
Remember me
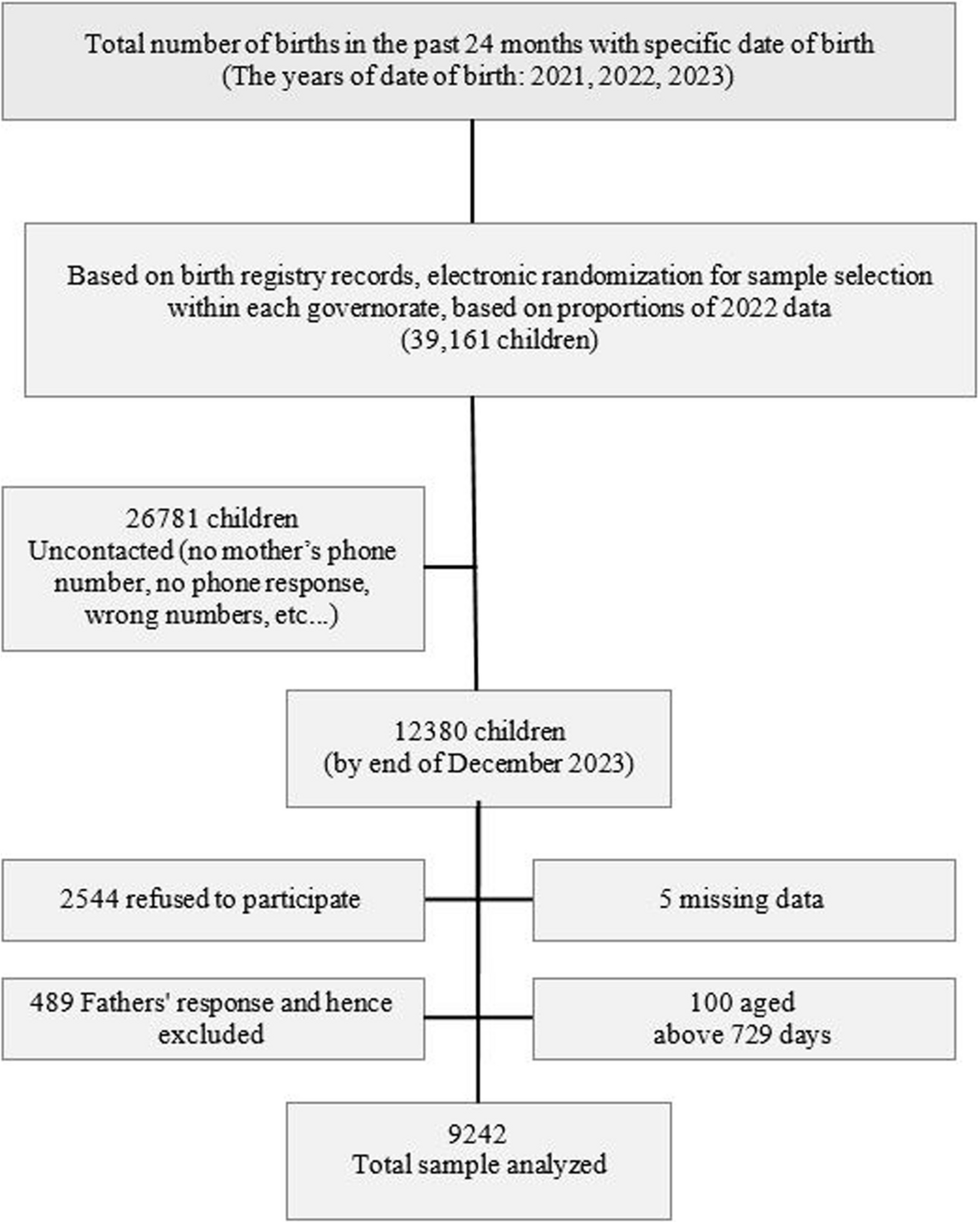


This was a prospective longitudinal study. The final sample consisted of 397 mother and infant pairs from the ECLIPSES-NEN study [23], a follow-up project of ECLIPSES study. The ECLIPSES-NEN study aimed to explore nutritional, environmental, sociodemographic, and emotional factors during pregnancy and early infancy that are related to child development. The participants in ECLIPSES-NEN were originally recruited as pregnant women for the ECLIPSES study [24]. Recruitment was carried out by midwives at primary care centres during the participant’s first pregnancy visit. Inclusion criteria were: to be at least 18 years old; being pregnant for 12 weeks or more; not having anaemia (Hb > 110 g/L), and understanding either of the country’s official languages (Spanish or Catalan), as well as the study characteristics. The exclusion criteria were to have a multiple pregnancy, to have had an adverse obstetric history, to have taken > 10 mg of iron supplementation every day in the three months prior to the 12th week of gestation, to have reported prior severe illness (state of immunosuppression) or chronic disease that could affect their nutritional status (cancer, diabetes, etc.), or to have reported liver disease.
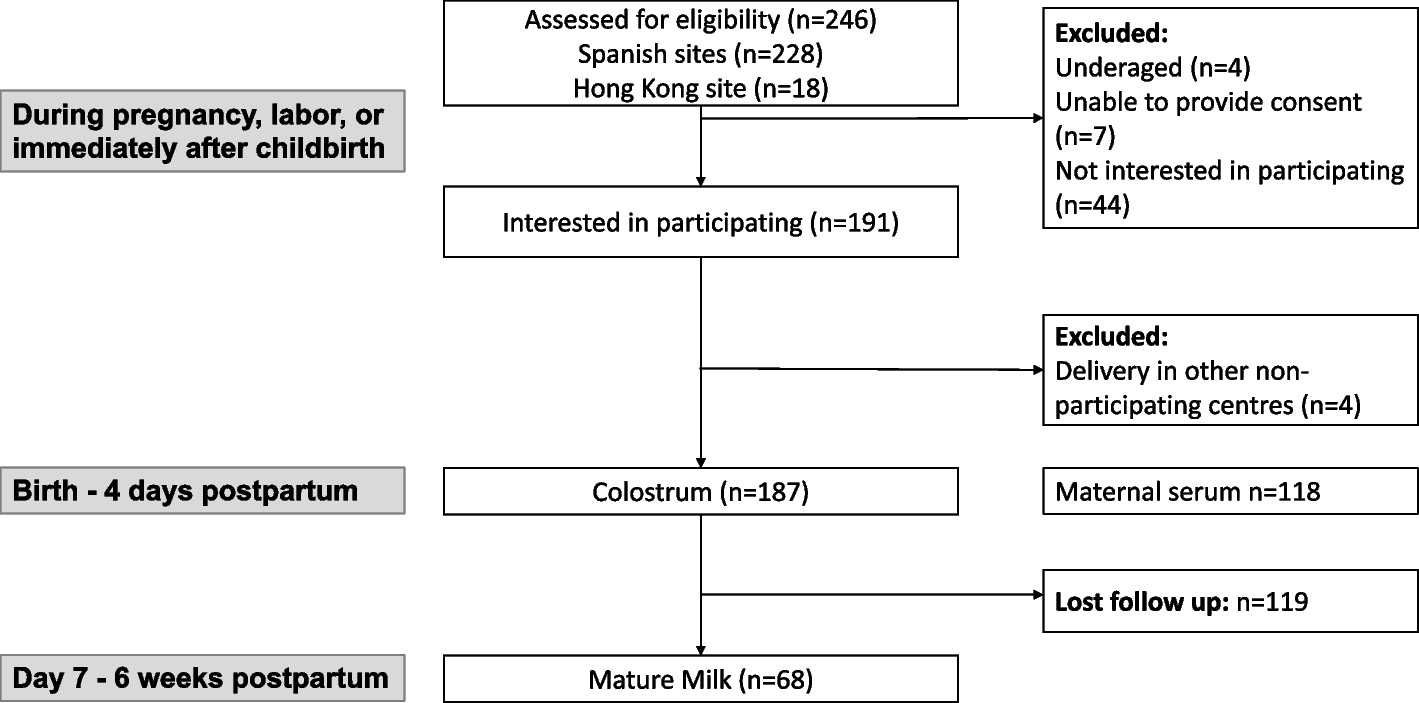
The ECLIPSES study consisted of three visits during pregnancy (in the 12th, 24th, and 36th weeks), a visit 40 days after delivery (postpartum visit) and the ECLIPSES-NEN consisted of a follow-up visit 4–5 years after delivery. Sociodemographic, clinical and psychosocial information were collected. A total of 793 pregnant women were included in the study at week 12 of pregnancy, 547 women provided data at week 24, 496 at week 36, and 466 at 40 days after delivery. At 4 years old, a total of 397 infants and their mothers came to the follow-up visit. Participant dropout was caused by voluntary abandonment, emergence of exclusion criteria during pregnancy, miscarriage, and lost to follow-up.
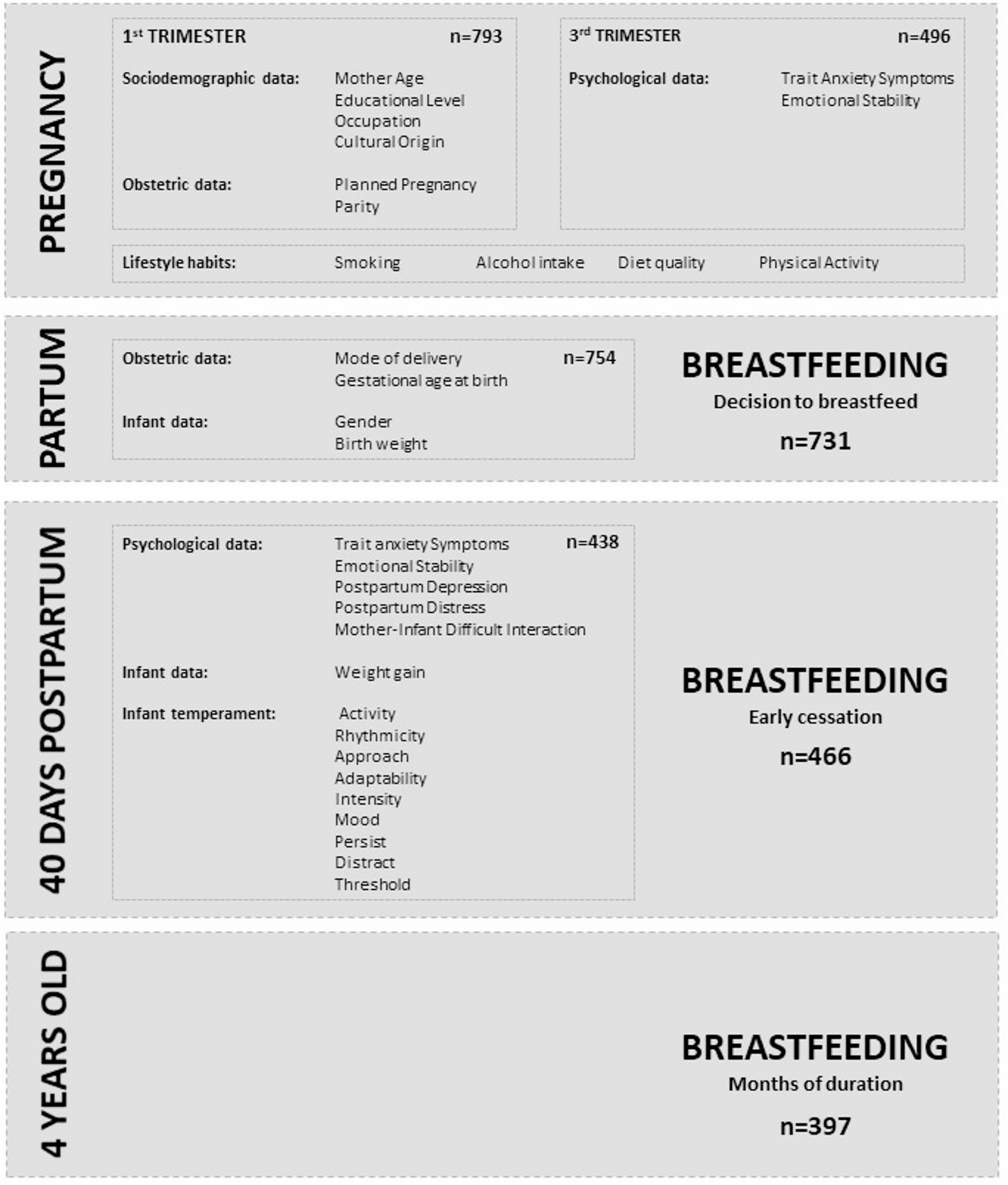
Figure 1 illustrates the longitudinal data collection across pregnancy, partum, 40 days postpartum, and at 4 years of age.
Fig. 1
Study design and variables
Variables and assessmentsBreastfeeding information was collected at three different times: at birth, from the hospital report when the decision to breastfeed was taken; 40 days postpartum, during the follow-up visit (if the mother reported that she had stopped breastfeeding, it was considered early cessation); and at the 4-year follow-up visit, when the total duration of breastfeeding in months was recorded. In this study, breastfeeding is considered when children have been fed with breastmilk or mixed breastfeeding.
Obstetric and neonatal data were obtained from the medical records. These variables were the mother’s age at the beginning of pregnancy; whether the pregnancy was planned; parity; mode of delivery; gestational age at birth; and infant gender and birth weight. In addition, socio-demographic data such as educational level, occupation and cultural background of the mother were collected.
The mother’s socioeconomic status (high, medium or low) was calculated using the Hollingshead index [25] by merging data about the educational level and occupation classified according to the Catalan classification of occupations [26].
The mother’s trait anxiety symptoms and emotional stability during pregnancy and at 40 days postpartum were assessed by the State-Trait Anxiety Inventory (STAI) [27], a questionnaire designed to assess symptoms of both state and trait anxiety. This self-report questionnaire contains 40 items, and two main scores and four factors can be obtained. The main scores are the state anxiety (the level of transient and situational anxiety) and trait anxiety (the level of dispositional and stable trait anxiety). The four factor scores are factor 1 (state of nervousness, tension, anxiety and restlessness), factor 2 (positive state of activation, animation, welfare, satisfaction and self-confidence), factor 3 (stable trait of melancholy, despair and feelings of inability), and factor 4 (emotional stability and absence of mood changes). This study used factor 3 as trait anxiety and factor 4 as emotional stability.
The mother’s smoking during pregnancy was assessed by the Fagerström Questionnaire (Fagerström_Q) [28]. According to this information, women were classified as smokers or non-smokers.
The mother’s diet during pregnancy was assessed using the Food Intake Frequency Questionnaire (FFQ) [29, 30], which included 45 food and beverage items. The frequency of consumption was indicated per week or per month. This information was used to estimate adherence to the Mediterranean diet as an indicator of quality of diet [30]. Qualified midwives and nutritionists administered the FFQs, and ensured accurate completion, data entry, and subsequent analysis.
Alcohol consumption during pregnancy was determined by analysing the responses to the alcoholic beverages item in the FFQ, with the responses being categorized simply as “no” or “yes”.
Physical activity during pregnancy was evaluated using the International Physical Activity Questionnaire– Short Form (IPAQ-SF) [31]. A self-administered questionnaire that includes 7 items on the frequency and duration of sitting, walking, and moderate and vigorous physical activities during the previous week. Based on the total minutes of moderate-to-vigorous physical activity reported, women were categorized as meeting or not meeting international recommendations for physical activity during pregnancy (≥ 150 min per week) [32].
The mother’s postpartum depression symptoms were assessed by the Spanish version of the Edinburgh Postnatal Depression Scale (EPDS) [33, 34], a questionnaire specifically designed to assess depressive symptoms during the postpartum period. EPDS total score was used as a continuous variable to capture the whole range of depressive symptomatology.
The mother’s distress and mother-infant interaction difficulties during postpartum were assessed by the Parent Stress Index– Short Form (PSI-SF) [35], a 36-item questionnaire designed to assess stress levels related to the parenting role. In this study, scores for mother’s distress, and mother-infant dysfunctional interaction were used.
Infants’ temperament was assessed using the Early Infancy Temperament Questionnaire (EITQ) [36], a tool designed to assess the New York Longitudinal Study temperament traits in one- to four-month-old infants. The temperament traits assessed were: activity level (the level and extent of motor activity), rhythmicity (the degree of regularity of functions such as eating, elimination and the sleep-wake cycle), approach (the response to a new object or person in terms of whether the infant accepts the new experience or withdraws from it), adaptability (the adaptability of behaviour to changes in the environment), threshold (the sensitivity to environmental stimuli), intensity (the energy level of responses), mood (the infants’ general mood or ‘disposition’, whether cheerful or prone to crying, pleasant or fussy, friendly or unfriendly), distractibility (the degree of the child’s distractibility from what he/she is doing) and persistence (the infant’s attention span and his/her persistence in that). Higher scores indicate less desirable infant characteristics.
Statistical analysisDescriptive data were expressed as means and standard deviations for continuous variables and as percentages and frequencies for categorical variables. Differences between variables in the breastfeeding groups were assessed using Chi-square tests for categorical variables and Student’s t-test for continuous variables.
To identify factors related to decision to breastfeed (no, yes) and early cessation of breastfeeding (no, yes), logistic regressions models using the stepwise method were performed. The candidate variables to be used in the model to predict the decision to breastfeed included: mother’s age (years), mother’s socioeconomic status (high, medium, low), employment status (unemployed, employed), cultural background (Spain, other), tobacco use during pregnancy (no, yes), alcohol use during pregnancy (no, yes), diet quality (score), physical activity according to international recommendations (no, yes), trait anxiety symptoms (score) and emotional stability (score) in the third trimester of pregnancy, planned pregnancy (no, yes), parity (primiparous, multiparous), mode of delivery (non-instrumental, instrumental), infant sex (boy, girl), gestational age (weeks), and infant birth weight (grams). For the model predicting the early cessation of breastfeeding, the following variables were added to the variables mentioned above: postpartum trait anxiety symptoms (score), postpartum depression symptoms (score), emotional stability (score), mother’s parenting-related distress (score), difficulties in mother-infant interaction (score), infant weight at one month (grams), and temperamental characteristics of the infant: activity (score), rhythmicity (score), approach (score), adaptability (score), intensity (score), mood (score), persistence (score), distractibility (score), and threshold (score). Finally, to explore factors related to the dependent variable total duration of breastfeeding (months) a multiple linear regression model was conducted using the stepwise method. The candidate variables for this model included all the variables from the two previous models. Estimates were presented in the form of an Odds Ratio (OR) for logistic regressions and a β coefficient (β) for multiple linear regression as well as 95% confidence intervals (CI). The collinearity between variables in the models was assessed. Statistical significance was defined as a p-value of < 0.05.
The statistical analysis was conducted using SPSS Statistics software, version 29.0 for Windows (SPSS Inc., Chicago, IL).
Comments (0)