H. pylori eradication therapy has been established to prevent gastric cancer and other H. pylori-related diseases [15]. However, it also remains necessary to identify H. pylori-infected young people despite low infection rates and confirm the usefulness and safety of eradication therapy. To address this issue, we trialled H. pylori screening using a urinary anti-H. pylori antibody test in school health checkups for 11 years. Our findings revealed very high compliance to initial testing, several unique clinicopathological characteristics, and the effectiveness of H. pylori resistance-based treatment.
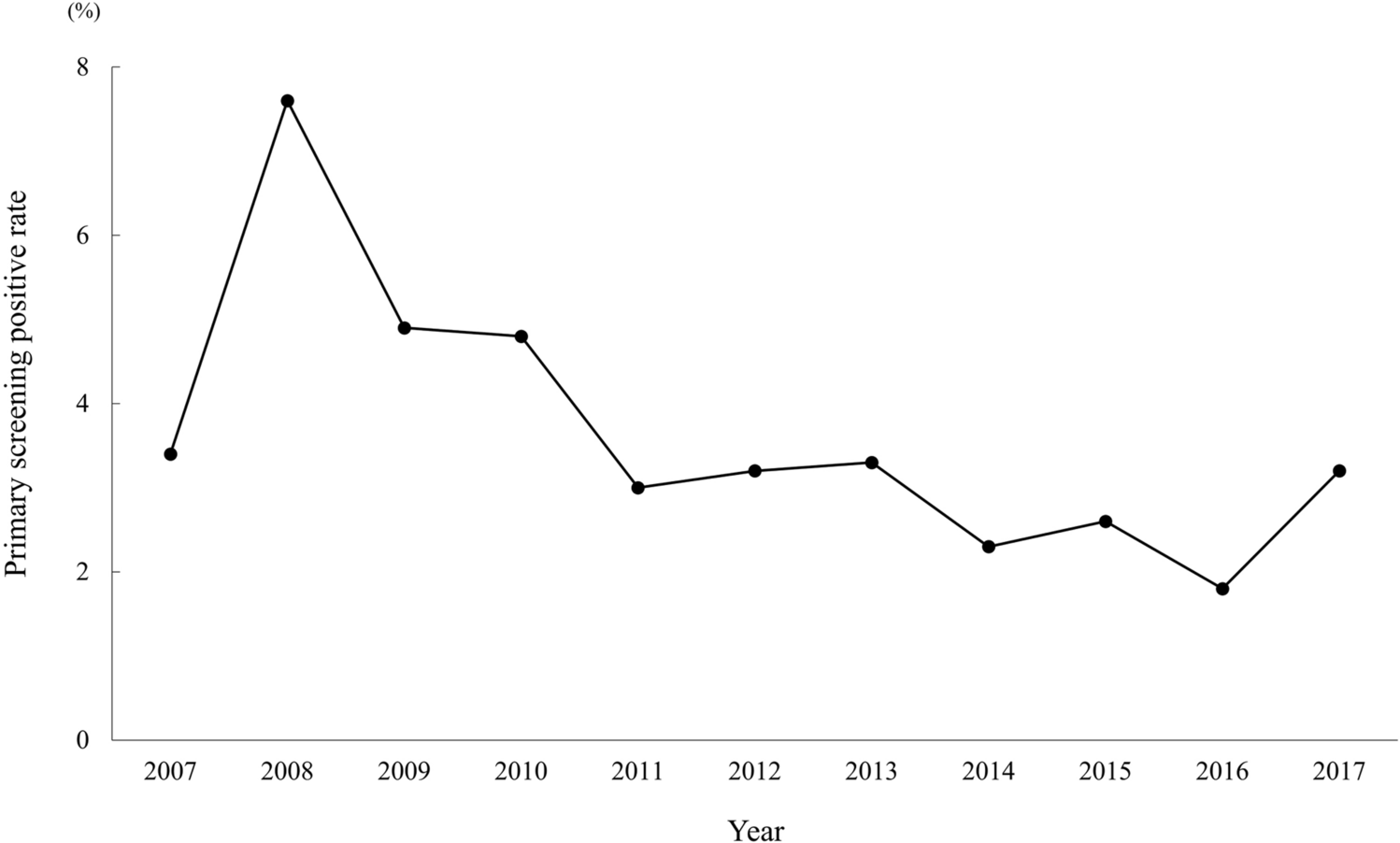
The primary screening participation rate was extremely high (99.7%) for the entire study period. Urine testing is common in school health screenings, and the use of a urine sample is considered a non-invasive way to promote participation. Our participation rate was higher than the 61.7–97.3% in previous studies of teenagers [6,7,8, 16], which cited a lack of interest for refusing to participate [16]. Carefully educating high school students and their parents about H. pylori infection may help heighten their understanding and willingness to consent. Indeed, the significant increase in participation rate in the late period suggested greater comprehension through the yearly continuation of H. pylori screening. The urinary anti-H. pylori antibody-positive rate over the 11-year period mostly remained below 5%, with the H. pylori infection rate low as in previous reports on adolescents [6,7,8, 16]. The infection rate among children was presumed to decrease annually [17], which was evident by the significant decline in the late period. Further decreases may be expected over time. We observed that the secondary test positive rate was significantly higher in the late period than in the early period. The immunochromatography method employed for measuring urinary anti-H. pylori antibodies as the primary screening in this study can be influenced by visual interpretation and the presence of proteinuria [10, 18]. It is possible that these factors affected the early primary screening results more than the later ones although the exact reason for the difference in rates is uncertain. Taken together, the introduction of H. pylori screening into school health checkups may be effective in identifying infected youths owing to a very high participation rate.
On the other hand, only 56% of primary screening-positive students underwent secondary screening following recommendations by a school doctor, with the remaining 44% lost to follow-up. Endoscopy was employed as additional screening at our hospital, which might have been perceived as overly invasive for the students. Thus, the time and the effort required for secondary screening along with the invasiveness of endoscopic examinations may have influenced our results. In another report, H. pylori status was judged by a urea breath test as secondary screening by the so called “test-and-treat strategy” [8], and so whether endoscopy is unnecessary remains to be determined. Future considerations to increase follow-through to secondary screening may include a hybrid strategy, with the option of either EGD or a urea breath test after careful explanation to the student and parents.
Although the purpose of endoscopy in this study was to more precisely investigate the actual status of upper gastrointestinal lesions and H. pylori susceptibility trends in young students, we still advocate EGD as secondary screening in clinical practice for several reasons. First, we were able to perform culture tests using the obtained biopsy samples, which improved eradication success rates. Our study showed a high CAM resistance rate of 41% during the 11-year period. CAM resistance of H. pylori among children in Japan has been increasing, with published rates of 40.7% from 2003 to 2007 [19], 52.6% from 2007 to 2012, and 84.6% from 2013 to 2018 [20]. In our cohort, CAM resistance rate increased from 35.9% in the early period to 45.1% in the late period. Despite being lower than figures reported in the last decade, CAM resistance among young people was consistently high, with some years over 50%. The MNZ resistance rate in this investigation was also high at 45.6% and comparable to a report of 53% among children in East Asia from 2005 to 2015 [21]. Globally, it has been established that eradication regimens should achieve ≥ 90% efficacy [22]. Although the CAM resistance rate of H. pylori is currently considered the main cause of eradication treatment failure [23], we could achieve a high initial eradication success rate of 96.5% by selecting the initial regimen based on the results of susceptibility testing. CAM has virtually no antibacterial effect against CAM-resistant strains, whereas MNZ continues to exhibit some effects against MNZ-resistant strains [24]. Therefore, a method of eradication therapy exclusively with a MNZ-based regimen without susceptibility testing is possible. However, MNZ is reportedly carcinogenic in animals and mutagenic in vitro [25]. While unlikely to increase the risk of carcinogenesis in humans, MNZ should be used conservatively due to the lack of long-term data [26]. Recently, P-CAB-based triple therapy was found to be more effective than PPI-based regimens for first-line H. pylori eradication therapy, even against CAM-resistant strains [27]. However, the success rate of P-CAB-based first-line eradication in junior high school students was less than 90% at 83.8–85.7% [6, 7, 28,29,30]. In the present study, we observed no significant therapeutic differences between PPI-based and P-CAB-based regimens, with both achieving high eradication success rates. Therefore, it still appears desirable to select the H. pylori eradication regimen after testing for CAM resistance rather a default PPI-based or P-CAB-based approach.
Another merit of endoscopic approaches to secondary screening is that clinicians can diagnose gastrointestinal diseases and evaluate the degree of inflammation of the gastric body, which is considered a carcinogenic risk factor for diffuse-type gastric cancer in nodular gastritis [1, 31, 32], as well as the extent of atrophy and intestinal metaplasia as risk factors for differentiated gastric cancer [33] using biopsy samples. In this study, the most common endoscopic finding in H. pylori-infected students was nodular gastritis (83.3%), with several cases of gastroduodenal ulcer scars. Although rare, gastric cancer associated with H. pylori has been reported in children and adolescents [34]. Since young people are generally at low risk of carcinogenesis, however, the follow-up protocol after eradication has not yet been established. We earlier described a case of advanced gastric cancer detected 3 years after eradication for nodular gastritis in a student subject [35], which highlighted that gastric cancer after eradication was rare, but possible, in young patients. We have also reported that young patients with nodular gastritis may have a low risk of carcinogenesis due to fewer inflammatory changes in the gastric body versus afflicted adult patients [36]; however, the severe inflammation detected in some youths suggested a future possibility of cancer [36]. Indeed, the above case of advanced gastric cancer 3 years after eradication had shown moderate inflammation in the gastric body in histological evaluations before eradication therapy [35]. A small number of cases already showed histological atrophy of the gastric body and intestinal metaplasia in this study. International consensus advocates that the H. pylori test-and-treat program should ideally target a younger adult population, such as individuals 20–40 years of age, before any potential preneoplastic changes in the gastric mucosa [22]. Considering the histological results of this study, intervention also appears beneficial in teenagers. Although risk stratification for gastric cancer after eradication based on pre-treatment histological analysis has been proposed [37, 38], there are as yet no reports on young patients or follow-up protocol. Endoscopic biopsy sampling of the gastric mucosa to assess histological findings before eradication may help predict future carcinogenesis and establish a more optimal follow-up strategy. However, if H. pylori school screening is to be implemented nationwide with EGD as secondary screening, several practical considerations must first be resolved, such as cost, capacity of endoscopy, and perceived invasiveness. Future multi-center prospective studies are warranted.
Adverse events associated with eradication therapy were observed in 12.9% of students. Skin rash was the most common event, while soft stool/diarrhea, another known side effect, was the second most common event. Adverse events in children and adolescents treated with PPI- or P-CAB-based triple therapy range widely from 4.0% to 66.2%, with soft stool/diarrhea ranging from 1.4% to 36%, and skin rash ranging from 0.1% to 4.5% [6, 7, 23, 28,29,30, 39, 40]. The incidences of adverse events observed in this study were comparably frequent but ranked differently. However, since the survey was conducted by interview only, there was a risk of underreporting if a student did not mention any events. In our intergenerational comparison of eradication therapy, younger patients exhibited more frequent and severe adverse events compared with middle-aged and older patients [41]. As a student required hospitalization in the present cohort, special attention to skin rash and other adverse events is advised during eradication therapy in young patients. Susceptibility testing to increase the initial eradication rate will also help complete treatment in a single session and reduce the risk of complications, which has been recommended in pediatric guidelines [42].
There were several limitations to this study. First, as it was conducted at a single high school, a larger scale survey is needed to fully consider the introduction of this trial into the nationwide school screening system. Second, no follow-up of students after H. pylori eradication was conducted; long-term monitoring is necessary to clarify the effect of eradication in young people on gastric cancer prevention. Nonetheless, we believe that this study remains meaningful since it sheds light on the trends in H. pylori infection rates, the clinicopathological characteristics of H. pylori-infected students including endoscopic findings, and the usefulness and the safety of eradication therapy over an 11-year period.
In conclusion, the introduction of primary screening in high school health checkups helped clarify the clinicopathological characteristics of H. pylori-infected students and the results of eradication therapy. Although it will be necessary to improve the secondary screening participation rate and contend with antibiotic resistance, this project exemplifies the utility of introducing H. pylori screening and eradication in youths, which may help prevent gastric cancer.


Comments (0)