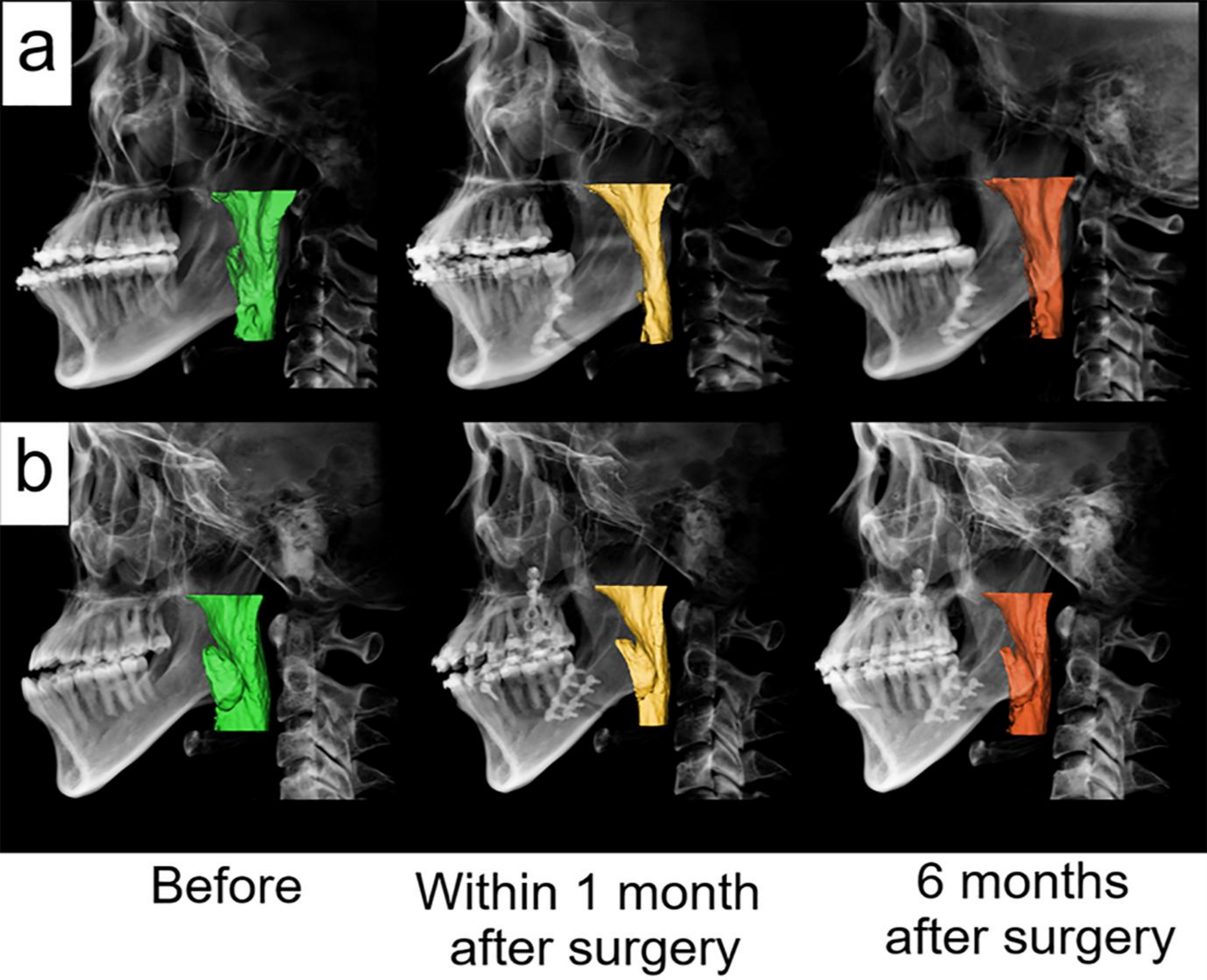
Previously, surgical wafers fabricated by conventional methods and 3D printing were compared using radiographic data of pre- and postoperative maxillary positions [1, 3, 8, 15, 19, 20]. However, postoperative outcomes were significantly influenced by intraoperative surgical factors. Since the positioning of the maxilla with intermediate wafers is highly dependent on the manipulation of the maxillomandibular complex and condylar position, it is essential to isolate surgeon-related factors to accurately assess the effectiveness of intermediate wafers. Additionally, intraoperative adjustments to the wafers relative to the dentition and forces applied during maxillomandibular fixation can interfere with the accurate reflection of preoperative plans recorded to the wafers. Moreover, the process of adapting screws and plates may further distort the final position of the maxilla.
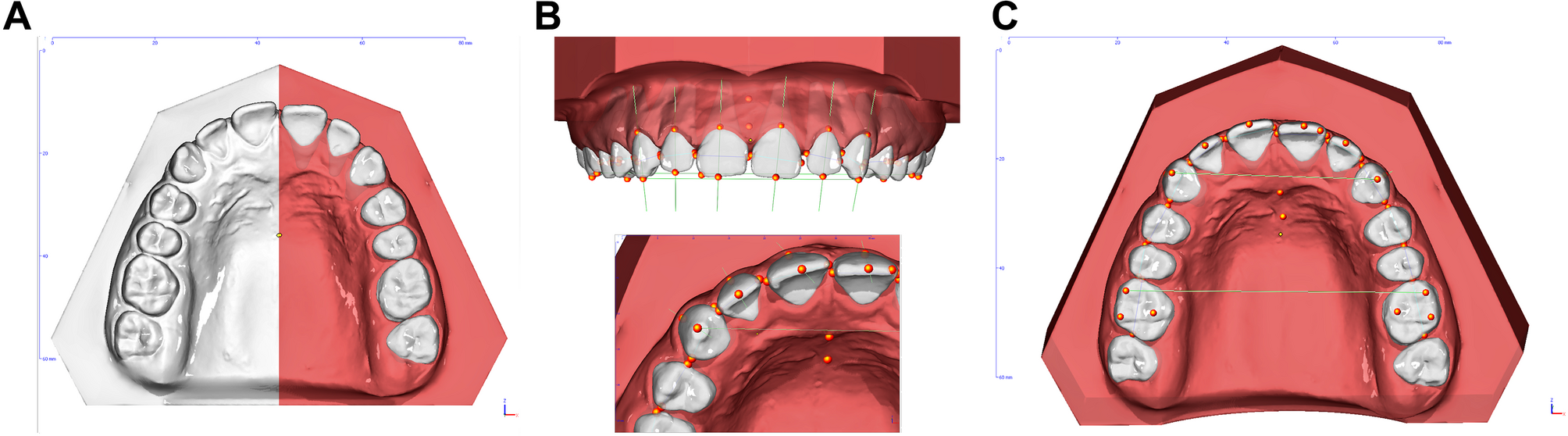
To address this, additional steps—including remounting, scanning, and subsequent superimposition—were introduced to mimic maxillary repositioning in orthognathic surgery, thereby eliminating intraoperative influences. Additionally, for each patient, we conducted both MMS and VMS, allowing us to assess two types of surgical wafers simultaneously, which is another advantage of this simulation [3, 8, 19, 20]. Through these steps, we were able to simulate the actual adaptation of wafers and analyze their influence on surgical outcomes, not measuring the thickness of the wafers.
Significant differences were observed across all three 3D coordinate axes of the maxillary position between CW and 3DW. While no significant differences between 3DW and VMS were observed, positional errors in all three directions were associated with CW compared with VMS. As hypothesized, CW fabrication following MMS was more prone to errors. During the preoperative planning for maxillary movement in orthognathic surgery, both planar movements and rotational movements (e.g., roll, pitch, and yaw) were considered. These rotational movements of the maxilla are challenging to reproduce during MMS, potentially leading to greater positional errors. Our results indicated significant differences in the transverse coordinates for roll and the vertical coordinates for pitch movement. Additionally, the presence of yaw in surgical planning increased the likelihood of positional errors in all coordinates. Yaw movement requires a high level of expertise for accurate maxillary cast repositioning, as it involves simultaneous adjustments in the transverse and anteroposterior coordinates while maintaining vertical coordinates during the manual manipulation of the maxillary cast. Furthermore, yaw adjustment in MMS is particularly challenging due to the absence of a consistent reference point, requiring reliance on reference lines that are difficult to digitize. Currently, devices used in MMS are primarily designed to measure the height of reference points. This limitation likely contributes to the increased potential for errors associated with the presence of yaw movements. However, the correlation between the extent of the movement and the errors was not identified. To consolidate the findings and achieve more credible results, a larger sample size is needed.
Other studies have also supported the accuracy of 3D methods in orthognathic surgery. One study demonstrated that 3D virtual computer-assisted planning offers higher accuracy compared to traditional methods like facebow transfer [9]. Another study investigated the accuracy of digitally fabricated intermediate wafers and found that the surgical outcomes were statistically insignificant from the planned maxillary movement in three dimensions [22]. In a randomized controlled study comparing digital and conventional resin wafers, digital wafers showed superior outcomes in transferring the surgical plan to the operation environment Additionally, a study comparing the validity of 3D-printed wafers and CW demonstrated that 3D-printed wafers is acceptably accurate in three spatial dimensions, in both laboratory and clinical settings [23]. Reported errors from other studies during the laboratory steps of VMS and 3DW ranged from 0.03 to 1.4 mm [6] and from 0 to 0.35 mm, respectively [10].
MMS has traditionally been the standard method for fabricating intermediate wafers. Despite efforts to enhance the accuracy of dental cast movement in MMS [4,5,6,7, 24, 25], manual manipulation during model surgery still results in three-dimensional inaccuracies. Technical errors may also arise during impression-taking, facebow transfer, and the mounting process [1, 8, 9]. Improper dental impressions can reduce the fit of wafers to dentition, which in turn deteriorates the accuracy of maxillary repositioning. Additionally, errors during the facebow transfer can lead to an incorrect Frankfort Horizontal plane orientation. Consequently, the three-dimensional coordinates of the maxillary cast may differ from those oriented in VMS. Moreover, the three-dimensional movement of the maxillary cast during MMS is highly dependent on the operator’s expertise. Reference lines for the maxillary movement, illustrated on the cast, inherently possess human errors and are challenging to accurately align with the three-dimensional axes set by the Frankfort Horizontal plane. Since 3D fabrication of wafers is directly accomplished from VMS, several steps prone to technical errors are eliminated, except the superimposition process, which involves merging scan data from dental casts and CT scans, can be a major origin of the errors. A study demonstrated that five out of six directions of maxillary movement in the articulator exhibited errors exceeding 1 mm, with inaccuracies in midline repositioning leading to corresponding discrepancies in the mediolateral repositioning of the posterior section of the maxilla [5]. Manually repositioning the maxillary dental cast to the precise 3D location, especially in cases involving yaw, presents significant challenges for the operator. Furthermore, these complex laboratory procedures in MMS are not only time-consuming but also require considerable effort.
Several studies have reported on the accuracy of 3D virtual datasets generated through VMS and laser scanning techniques. However, potential errors during the acquisition of virtual datasets in VMS have also been noted [26,27,28]. Limitations of CT imaging, including inadequate noise levels, resolution, contrast, and image quality, hinder the establishment of a precise digital mounting method for VMS [13]. Furthermore, the slicing thickness of CT data may limit the accuracy of occlusal surface reconstruction, affecting the precision of reference points in the digital mounting process on programmed articulators and potentially introducing errors. Artifacts at the occlusal level of dentition in CT imaging further compromise the accuracy of occlusal and intercuspidation data.
Fully automated and point-based semi-automated superimposition technologies have been developed to merge scan data from dental casts and CT scans to enhance the resolution of dentition [29,30,31]. However, these technologies do not guarantee accuracy, particularly in cases involving orthodontic braces, which may be inadequately represented due to metal artifacts in CT scans. Therefore, manual adjustment of scanned dentition to align with CT-derived dentition is necessary, inherently introducing human errors even within digital processes. Additionally, errors may occur during the wafer fabrication process with 3D printers. Stereolithographic technology, which is still under development, can introduce errors due to dimensional changes in the resin from sequential curing and the removal of residual resin using alcohol [10].
The results of this study suggest that 3DW with VMS offers greater accuracy than CW with MMS, as confirmed by in vitro simulations that excluded intraoperative factors. 3DW facilitates more precise alignment of the maxilla as planned in VMS, particularly when rotational movements of the maxilla, such as yaw, roll, and pitch, are required in maxillary repositioning. The study demonstrates that manually reproducing the preoperatively planned maxillary position is considerably challenging. Therefore, it is recommended to directly fabricate surgical wafers using a 3D printer, as planned and designed through 3D imaging solutions, to achieve accuracy, despite potential technical errors arising from digital scanning, superimposition, and printing. It also reduces laboratory work and time for the operator, thereby decreasing overall effort. In the foreseeable future, advancements in 3D imaging software and 3D printing technology might enable VMS and 3D printing to entirely replace MMS. However, it must be noted that there are inherent errors originating from the 3D software. The errors from the scanning process of dental casts and the merging of scan data from dental casts and CT scans are inevitable. These errors may favor the results from 3DW, as the maxillary position set in VMS was used as a standard. Moreover, the costs associated with the laboratory setup for 3D software, printers, and scanning devices are significantly higher than those for CW. Even when virtual planning and 3D printing is outsourced to external laboratories, the expenses remain relatively higher. Additionally, the availability of 3D solutions can vary greatly depending on the region.
This study isolated surgical factors that influence maxillary repositioning and mimicked the relocation process in vitro, similar to Le Fort I osteotomy. However, a larger sample size is necessary for a thorough analysis of the factors contributing to inaccuracies in wafer fabrication. Furthermore, it is important to acknowledge that more skilled technicians may enhance the accuracy of MMS. Depending on the expertise of the MMS operator, the gap between CW and 3DW may not be significant. Particularly in cases involving complex movements of the maxilla, such as rotational movements, the likelihood of errors may greatly depend on the operator’s experience. Therefore, conducting a study to compare outcomes from various MMS operators is crucial to quantify this influence. Additionally, the post-processing of 3D-printed wafers can result in varying levels of accuracy. It is also important to note that different types or brands of 3D printers and printing materials are reported to have varying accuracies [21, 32]. Recently, the accuracy of intraoral scanners has improved significantly. While we utilized a laboratory model scanning device, direct dentition scanning from patients could simplify the preoperative work-up for orthognathic surgery by eliminating the need for dental impressions. However, current complete-arch scanning with intraoral scanners is reported to be insufficiently accurate for fixed appliances [33,34,35]. The impact of this limitation on the fabrication of wafers and maxillary repositioning in orthognathic surgery should be investigated in future studies. Furthermore, newer acquisition technologies may enhance accuracy and improve these outcomes [35].








Comments (0)