Study design
This double-blinded, prospective, randomized controlled trial (RCT) was conducted at a single orthopaedic centre in Poland. The Bioethics Committee of Poznan University of Medical Sciences approved the study protocol on September 13, 2023 (protocol number 541/2023). Subsequently, the trial was registered at ClinicalTrials.gov (NCT06470139) on August 13, 2024. Before participation, written informed consent was obtained from all patients following ethical research standards. Patient enrollment occurred between August 14, 2024, and January 31, 2025. The study was conducted in full compliance with the principles outlined in the Declaration of Helsinki.
Participants
Patients scheduled for total hip arthroplasty under spinal anesthesia were considered for enrollment before surgery. Inclusion criteria encompassed individuals aged 65 to 100 years who could provide informed consent and reliably report symptoms to the research team.
Exclusion criteria included patients who declined participation or could not provide first-party consent due to cognitive impairment or language barriers.
Randomization and blinding procedures
A computer-generated randomization process assigned patients in a 1:1 ratio to one of the following groups: the PENG group – received an ultrasound-guided PENG block, and the PENG + DEX group –received an ultrasound-guided PENG block with Dexamethasone. The randomization list was generated using the nQuery Advisor program (Statistical Solutions, Boston, MA, USA) by a researcher who was not otherwise involved in the study. Group allocations were concealed in opaque, sequentially numbered envelopes to ensure allocation concealment until the moment of intervention.
Blinding protocol
This study maintained double-blinding through strict role separation among researchers. A designated independent researcher, who had no role in patient care or outcome assessment, prepared the randomization list and sealed the group assignments in numbered envelopes. Before the orthopaedic procedure, the"first"consultant anesthesiologist received and opened the assigned envelope and administered the PENG block, or PENG block, with Dexamethasone according to the allocated group. Immediately after performing the nerve block, the"first"anesthesiologist was replaced by a"second"consultant anesthesiologist, who remained blinded to the group assignment and supervised all anesthesia-related procedures during surgery. Throughout the study, the anaesthesia team, surgical team, operating room staff, patients, and outcome assessors remained blinded to the intervention received. Group allocation was only revealed after the completion of statistical analyses to prevent bias.
Procedures
In both study groups, patients received an individualized dose of midazolam (ranging from 2.5 mg to 7.5 mg p.o.) approximately 30 min before surgery as part of a multimodal preemptive analgesia protocol. The exact dose was tailored based on the patient’s age, weight, and comorbidities. All patients underwent standardized spinal anaesthesia under mild sedation, tailored for geriatric tolerance. Sedation was achieved with a continuous propofol infusion, adjusted within a 2–5 mg/kg/hour range, administered throughout the surgery. The infusion rate was carefully titrated to maintain adequate sedation while minimizing respiratory depression. Oxygen supplementation was provided via a face mask at a flow rate of 3–5 L/min, adjusted according to the patient’s oxygenation status and respiratory function. Spontaneous ventilation was maintained throughout. Spinal anaesthesia was performed at the L3/4 interspace using a 27 G, 90 mm Sprotte needle (PAJUNK) with 4 ml of 0.5% ropivacaine. The surgeon performed no periarticular infiltration during the procedure. The “first” and “second” anaesthesiologists involved in this study had over five years of post-specialty clinical experience focusing on regional anaesthesia, specifically nerve blocks.
PENG block procedure
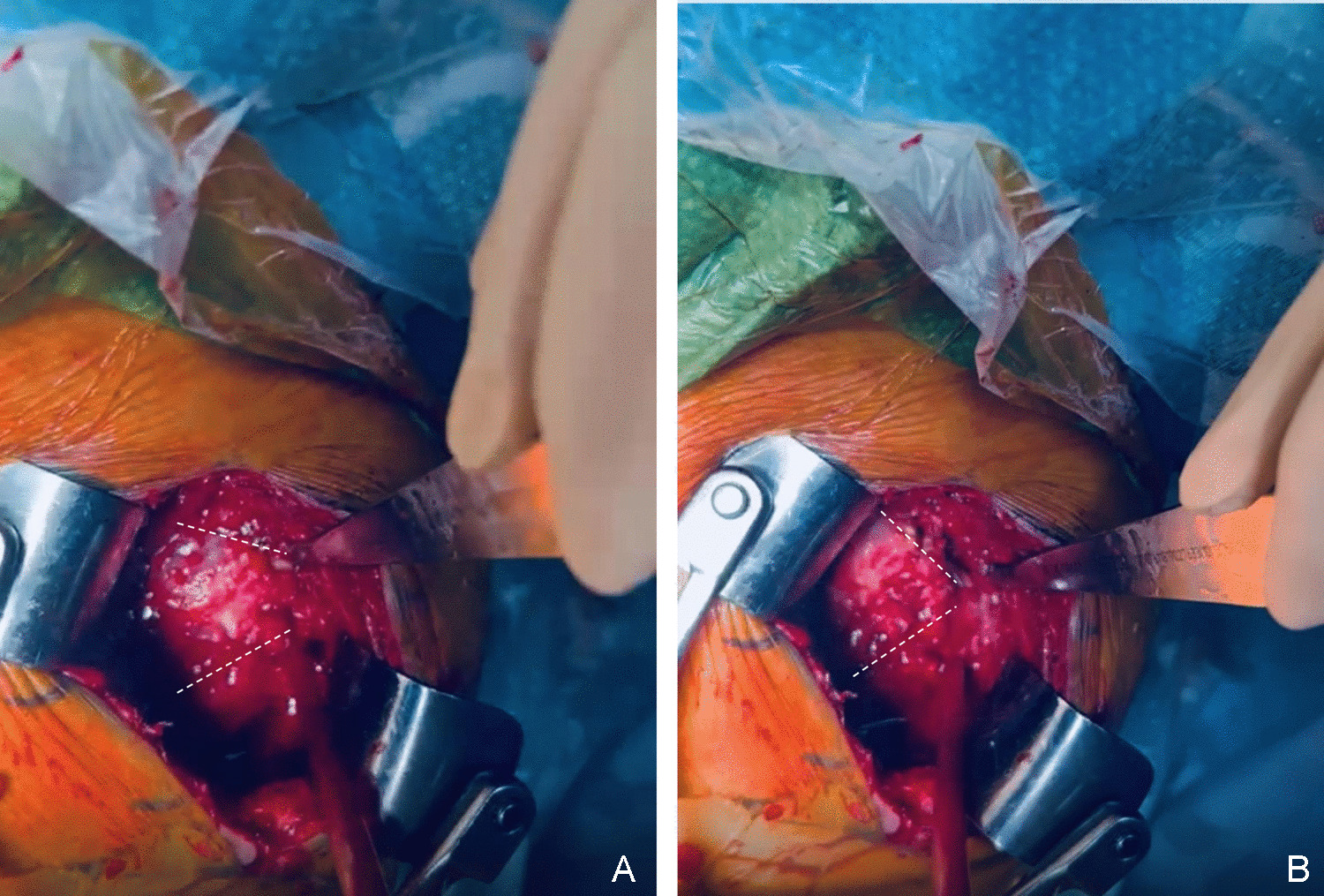
Following the administration of spinal anaesthesia and before the surgical incision, the PENG block was performed with the patient in the supine position. A curvilinear, low-frequency (4–8 MHz) ultrasound probe guided a 22-gauge needle (Stimuplex Ultra 360, 80 mm) inserted in a lateromedial direction. The needle was positioned laterally to the iliopsoas tendon to prevent quadriceps weakness between the ilio-pubic eminence and the anteroinferior iliac spine. Hydro-location was confirmed with 0.5 ml of 0.9% isotonic saline. After confirming negative aspiration, either 20 ml of 0.2% ropivacaine with 2 ml of 0.9% NaCl, or 20 ml of 0.2% ropivacaine with 4 mg of dexamethasone was slowly administered laterally to the iliopsoas tendon, according to the patient’s randomized group assignment.
Surgical and postoperative protocol
All patients underwent hip arthroplasty under spinal anaesthesia performed by a single surgical team consisting of four orthopaedic surgeons at the Orthopedic Hospital, Poznan University of Medical Sciences. The Direct Superior Approach (DSA) was consistently used across all patients, and an uncemented implant (Smith & Nephew Polarstem/R3) was implanted in each case.
Postoperative care and follow-Up
A radiographic evaluation was conducted on the first postoperative day. Patients followed a standardized rehabilitation and pain management protocol (detailed in the following sections). Weight-bearing as tolerated was encouraged, and patients were mobilized with hikers. Each patient underwent a minimum of two days of active follow-up postoperatively. An independent researcher collected Primary and secondary outcomes during in-hospital visits, ensuring unbiased data collection.
Postoperative analgesia and thromboprophylaxis management
Postoperative pain management followed a multimodal analgesic protocol, incorporating a combination of non-opioid and opioid analgesics to optimize pain control while minimizing opioid consumption. The regimen included: Acetaminophen 1.0 g every six h, Metamizole 1.0 g every six h, Ibuprofen 400 mg every eight h. For rescue analgesia, if a patient’s Numerical Rating Scale (NRS) score reached ≥ 4, a 5 mg intravenous oxycodone bolus was administered. To ensure standardized reporting and facilitate comparisons with other studies, total opioid consumption was expressed in morphine milliequivalents (mEQ), using a standard conversion ratio of 1 mg oxycodone = 1.5 mg morphine.
Thromboprophylaxis and early mobilization
All patients received daily enoxaparin for four weeks postoperatively as prophylaxis against thromboembolic events. Early mobilization was initiated ten h after surgery, with patients ambulating under supervision using a hiker to promote functional recovery and reduce postoperative complications.
Outcome measures
The primary outcome was the time to the first administration of rescue opioid analgesia, which was assessed by residents from the postoperative and orthopaedic wards who were not involved in the study.
Secondary outcomes included total opioid consumption, which was recorded in milligrams of oxycodone from the orthopaedic ward records. This data was converted into morphine milliequivalents (mEQ) using the standardized conversion ratio (1 mg oxycodone = 1.5 mg morphine) to ensure consistency with other studies. Residents and fellows, who were blinded to the study, performed these assessments. Pain intensity was evaluated using the Numerical Rating Scale (NRS) at predefined postoperative time points (4, 6, 12, and 24 h after surgery). The NRS ranged from 0 (no pain) to 10 (worst pain imaginable). Two independent physicians conducted these evaluations, and the final pain score was determined through mutual agreement at the end of the assessment. Quadriceps muscle strength was assessed using the Medical Research Council (MRC) Scale for Muscle Strength, where Grade 5 represents normal muscle strength, Grade 4 indicates movement against gravity and resistance, Grade 3 indicates movement against gravity over nearly the entire range, Grade 2 indicates movement of the limb but not against gravity, Grade 1 represents visible contraction without movement of the limb (not applicable to hip flexion), and Grade 0 indicates no visible contraction. Two independent physicians evaluated quadriceps strength, and the final score was determined by consensus at the end of the assessment.
Nerve injury was assessed retrospectively on the day of discharge based on documented neurological deficits in the orthopaedic ward records. Nerve deficits were classified as follows: 0: No nerve damage, 1: Minor sensory paraesthesia, 2: Complete sensory anaesthesia, 3: Complete motor deficit with or without sensory paraesthesia, 4: Complex Regional Pain Syndrome. Two researchers, blinded to group allocation, reviewed and classified these outcomes.
Blood glucose levels were measured at 12, 24, and 48 h postoperatively. Blood samples were collected by nursing staff, blinded to the study, and analyzed by two independent researchers who were also blinded to group allocation.
Statistical analysis
The sample size was based on our primary hypothesis that the time to first rescue opioid analgesia would be significantly longer in the PENG + DEX group than that in the PENG group. Our null hypothesis was that there would be no significant difference in the time to first rescue analgesia between these two groups. The time to first rescue opioid analgesia was the primary variable. Based on a pilot study on ten patients, not included in the final analysis, the time to first rescue opioid analgesia was 9.46 ± 4.43 h (mean ± SD) in the PENG group and 14.26 ± 4.16 h (mean ± SD) in the PENG + DEX group. Using pairwise comparison, we calculated the sample size required to detect a difference in the time to first rescue opioid analgesia among the two groups. Accordingly, 22 subjects were required in each group to achieve a statistical power of 95% at a p-value of < 0.05. To facilitate block randomization and account for loss to follow-up, 30 patients per group (60 in total) were recruited.
Statistical analysis was performed using GraphPad Prism 10.1.1 (270) software (GraphPad Software Inc., San Diego, CA, USA). The parametric distribution of numerical variables was evaluated using the Shapiro–Wilk normality test. Differences between groups were assessed using the ANOVA with post hoc Tukey’s test. Categorical variables were compared with the Kruskal–Wallis test, and contingency analysis between groups was conducted using Fisher’s exact test. A p-value of < 0.05 was considered statistically significant and was calculated with 95% confidence intervals (Cl).





Comments (0)