
Remember me

This current case highlights rare and important issues in the field of infectious diseases; (1) the mixed infection caused by a rare fungus and a virus, and (2) the mNGS examination can rapidly and accurately identify pathogens and reveal changes in pathogen dominance. For the former issue, corneal scraping mNGS identified the fungal species S. lycopersici, contributing to the first reported case of keratitis caused by this pathogen. S. lycopersici, originally isolated from Solanum lycopersicum in Japan [18], belongs to the order Pleosporales (subclass Dothideomycetes), the family Pleosporaceae, and the genus Stemphylium, which is a significant plant pathogen [19]. Stemphylium spp. are important fungi characterized by dark filamentous spores and have a wide global distribution. Stemphylium spp. hold a crucial place in the classification of hemipteran fungi and can be distinguished into 28 species based on gene regions. Woudenberg et al. have meticulously detailed the morphology of S. lycopersici in their study (Fig. 4) [20]. We hypothesized that S. lycopersici may have been introduced into the immunosuppressed cornea through an external foreign body. Additionally, the patient’s cornea was damaged by stone chips, which could alter the immune barrier on the ocular surface. This injury may have facilitated the development of mixed polybiotic infectious keratitis in this case. We believe that using mNGS examination of corneal scrapes to identify fungal species could help identify this new pathogen of keratitis.
Fig. 4
Stemphylium lycopersici conidiophores and conidia after 7 d on PCA. Reprinted with permission from Woudenberg & Crous, ‘Stemphylium revisited’, *Studies in Mycology*, vol. 87, no. 1, p.77–103, 2017. Copyright 2024 by the Westerdijk Institute of Fungal Biodiversity
In general, it is difficult for ophthalmologists to quickly identify pathogens and detect changes in the prevalence of pathogens in mixed infections by standard examination and clinical review. In instances of refractory infectious keratitis where empirical treatment fails, several possibilities should be considered: (1) incorrect diagnosis of the pathogen and subsequent drug selection, (2) the presence of a mixed infection involving multiple microorganisms, (3) evolving microbial resistance, (4) systemic diseases that compromise ocular surface immunity, and (5) patient drug adherence was poor. We eliminated (4) and (5) as causes since the patient lacked a history of systemic diseases affecting the immunity of the ocular surface and demonstrated consistent adherence to their medication regimens. In the case of (1) and (2), the mNGS should be used to quickly identify all pathogens, enabling timely adjustments to the treatment plan. For scenario (3), the mNGS can discern the pathogenicity of microorganisms in infectious keratitis and pinpoint dominant shifts, thus facilitating prompt medication modifications. Furthermore, if feasible, microbial scraping should be performed for drug susceptibility testing. In this case, given the negative corneal scrape culture result, we used IVCM to diagnose a fungal infection and administered the appropriate empiric treatment. However, the inability to identify the specific type of fungus and diagnose mixed infections led to suboptimal treatment results. Thus, mNGS testing was conducted, which precisely identified the types of pathogenic microorganisms and diagnosed mixed infection. When presenting the results, the scientific method of mNGS minimizes the influence of contamination and eliminates the influence of the common ocular flora, significantly enhancing the reliability of the findings.
Challenges in clinical and microbiological diagnosisIK is an ophthalmic emergency that can cause significant corneal damage, leading to corneal opacification, and is one of the leading causes of blindness worldwide [1]. Early identification of the pathogen responsible for corneal infection allows rapid and optimal treatment, preventing irreversible corneal damage and significantly improving the chances of full recovery. However, clinical features are not specific to the type of microbial keratitis, making the early accurate diagnosis of IK challenging [21]. Consequently, both in vivo and in vitro tests are necessary to aid in the early diagnosis of IK. Corneal smears and cultures remain the gold standard for IK diagnosis; however, these methods lack sensitivity. Fungal cultures are particularly time-consuming, and some rare species require two weeks or more to confirm the presence or absence of pathogen growth [22]. Other widely used diagnostic modalities, such as direct microscopy, IVCM, and histopathological examination, also have significant drawbacks. These methods often result in a low positive rate for early diagnosis and may overlook mixed infections, preventing patients from receiving effective treatment promptly and leading to severe consequences [23]. The emergence of newer technologies highlights the inadequacies of older methods, which do not provide accurate and timely diagnoses necessary to guide treatment and preserve patients’ vision.
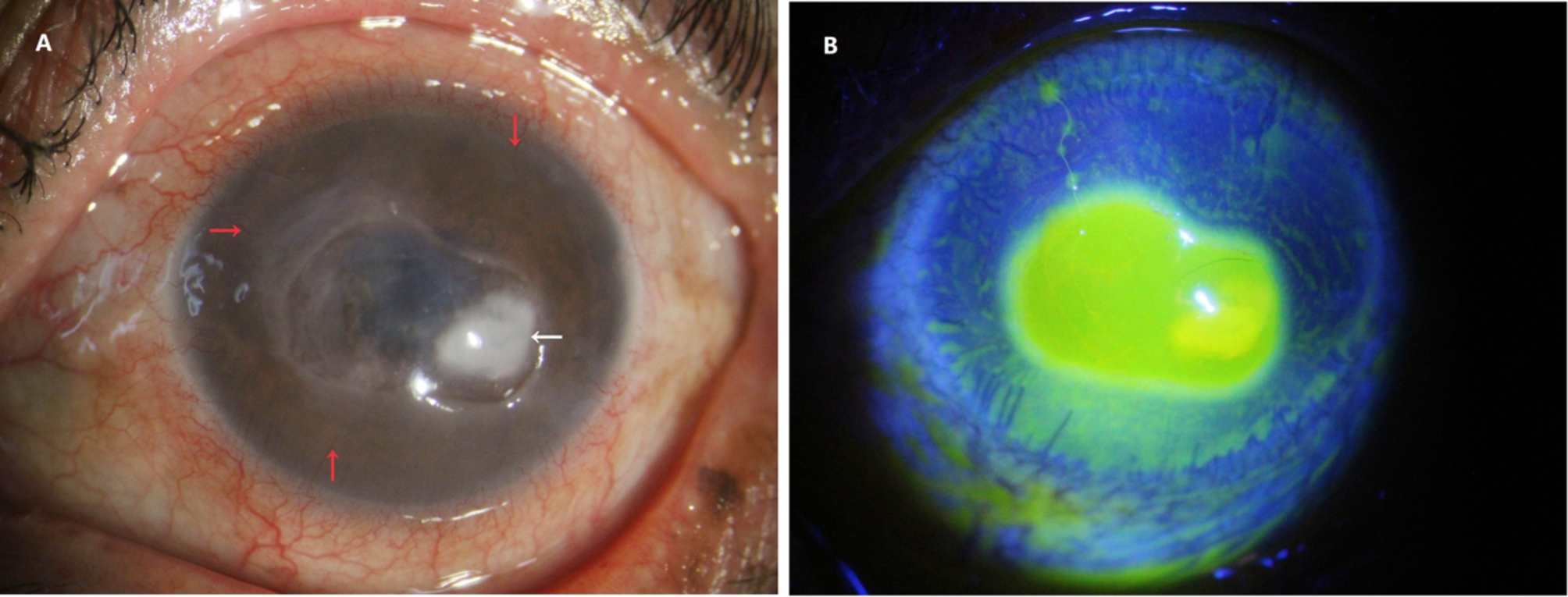
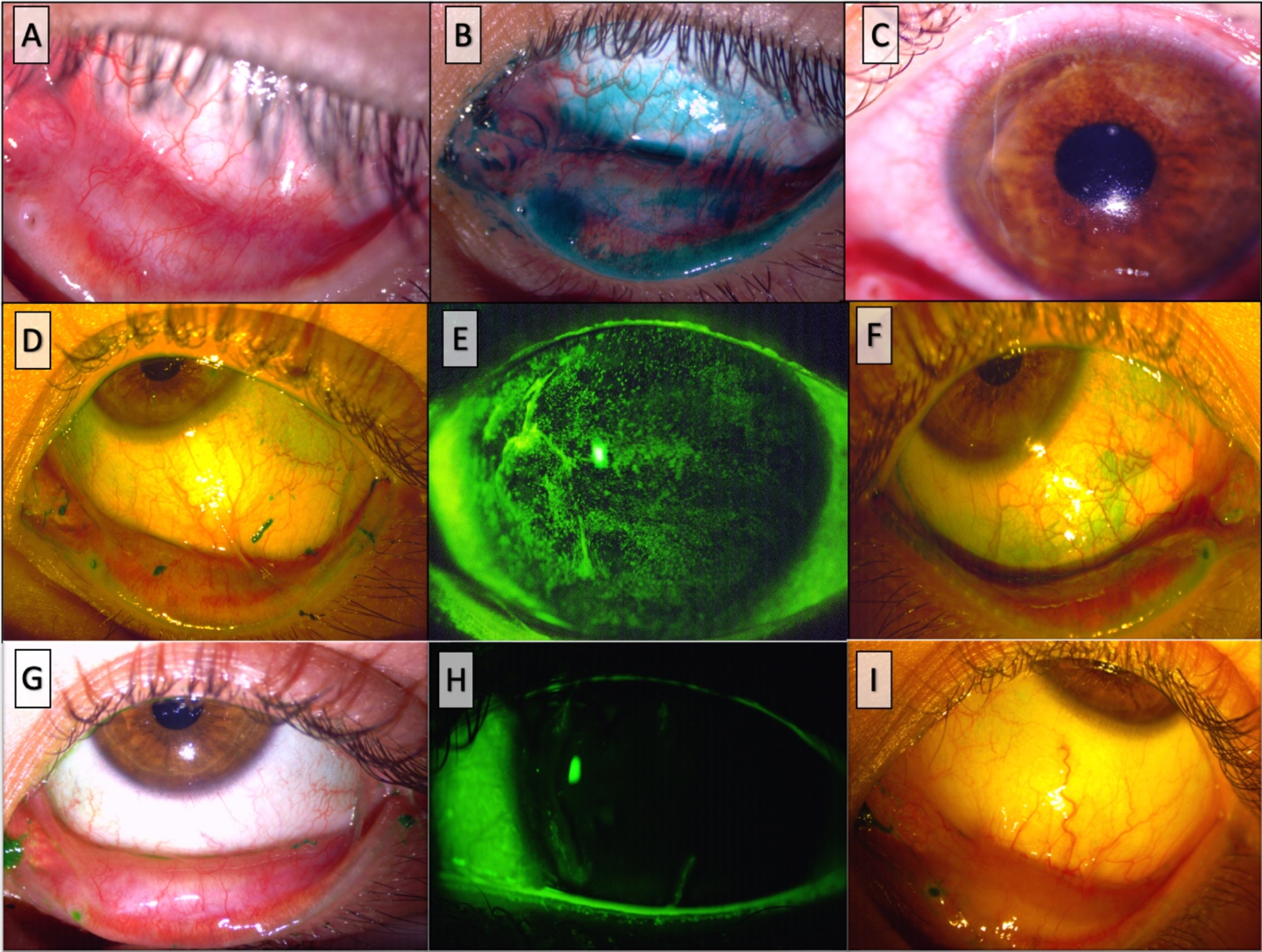
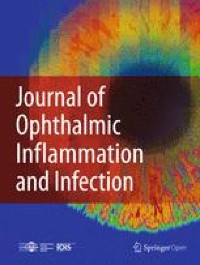
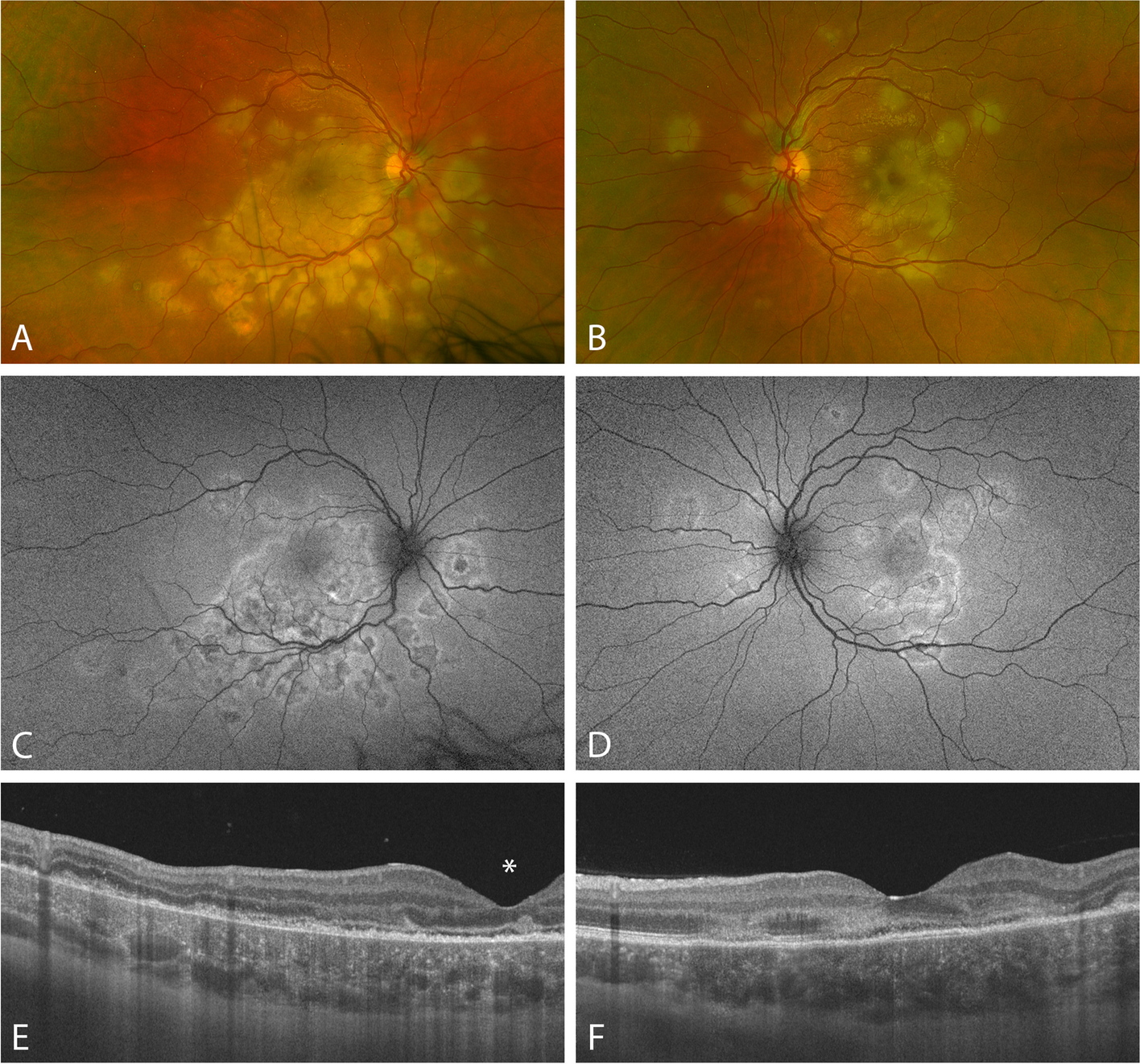
The patient had previously been treated in a local hospital before seeking care in our facility. Due to the inability to identify the pathogen, empirical treatment with levofloxacin eye drops tobramycin eye drops, and ganciclovir ophthalmic gel was administered. This approach masked clinical symptoms and delayed the accurate diagnosis and treatment of the disease. A corneal scraping culture yielded negative results and an IVCM examination suggested a fungal infection. Although many clinical features of fungal keratitis overlap, identifying the specific fungal species is crucial to guide the appropriate treatment. There are no distinct ocular signs to differentiate the rare fungal keratitis caused by S. lycopersici from other types of fungal keratitis. Empirical treatment with 5% natamycin eye drops was initiated, but the response was poor. Subsequent corneal scraping mNGS identified a mixed infection caused by S. lycopersici and human alphaherpesvirus 1.
Challenges in clinical treatmentBroad-spectrum topical antibiotics are commonly used by clinicians to treat corneal infections of unknown etiology [24]. However, its extensive use alters the microbial spectrum and the respective antibiotic susceptibility patterns, potentially increasing the prevalence of drug-resistant bacteria that cause disease [25]. AMR has become a major public health threat in the 21 st century, driven by various factors, including diagnostic uncertainty leading to inappropriate antibiotic use [26]. In the current ‘post-antibiotic’ era, clinicians must exercise greater caution when choosing antibiotic therapy [27].
Ray et al., in their SCUT trial, discovered that the minimum inhibitory concentration (MIC) of bacteria isolated from patients with IK who had been pretreated with topical fluoroquinolones was 3.48 times higher than in those who had not received such treatment [28]. A subgroup analysis of the Mycotic Ulcer Treatment Trial I (MUTT I) also revealed that patients with IK treated with topical antifungal medications experienced a mean increase in MIC of 2.14 times per year, even after adjusting for pathogen factors [29]. Emerging technologies such as mNGS and artificial intelligence-assisted platforms improve the microbiological diagnosis of IK [30, 31], thus improving treatment and reducing the risk of AMR.
Comments (0)