific psychological distress was defined as having a score of 13 or higher on the K6 scale.
PCL-S was used to assess the current traumatic symptoms related to the experience of the Great East Japan Earthquake. This self-report measure consists of 17 Likert items designed to detect symptoms of PTSD. Participants rated each item on a scale of 1–5 (not at all, a little bit, moderately, quite a bit, or extremely). The Japanese version of the PCL-S has been validated [17, 18]. In this study, participants were classified as having probable PTSD if their total score on the PCL-S was 44 or higher [19].
Statistical analysisThe health status and food intake frequency for each food group were compared between evacuees and non-evacuees, as well as between men and women, using χ2 tests. Multivariable-adjusted logistic regression analysis was then used to investigate the association between high-frequency consumption of certain foods and psychological distress, as indicated by estimated odds ratios (ORs) and 95% confidence intervals (CIs). Model 1 of the logistic regression analysis was adjusted for age, sex, and presence or absence of evacuation. Model 2 included the variables from Model 1, as well as current smoking, current drinking, exercise habit, unemployed, and educational attainment (University/graduate school). These variables were selected as covariates based on their potential influence on psychological stress. For all statistical analyses, a significance level of 0.05 (two-tailed) was used. The SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC, USA) was used to conduct the statistical analyses.
Comments (0)