This exercise highlights the critical role of the redistribution method, emphasizing its interdependence with ICD coding practices and the definitions of IDD codes.
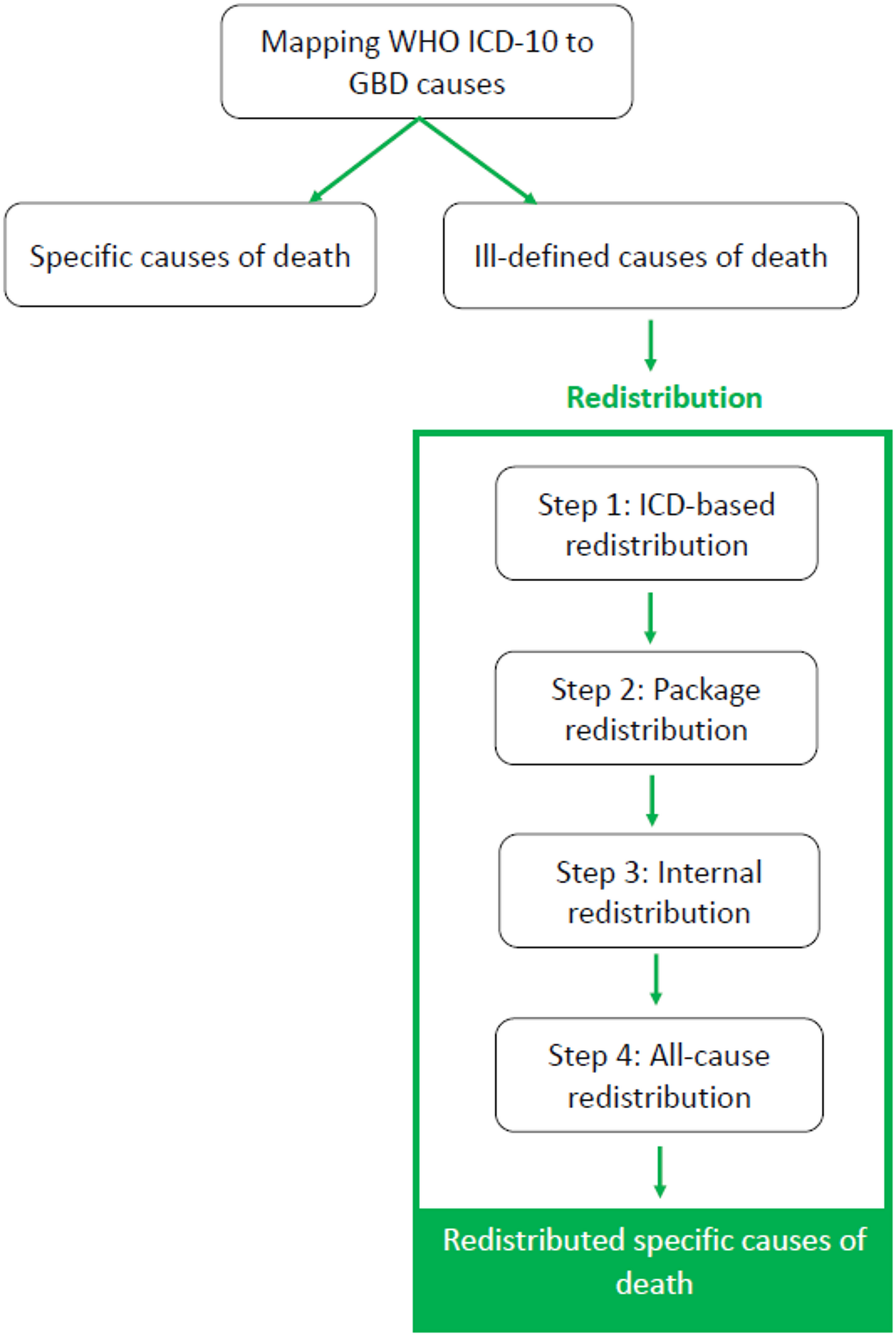
Redistribution method
This redistribution method is transparent and can be replicated and adopted to apply to other national contexts, depending on the available mortality data. This approach allows using all available data on multiple causes of death, to redistribute IDDs by 6 age groups and sex and validated by burden of disease experts [9]. By applying a probabilistic redistribution approach, the resulting uncertainty intervals were relatively narrow, indicating higher precision in the estimates. After redistribution of IDDs, we observed a few major shifts in leading causes of death among three countries: Belgium: Lower respiratory infection ranked 28th (before redistribution) to 5th position (after redistribution), and stroke ranked 6th (before redistribution) to 3rd position (after redistribution). France: Lower respiratory infection ranked 22nd (before redistribution) to 6th position (after redistribution), and other cardiovascular and circulatory diseases ranked 26nd (before redistribution) to 8th position (after redistribution). Slovenia: Lower respiratory infections ranked 31st (before redistribution) to 4th position (after redistribution), atrial fibrillation and flutter ranked lower than 50th (before redistribution) to 27th position (after redistribution) and cardiomyopathy and myocarditis ranked 43rd (before redistribution) to 36th position (after redistribution). These shifts could be due to narrow definitions of IDDs.
This approach allows us to understand the in-depth knowledge of various steps applied to the redistribution process in a clear and transparent way. These steps ensured that the IDDs were accurately redistributed to specific causes of death and that the targets were updated at the end of each step, which decreases the chance of over- or under-represented causes of death in the final ranking [9].
ICD-coding practices
The ICD (International Classification of Diseases) coding practices can significantly vary from country to country. For example, variations in interpretation of causes of death, updates/revisions in ICD versions, which may add or reclassified into more specific categories, some coding systems may choose more specific codes while others might use a broader category, some coding systems may emphasize on contributing cause while others may focus on the underlying cause of death, presence of a centralized coding system for underlying causes of death (i.e., Slovenia, with a low proportion of IDD). Overall, all these factors should be considered in the context of the identification of IDDs, which may result in differences in the ranking of leading causes of death between regions, countries, and over time, even when mortality rates are similar.
Definition of IDD
The criteria used to define what constitutes an ill-defined death is important and it can vary between countries or regions, affecting the number of deaths categorized under IDD. At present, only GBD updates the list of IDDs at the cycle of each GBD study. The definition of IDD could have a narrow or broad definition. A narrow definition may result in fewer deaths being classified as IDD, leaving more deaths under specific causes of death and creating the appearance of more accuracy to mortality statistics. Nevertheless, a narrow definition may underreport issues by partially excluding specific death that lack clarity such as cardiac arrest with no underlying cause. Conversely, a broad definition might increase the number of IDDs and could highlight the full extent of poor reporting that requires more extensive redistribution, which may risk losing important information in the national context. Using broad definitions can dilute specificity by grouping together certain deaths that are unclear and may inflate the proportions of unclear deaths. The differences in how IDDs are defined, thus, redistributed to specific causes of death (i.e., target codes), can lead to significant variations in the rankings of final causes of death (after redistribution), which can affect trend analyses and health policy decisions.
This commentary has some limitations: first, we did not explore the existing differences in IDDs among the three countries, which might be due to different coding practices/systems. Further research is needed to explore that. Second, we did not compare results of this model with other models or independent datasets, to explore the impact of redistribution methods. More research is needed to compare different models used for redistribution of IDDs by using a single dataset. Moreover, a scoping review is needed to compare all the available redistribution methods, highlight the strengths and limitations of each model.
Policy recommendations
We propose a task force under the supervision of the European Commission/Eurostat could be established, to develop a common/standardized consensus list of IDDs, aligned with the mortality databases in European countries. This task force should include representatives from national statistical offices, mortality data experts and public health institutes from European countries. This task force should agree on a comprehensive definition of IDDs, harmonized list of IDDs validated by the task force, integration of the standardized list into the national mortality database and reporting systems, and to review this list periodically to update the changes. This approach would support comparability, transparency, and data quality in European mortality statistics, especially important for cross-country analysis, burden of disease studies, and health policy planning. This work has important implications to future BoD analyses at national level in terms of transparency of redistribution approach, in-depth understanding of local mortality data set, highlight data gaps and to improve further the quality of data reporting.






Comments (0)