
Remember me
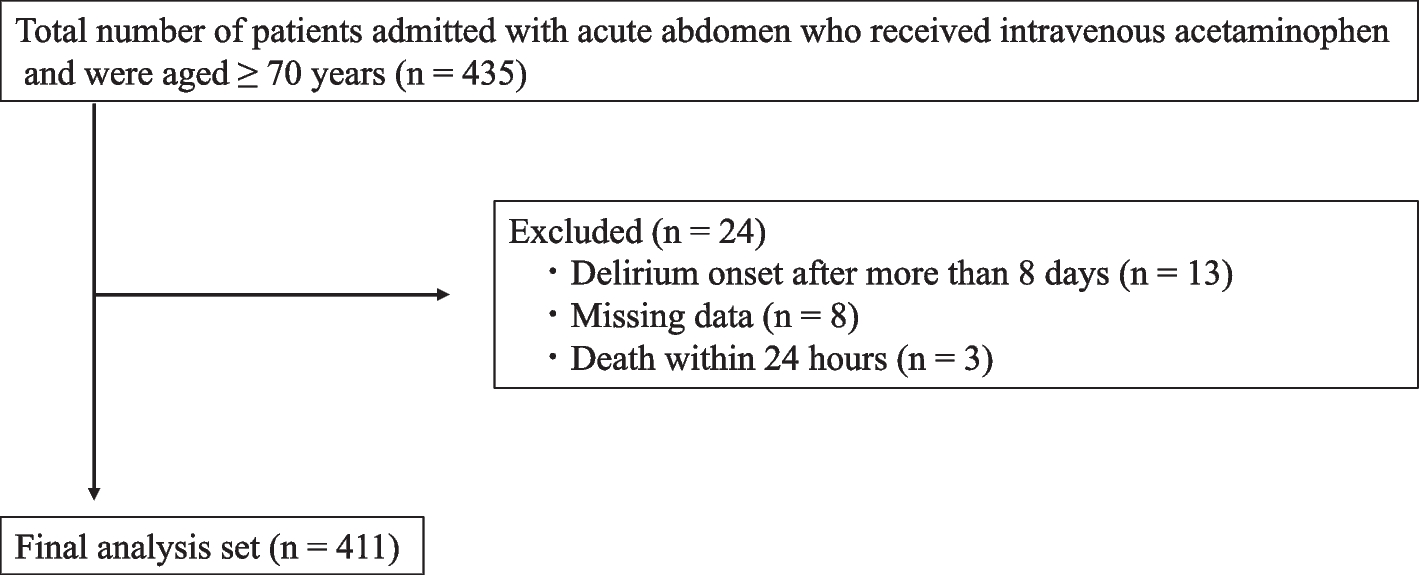
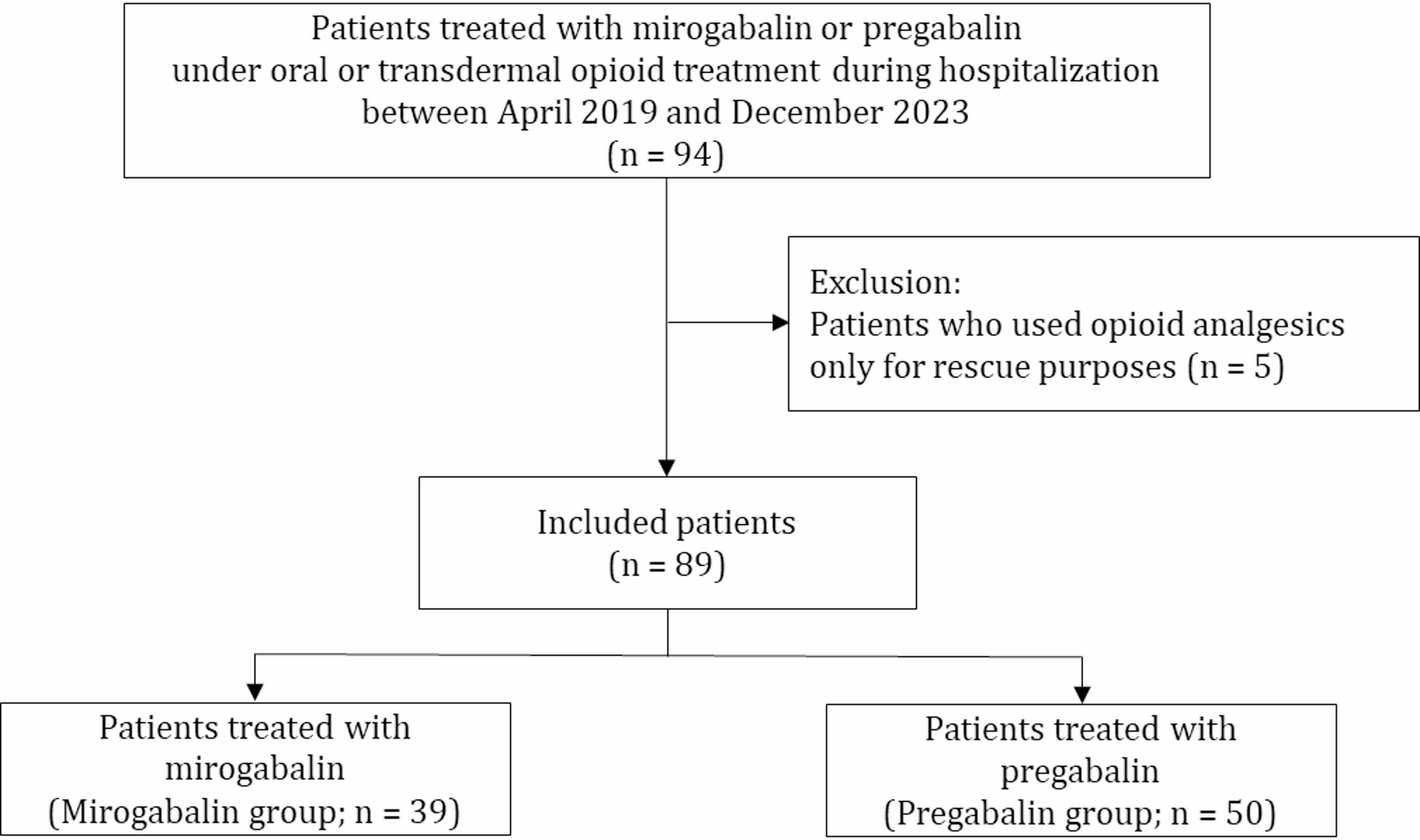
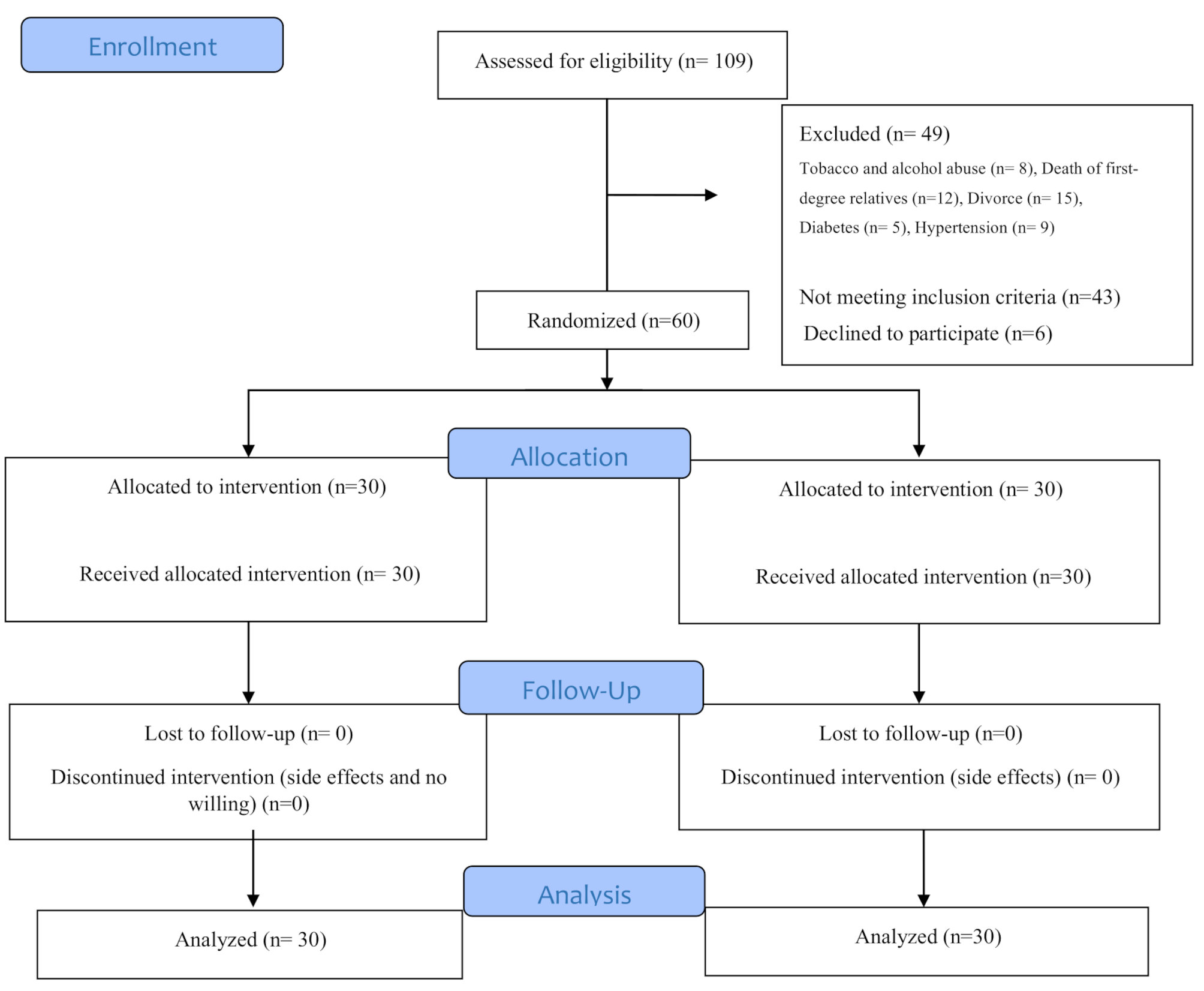


Of the 94 patients surveyed, five were excluded owing to opioid analgesic use for rescue purposes, leaving 89 included in this study. The included patients were divided into two groups: those who started receiving mirogabalin (mirogabalin group; 39 patients) and those who started pregabalin (pregabalin group; 50 patients) (Fig. 1).
Fig. 1
Patient selection flowchart
The baseline characteristics of the patients are listed in Table 1. There were no substantial differences between the mirogabalin and pregabalin groups in terms of median age (71.0 vs. 64.5 years), BMI (19.6 vs. 20.5 kg/m2), CLcr (66.3 vs. 78.7 mL/min), or the percentage of females (43.6 vs. 34.0%), respectively. At baseline, the median MMEs in the pregabalin group were approximately twice as high as those in the mirogabalin group (60 mg vs. 30 mg, respectively); however, this difference was not statistically significant. The majority of opioids—78.0% in the mirogabalin group and 89.3% in the pregabalin group—were administered orally. The proportion of patients using NSAIDs/acetaminophen was comparable between the mirogabalin (69.2%) and pregabalin (72.0%) groups. The most common initial dosage at the start was 10 mg for mirogabalin (76.9%) and 150 mg for pregabalin (34.0%). Additionally, a considerable number of patients started pregabalin at lower doses: 50 mg (26.0%) and 75 mg (26.0%).
Table 1 Patient baseline characteristicsDifferences between Mirogabalin and Pregabalin in the occurrence of Somnolence and DizzinessThe cumulative incidence curve for mirogabalin and pregabalin groups is shown in Fig. 2. The median [95% confidence interval (CI)] time of occurrence of somnolence and dizziness in the mirogabalin group was significantly shorter than that in the pregabalin group under the log-rank test (8.0 [5.0–22.0] vs. 17.0 [10.0–not reached], respectively; p = 0.039).
Fig. 2
Kaplan–Meier curves of the occurrence of somnolence and dizziness. The vertical axis shows the cumulative incidence rate using the Kaplan–Meier estimation. The horizontal axis shows the number of days since the baseline day
In the multivariable Cox proportional hazards regression analysis adjusted for age group (≥ 65 years and < 65 years), sex, presence of renal impairment (≤ CLcr 60 mL/min and > CLcr 60 mL/min), and baseline MMEs (per 10 mg unit), the mirogabalin group showed a higher risk of somnolence and dizziness than the pregabalin group (HR: 1.74 [95% CI 0.93–3.26], p = 0.117), although without significance. Furthermore, when CLcr was ≤ 60 mL/min, the risk of somnolence/dizziness tended to be higher in both groups (HR: 2.01 [95% CI 0.96–4.20], p = 0.065) (Table 2).
Table 2 Hazard ratio for occurrence of somnolence and Dizziness in patients treated with pregabalin/mirogabalin under opioid treatmentChanges in opioid dosage from baseline to occurrence of Somnolence and DizzinessThe occurrence of somnolence and dizziness might be influenced by an increase in opioid dosage. Therefore, we investigated the changes in MMEs from baseline to the occurrence of somnolence and dizziness. MMEs did not change in the mirogabalin group but increased in the pregabalin group up to the occurrence of somnolence and dizziness (median [interquartile range] = 15.0 [0–52.5], p = 0.014) (Fig. 3).
Fig. 3
Changes in morphine milligram equivalents in patients with somnolence and dizziness in each group. The central line in each box represents the median, while the upper and lower edges indicate the first and third quartiles. The whiskers extend to 1.5 times the interquartile range, and any points beyond this range are considered outliers (denoted as dots). MMEs, morphine milligram equivalents
Changes in Mirogabalin and Pregabalin doses from baseline to the occurrence of Somnolence and DizzinessDose changes of mirogabalin and pregabalin after the initiation of opioid co-administration might also influence the occurrence of somnolence and dizziness. Thus, we investigated the changes in mirogabalin and pregabalin dosage from baseline to the occurrence of somnolence and dizziness. In the mirogabalin group, 87.5% of the patients had no change in dosage from baseline to the occurrence of somnolence and dizziness. In the pregabalin group, while 68.4% of the patients had no change in dosage from baseline to the occurrence of somnolence and dizziness, 31.6% received increased doses (Table 3).
Table 3 Number of patients with changes in mirogabalin and pregabalin dosage from baseline to the time of somnolence and dizziness occurrencesSubgroup analysis for differences in the occurrence of Somnolence and Dizziness between Mirogabalin and PregabalinTo eliminate the potential influence of somnolence and dizziness occurring immediately after opioid initiation, the exacerbation of pre-existing somnolence and dizziness, and the effects of transdermal formulations (e.g., fentanyl), we conducted subgroup analyses limited to (1) patients who had been using opioids for at least one week prior to baseline (2), patients who did not exhibit somnolence or dizziness at baseline, and (3) patients who were using oral opioid formulations at baseline (Additional files 2–7). While the results should be interpreted with caution given that these are subgroup analyses, trends similar to those in the overall population were observed across all subgroups.
Comments (0)