Nocturnal enuresis (NE), particularly primary monosymptomatic nocturnal enuresis (PMNE), is a challenging condition with significant impacts on both patients and their families. The study aimed to evaluate the therapeutic efficacy and safety of combined transcranial and direct sacral magnetic stimulation in patients with PMNE. The findings shed light on potential avenues for managing this condition effectively.
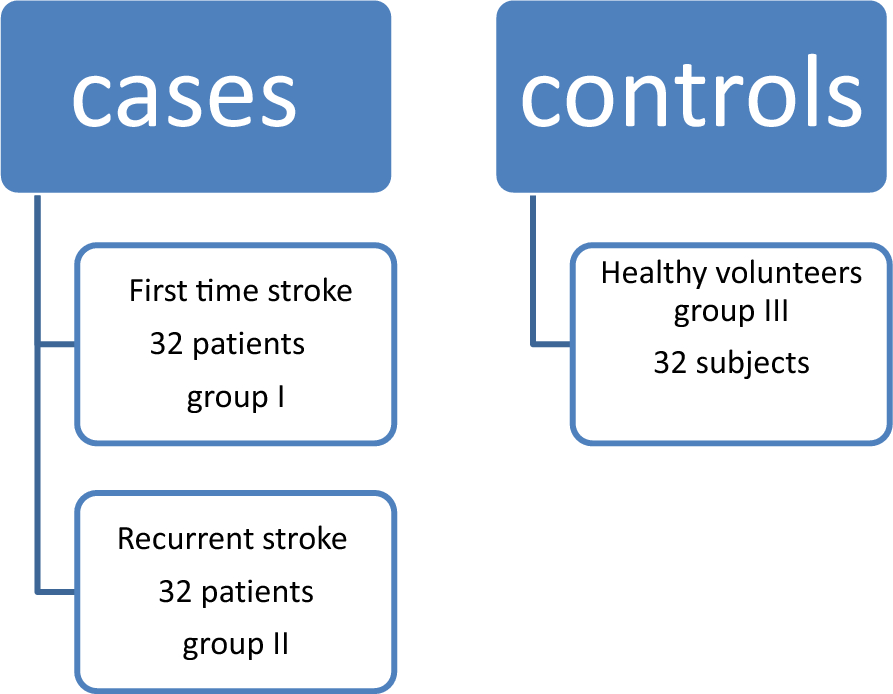
Two age and gender-matched groups were randomly assigned to undergo real magnetic stimulation (22 patients) or a control group (18 patients) that received sham stimulation. In compliance with safety recommendations, a suggested magnetic stimulation protocol is proposed to incorporate transcranial stimulation alongside the previously studied direct magnetic sacral root stimulation.
The complex etiological interplay of PMNE includes decreased arousal from full bladder during sleep because of brainstem enuresis impeding reflex maturational delay. In addition to disrupting the sleep–wake cycle, psychological issues are also taken into consideration [10].
Functional magnetic resonance imaging (fMRI) was utilized in a 2011 study by Du Lei to investigate how children with PMNE’s spontaneous brain activity changed during the resting state. They discovered that the left midbrain, medial frontal gyrus (Brodmann area, BA 10), and left inferior frontal gyrus showed significant abnormalities in children with PMNE [17].
Other investigations revealed the left medial orbital superior frontal gyrus (Frontal_Med_Orb_L) and an enhanced activity in the left superior occipital gyrus with the left thalamus serving as the seed. However, the PMNE group displayed a markedly reduced functional connection to this gyrus [18].
Based on these observations, the current study extends this literature by examining the combined effects of transcranial and sacral magnetic stimulation in PMNE, providing valuable insights into potential treatment modalities. This is corroborated by studies indicating the efficacy of magnetic stimulation in addressing urinary dysfunction. Patients with nocturnal enuresis are characterized by pathologically increased excitability and reduced inhibitory processing in the motor cortex, which may contribute to the pathogenesis of nocturnal enuresis, according to a 2015 study by Khedr and colleagues that investigated the cortical excitability of patients with PMNE. They discovered that patients with MNE had lower motor thresholds (resting and active) and shorter cortical silent periods, compared to healthy control subjects which denotes inhibitory mechanisms at the level of the motor cortex, probably mediated by gamma-aminobutyric acid (GABA)-B receptors [19].
Results from studies utilizing positron emission tomography (PET) scanning point to the most medial region of the primary motor cortex as the starting point for the voluntary motor pathways involved in pelvic floor control [20].
The noninvasive technique of repetitive transcranial magnetic stimulation (rTMS) is used to control the excitability of the human cerebral cortex. The modulatory effects on cortical excitability can vary depending on the stimulation paradigms, including frequency, intensity, duration, and total number of pulses. It is generally accepted that low-frequency (≤ 1 Hz) rTMS has an inhibitory influence on motor cortical excitability, while high-frequency (> 5 Hz) rTMS enhances it [21].
But the idea of “excitatory” versus “inhibitory” in rTMS should also be viewed as relative, because, instead of direct cortical excitation leading to a net result of inhibition, high-frequency stimulation may excite gamma-aminobutyric acid-mediated intracortical inhibition, and vice versa in a low-frequency stimulation [22].
Transcranial magnetic stimulation (TMS) has been used in numerous paradigms since 1998 to test various aspects of cortical excitability, according to Pascual-Leone, Alvaro. Cortical excitability can be persistently inhibited or facilitated, depending on rTMS parameters [23].
We noticed that patients with PMNE have a relatively high motor threshold. We employ a 3 Hz frequency stimulation stimulatory procedure. Our findings may differ from those of Khedr and colleagues (2015), who present an opposite observation. However, their investigation focused on patients who had previously been using drugs that could affect brain excitability; in this study, medications were ceased 3 months prior to the start of the study.
In addition, based on functional MRI studies, it was hypothesized that NE involves a complex interaction between various brain regions with intricate neuronal network dysfunctions that modify supraspinal control of voiding activity and cortical excitability. These dysfunctions may act directly on cortical neurons or indirectly through trans-synaptic intracortical neurons [10].
The final data supported our hypothesis by suggesting that a possible decline in MT correlated with a comparable improvement in both clinical and functional outcomes. Rather than cortical excitability, we propose a hypothesis of defective cortical regulation via neural networks, which we advise further investigation in a separate study linked with functional neuroimaging.
Urge incontinence and urine frequency were successfully treated with sacral roots magnetic stimulation, as demonstrated by numerous studies that investigated this topic [24]. The effectiveness of magnetic sacral root stimulation (SMS; 15 Hz with a total of 1500 pulses/session) for the treatment of monosymptomatic nocturnal enuresis was investigated in a double-blind, randomized clinical trial conducted by Khedr and colleagues in 2015. Real rSMS participants had a considerable reduction in the mean number of wet nights per week. One month after the treatment concluded, this improvement persisted. The quality of life of patients who received real-rSMS also showed improvements [3].
In another study investigated twenty girls with PNE and compared functional sacral magnetic stimulation to standard treatment modalities. The results showed a substantial reduction in the frequency of weekly PNE episodes following sacral stimulation when compared to placebo (P = 0.007) [25].
When compared to direct electrical stimulation, magnetic stimulation offers a more profound stimulation and is less painful, with minimal to no documented adverse effects. It may also be applied over clothing and is not linked to symptoms, such as diarrhea or abdominal pain [24].
The exact mechanism underlying rSMS is unknown. However, the predominant autonomic and somatic innervation of the urethra, vaginal wall, rectum, and pelvic floor muscles is provided by the roots of sacral nerves S2–S4. One effective technique to manage and alter the pelvic floor is to stimulate these roots [26, 27]. The effect of magnetic stimulation on micturition has been explained by a number of mechanisms, including: direct effect on the bladder wall and contraction of the pelvic floor muscles through the pudendal nerve’s efferent fibers [8, 27, 28]; activation of peripheral afferent fibers and evoking sensory input to the spinal cord, increasing the excitability of sensorimotor connections in the cord and cortex, which raises cortical arousal or improves inhibition of noradrenaline and serotonin reuptake; and finally, improving the excitability of the corticospinal tract, which promotes detrusor muscle contraction and/or relaxation of the urethral sphincter [29].
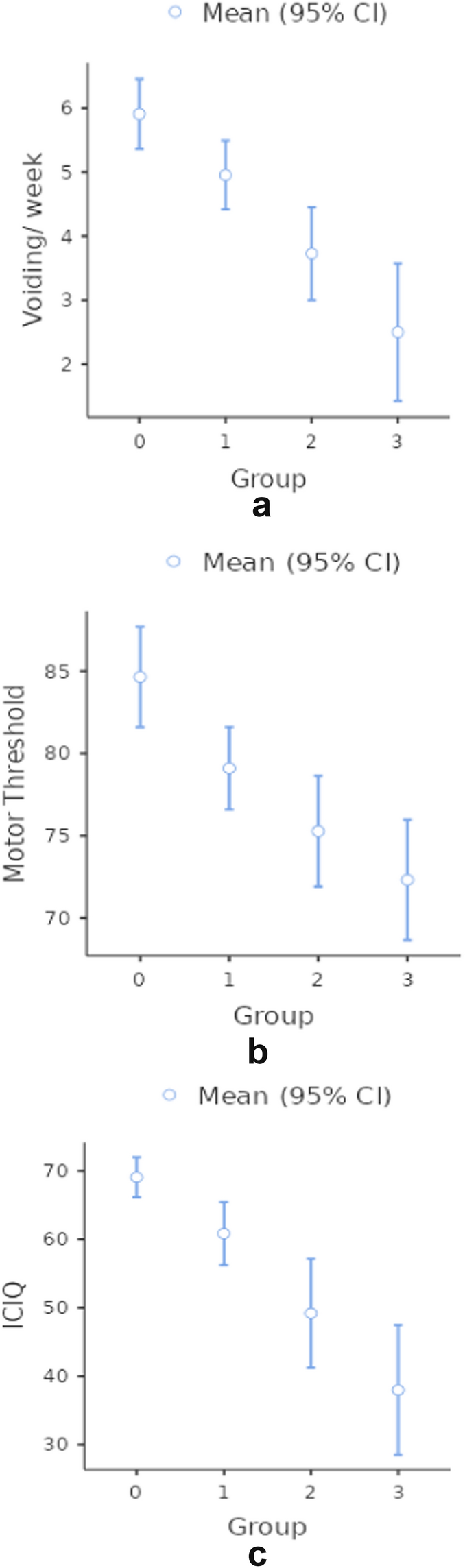
The study results demonstrate promising therapeutic efficacy, with a significant reduction in the frequency of wet nights observed in the real stimulation group compared to the sham group. This improvement was particularly pronounced after 1 month and sustained at the 3-month follow-up, indicating the long-term benefits achieved by the combined stimulation protocol.
Assessment of motor threshold (MT) revealed gradual change in cortical excitability in the treatment group, indicative of alterations in neuronal networks following magnetic stimulation. This supports the hypothesis that transcranial magnetic stimulation (TMS) can modulate brain activity, potentially influencing bladder control mechanisms. The sustained changes observed in MT over the follow-up period further underscore the durability of the treatment effects.
Using the ICIQ–LUTS qol score, the study additionally evaluated the influence on quality of life and found an associated improvement with clinical outcomes. The improvement that was seen immediately after the sessions was not statistically significant, but at the 1- and 3-month follow-ups, there were notable improvements. These results demonstrate the comprehensive advantages of the multimodal stimulation protocol, which improve general well-being in addition to decreasing episodes of enuresis. Response evaluation based on the ICCS criteria showed a higher response rate in the real stimulation group, with a greater proportion of patients achieving partial or complete response compared to the sham group.
Importantly, the safety assessment revealed no significant adverse effects associated with the magnetic stimulation protocol, reaffirming its safety profile in pediatric patients with MNE.
Limitations and future directions
While the study provides valuable insights into the therapeutic potential of combined magnetic stimulation, several limitations should be acknowledged. The sample size was relatively small, and the follow-up duration was limited to 3 months. Future studies with larger cohorts and longer follow-up periods are warranted to validate the findings and assess the durability of treatment effects. In addition, exploring the underlying mechanisms of magnetic stimulation on bladder control pathways could further enhance our understanding and optimize treatment strategies for PMNE. The combined transcranial and sacral stimulation protocol provides a durable sustained ameliorating effect for patients with PMNE; however, it is recommended to perform another study to compare the combined protocol with the pure sacral stimulation for the same parameters which is still lacking according to our knowledge.

Comments (0)