Study design and population
This study drew data from the baseline wave (conducted from 2014 to 2017) of the China Hainan Centenarian Cohort Study (CHCCS), which collected all centenarians and a representative sample of individuals who were 80–100 in Hainan province. Being the southernmost province of China, Hainan has the highest percentage (20.52/100,000) of centenarians among all Chinese provinces [23, 24]. The survey contained extensive information on respondents’ demographic and socioeconomic statuses, health and health services utilization, LTC needs and the types of long-term needs they received.
A complete sampling for centenarians was conducted according to the household registration data provided by the Civil Affairs Bureau. We dropped centenarians who declined to participate, were unable to participate due to dementia or paralysis, did not meet the age verification, died before the interview and participants with more than 25% missing data. For the respondents who were 80–99 years old, stratified random sampling was adopted by age, gender, geographic location and population density. 1,798 oldest old individuals were recruited into this survey. We dropped 153 individuals with missing data for the variables included in the regressions. Among the 1,645 respondents who were available with complete information, 201 individuals neither reported a need for assistance in any ADL or IADL domains, nor did they indicate a need for assistance in performing daily activities in the self-reported question. In the end, we included the remaining 1,444 individuals who were in need of LTC in the analysis.
Information for each participant was collected from a self-reported questionnaire with a face-to-face interview, interdisciplinary examinations and a laboratory analysis. A detailed description of the sampling method and data collection process was documented in another study [25].
The ethics approval was from the Ethics committee of the Chinese People’s Liberation Army General Hospital (Beijing, China). All participants provided written informed consent before the information was collected.
Measurement of unmet needs for LTC
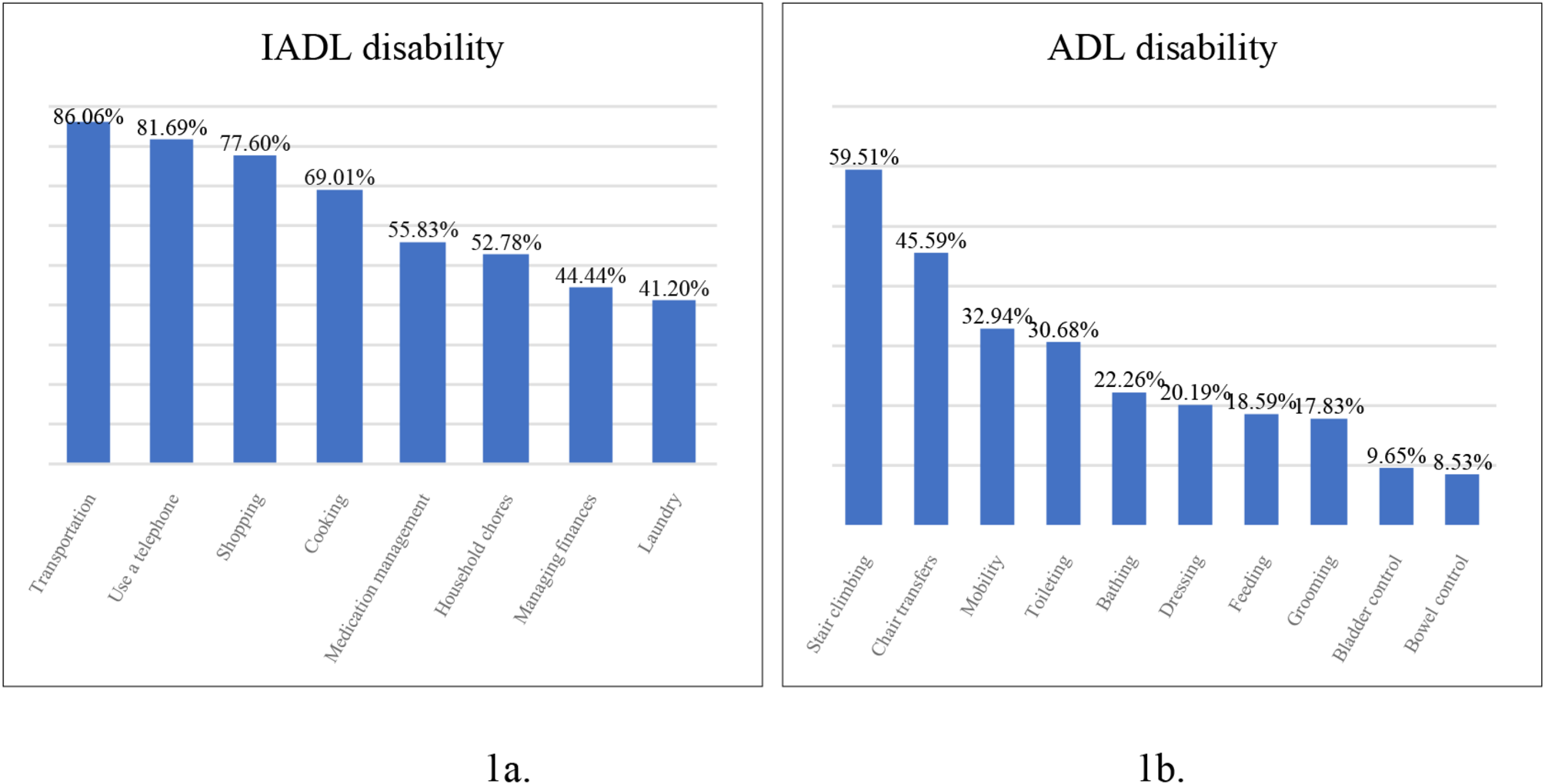
Unmet needs for LTC were the key interest in this study, which evaluated the gap between needs and provision for the LTC. To begin with, we identified individuals in need of LTC by employing Lawton’s Instrumental Activities of Daily Living (IADLs) [26] and Barthel’s Activities of Daily Living (ADLs) assessments [27]. These surveys encompass 8 IADL domains (such as using a telephone, doing laundry, household chores, cooking, shopping, transportation, managing finances, and medication management) and 10 ADLs (covering grooming, bathing, toileting, bowel and bladder control, dressing, feeding, stair climbing, chair transfer, and mobility on level surfaces). The respondent who self-reported a need for assistance in any of these ADL or IADL tasks was considered to have an LTC need. We excluded those who did not need any assistance in ADL or IADL tasks.
Subsequently, within the subset of the individuals who had LTC needs, we derived the dependent variable, denoting an indicator of unmet needs, from their self-reported responses to the question: “Do you require assistance for daily activities of daily living?” The response options included: (1) “I don’t need any assistance,” (2) “I need assistance, but no one provided it,” and (3) “I need assistance, and I received it.” We constructed a binary variable to indicate whether the individual had an unmet LTC need. Specifically, it was assigned the value 0 if the respondent selected answers 1) or 3), and the value 1 if the respondent chose the second answer to the question. This was an overall description of the current LTC situation self-reported by the respondents, and the answer did not indicate the provision of care for a specific ADL or IADL domain. Thus, we considered this was a general perceived unmet need.
Measurement of Health-related quality of life
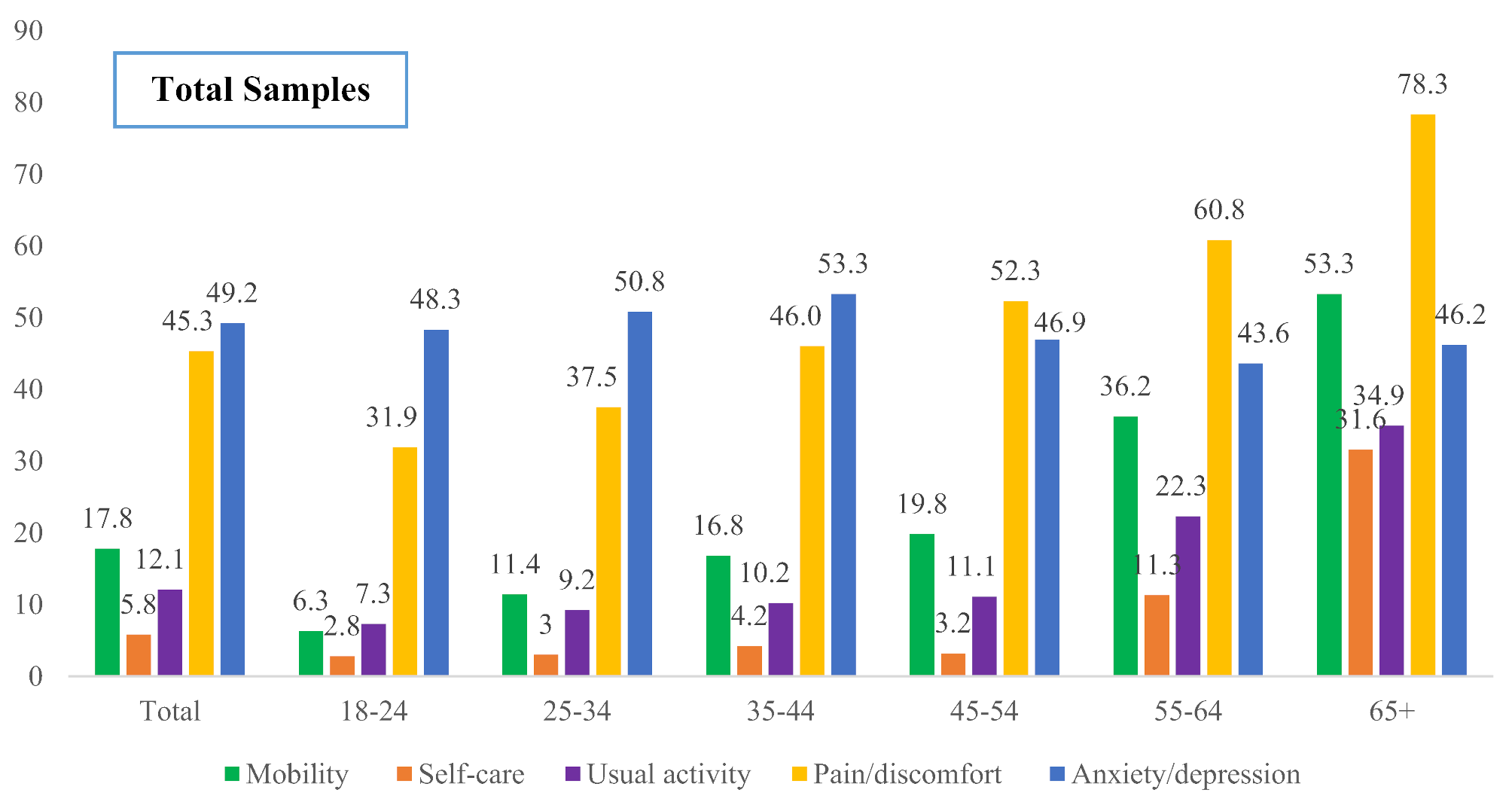
Health-related quality-adjusted life years (QALYs) were determined using the EQ-5D-3L questionnaire, which requires respondents to assess their current health across five domains: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In this questionnaire, each domain has three response levels: ‘1’ indicating no problems, ‘2’ indicating moderate problems, and ‘3’ suggesting severe problems. It is assumed that a response of ‘1’ across all domains correlates with a higher perceived quality of life, representing a state closer to perfect health. The QALY index, ranging from 0 (death) to 1 (perfect health), is calculated based on these responses, utilizing the Chinese Time-Trade-Off value set to represent health states quantitatively [28]. The QALYs ranged from 0 to 1, with 0 indicating death and 1 indicating perfect health. More detailed information on the calculation of QALYs of the oldest old population was described in another study [29].
Socio-demographic and health-related variables
Two groups of covariates included in the analyses were socio-demographic factors and health related variables. For socio-demographic variables, we investigated age, gender, rural-urban residency, education, marital status, the number of leisure activities, whether the respondent has a regular social and family contact. Age was considered a categorical variable in the statistical description (80–85, 86–95, 96–105, and > 105 years) and a continuous variable in the regression analysis. Gender was a binary variable with 1 indicating male and 0 indicating female. The dummy variable, illiterate, was constructed to reflect respondents’ educational attainment because more than half of the oldest-old respondents did not go to school at all during their school-age period. A dummy variable indicating rural-urban residency was generated directly from the related question. Marital status was categorized into three dummy variables: married, widowed and single. The number of leisure activities was determined from the questionnaire, where respondents were asked to select from more than 15 leisure activities (multiple choice), such as reading, playing cards, planting, having pets, social activities, etc. This variable was then treated as a continuous variable. Two binary variables were generated to indicate whether the respondent had regular contact with friends and family members to seek help each month.
A dummy variable indicating whether the individual was living alone was generated. To further investigate the living arrangements, we also further classified the individuals who were not living alone and constructed a set of binary variables, including living with children but not with the spouse, living with the spouse and children, living with the spouse but not with any child, living with grandchildren but not with the spouse or any child, living with other family members, and living in a nursing home.
For health-related variables, we included functional disabilities, number of drugs taken per day, vision impairment, hearing impairment, sleep quality, and sleep quality. ADL and IADL scores were calculated according to the responses to the questionnaires. IADL scores ranged from 0 to 8 with lower scores indicating higher dependency. An early warning of functional decline would be reflected by the IADL scale [30]. The ADL scores ranged from 0 to 100, with lower scores implying a higher level of disability. We generated two dummy variables indicating whether the respondent had IADL disability or ADL disability. If the respondent needed help in more than 6 domains in IADL or 3 domains in ADL, he/she would be classified as IADL disability or ADL disability respectively. Since the IADL and ADL were collinear, we did not include the IADL indicator in the regression. Number of drugs taken per day was generated as a continuous variable. Three dummy variables indicating the self-reported sleep quality were generated also according to the response to the questionnaire. Vision and hearing impairments were dummy variables indicating whether the respondent had any problem that affected daily life and cannot be corrected to a normal level.
Statistical analysis
We conducted both descriptive and Tobit regressions in this study. Firstly, mean values and standard deviations for continuous variables, numbers and percentages for categorical variables were presented by LTC status and for the whole sample. The significance of the differences between groups of LTC status was tested using t-tests for continuous variables and chi-squared tests for categorical variables. Secondly, we mapped out the prevalence of problems in each domain of ADLs and IADLs for the oldest old and centenarian population. Then, since QALYs ranged from 0 to 1 and censored at 1, we conducted Tobit regressions to analyze the association between unmet LTC needs and QALY score. Besides, to explore the relationship between unmet LTC needs and the five EQ-5D dimensions, we conducted Ordered Probit regressions, which were suitable for analyzing the levels of problems reported in the five EQ-5D dimensions. For the sensitivity analysis, the Propensity Score Matching (PSM) method, specifically using nearest neighbor matching with a caliper of 0.05, was utilized to align the group with unmet LTC needs and the group without, prior to conducting the regression analyses.

Comments (0)