In this study, we explored the characteristics, biomarkers, treatments, and progression of patients diagnosed with NSCLC and explored various elements affecting therapy determination for advanced stages and metastatic non-small cell lung cancer in Palestine.
In this study, it is evident that the number of males (80.4%) diagnosed with NSCLC was much higher than that of females, which is very similar to the findings of a study in Palestine and in other regional countries in Africa and the Middle East KINDLE study, where more than 80% of patients diagnosed with NSCLC were males and approximately 50% had adenocarcinoma [10, 11]. Many factors increase the risk of lung cancer among Palestinian males. Smoking has been reported to be more prevalent in males in Palestine owing to socioeconomic and cultural factors. It has been reported that the rate of smoking exceeds 36% among adults in Palestine [11]. A multicenter study on the prevalence of tobacco use in Palestine revealed that tobacco smoking was higher among males than females by a factor of 2 [12]. This finding was supported by the results of several previous studies. The higher incidence of lung cancer in males is due to their excessive smoking history, and smokers have a higher risk of developing lung cancer in their lifetime [13].
Furthermore, a systematic review and meta-analysis revealed that smoking cessation at or around the time of diagnosis was significantly associated with improved overall survival in patients with NSCLC, SCLC, or lung cancer [14]. Adenocarcinoma has been reported as the most prevalent histological subtype of lung cancer, which was evident in this study, as the most common histological subtype in the study was adenocarcinoma (86.3% of the participants had lung adenocarcinoma). Studies of NSCLC conducted in Jordan, Lebanon, and the USA have reported that adenocarcinoma is the most common type of NSCLC [15,16,17].
Programmed cell death protein 1 (PD-1) and programmed cell death ligands are among the most important biomarkers in treatment decision-making. PD-1/PDL-1 inhibitors, such as nivolumab and pembrolizumab, achieve their therapeutic effect by preventing the antigen binding of PD-1 and PDL-1, allowing T cells to attack and destroy tumor cells [18]. In this study, 56.9% of the patients had PDL-1 expression, which is very similar to a recent study conducted in Lebanon, which revealed a PDL expression of 61.7% [17]. In this study, patients with PDL expression who received immunotherapy as monotherapy or in combination therapy had a better overall response than patients with low or no PDL-1 expression. In the present study, we observed that a higher efficacy response when immunotherapy was used in the presence of high PDL-1 expression was very evident in this study [19]. This finding is supported by a systematic review showing that PD-1/PD-L1 inhibitors are effective and promising immunotherapeutic agents for the treatment of many types of cancer [20]. Meanwhile, 11.8% of patients in the study had (PDL-1 expression < 1%), whereas 33.3% of them received immunotherapy regardless of the absence of PDL-1 expression due to a lack of other options, the patient’s performance status, inability to tolerate chemotherapy side effects, or the main aim of treatment being remission and not cure [21, 22]. In addition to PD-1/PDL-1 expression, EGFR mutations are known to become a part of the treatment modalities for patients with NSCLC. The EGFR mutation was found to be the most abundant genetic mutation type (45.1%), with exon 21 L858R being the most common EGFR subtype (24.5%). In a systematic review and meta-analysis of EGFR mutation frequency in Middle East and African non-small cell lung cancer patients, EGFR mutation exon 19 was the most prevalent type [23]. A clinical report performed in Jordan on patients with adenocarcinoma NSCLC showed that the prevalence of EGFR mutations is higher among Asian patients than among Jordanians and lower among African Americans [19]. The prevalence of EGFR mutations in this study was much higher than that in regional countries, such as Lebanon (12%), Morocco (21%), Egypt (27%), and the Gulf area (more than 30% in the Gulf area [24]. Combination therapy has been utilized in more than 50% of patients with EGFR mutations and is recommended to improve overall outcomes [25].
Tumor nodes affect treatment selection. In advanced stages, the treatment goal is to improve patients’ quality of life and overall survival. In this study, 22.5% of the participants had stage III NSCLC, and 77.5% had stage IV NSCLC. Most patients with advanced-stage disease were treated with combination therapy. In total, 56.1% of patients with stage IVA and 42.1% of patients with stage IVB received combination therapy, and the use of immunotherapy with chemotherapy improved the overall survival for advanced and metastatic stages of NSCLC [26].
Pharmacotherapy treatment modalities
Patient performance status, or Eastern Cooperative Oncology Group (ECOG) performance status, is an important variable used in selecting treatment modalities to determine treatment and for optimum results, considering the patient’s tolerability and physical status. In this study, 46.2% of patients with an ECOG score of 0 received monotherapy, patients with ECOG 1 (76.7%) and ECOG 2 (72.4%) received combination therapy, and the majority of patients with poor performance status (ECOG ≥ 3) (80.0%) received monotherapy (Table 1). These findings are supported by the Clinical Oncology Guidelines for managing NSCLC in patients with an ECOG performance status ≥ 3. Chemotherapy can result in lower response rates and higher toxicity. These findings were supported by the ASCO clinical guidelines for the management of NSCLC in patients with an ECOG score ≥ 3 to use immunotherapy alone. The use of chemotherapy in patients with ECOG ≥ 3 can result in lower response rates and high toxicity [27], as found in our study; only one patient with ECOG ≥ 3 used chemotherapy alone, whereas other studies suggest that immunotherapy improves the quality of life and benefits the patient’s survival rate [28]. ECOG performance status can decline or improve in patients during the treatment period, explaining why patients with poor performance status receive chemotherapy or combination therapy.
Patients with early-stage resectable NSCLC can be treated or cured surgically by removing the affected tissue from their lungs [29]. In terms of late diagnosis at advanced or metastatic stages, surgical intervention for complete tumor resection is not recommended. However, surgery can reduce the tumor burden at the sites of metastasis [30]. Of the patients, 77.5% underwent surgery with the aim of tumor removal, and 22.5% had no surgery because of extended metastasis of the disease. Although surgery is a reliable option for early-stage cancer, some patients develop tumor recurrence mainly due to micrometastatic cancer cells [31]. In this study, 47.1% of the patients who underwent surgery experienced tumor recurrence. After recurrence, the tumor was most likely more aggressive and spread to other regions, requiring the addition of immunotherapy and targeted therapy to traditional chemotherapy, according to the National Cancer Institute (NCI) guidelines [32].
Many treatment options for lung cancer, including chemotherapy, are used if the patient can tolerate side effects, such as immunotherapy, which is used in the presence of PDL-1 expression. According to the American Cancer Society, targeted therapy and immunotherapy are the first-line agents for patients diagnosed with stage IVB NSCLC. According to the ASCO of Clinical Oncology, stages IIIB and C are treated using platinum-based doublet chemotherapy, an EGFR inhibitor, and a PDL-1 inhibitor (if EGFR mutations and PDL-1 expression are present). For stages IVA and B, first-line treatment includes chemotherapy with a PDL-1 inhibitor [33]. The combination of chemotherapy and immunotherapy has a synergistic effect, emphasizing its antitumor activity [34]. In Palestine, there is limited access to newer medications, and not all immunotherapy and targeted therapy, such as nivolumab, pertuzumab, and pembrolizumab, are available to patients [11]. Patients with EGFR mutations who are not treated with EGFR-TKI inhibitors, such as erlotinib or gefitinib, are considered first-line agents in these patients owing to their increased survival rates; however, these medications are not available [35]. In this study, only 4.9% of the patients received a combination of platinum-based chemotherapy with taxane, 24.5% of the patients received pembrolizumab, and 7.8% received a combination of taxane and folate antagonist chemotherapy with pembrolizumab immunotherapy. The limitations of cancer treatment options, diagnosis, and screening negatively impact patient outcomes. As shown in this study, the majority of patients were diagnosed in the later stages of cancer, making treatment options very challenging and resulting in a low survival rate. In Palestine, there is a lack of effective programs focusing on screening and controlling risk factors for cancer prevention. Furthermore, the limitations of pathological tools for treatment and diagnosis have caused many cancer patients to be referred to or seek treatment outside the territory, limiting access to care in conflict zones where movement is restricted and requires a permit that is often denied by the occupation authority [36].
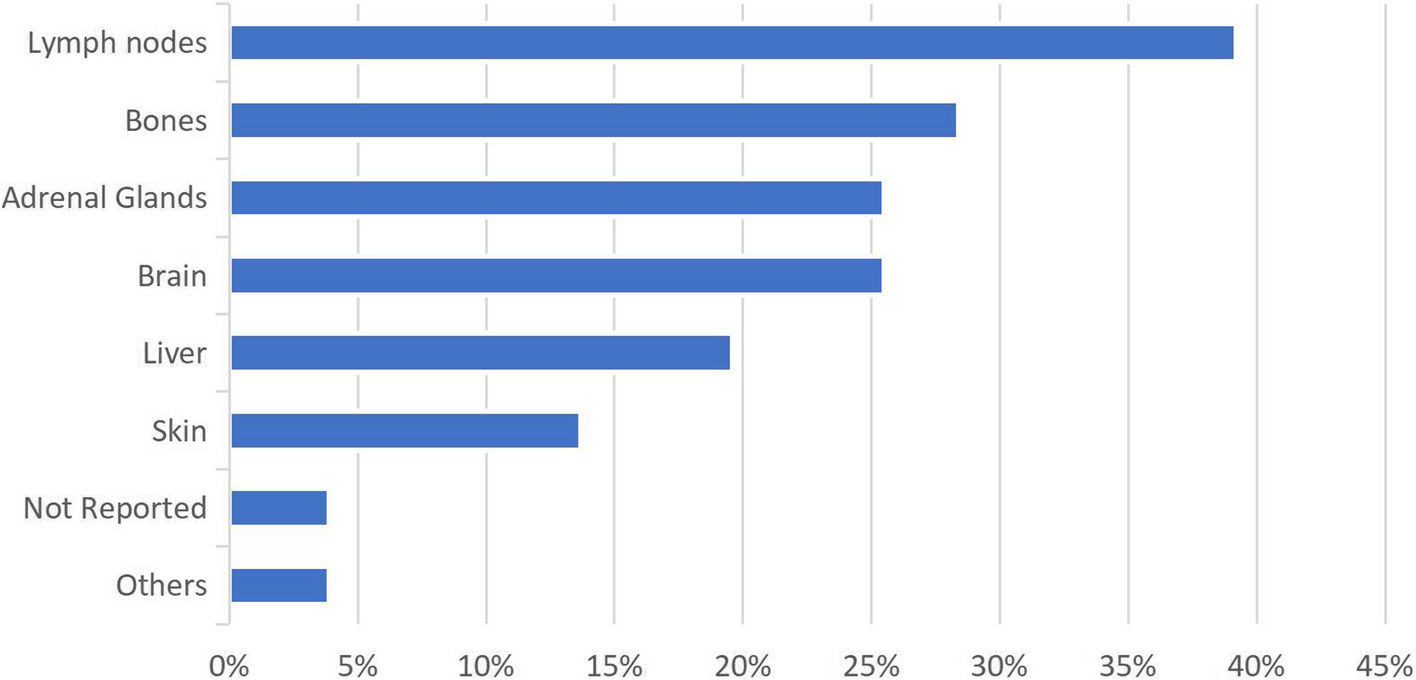
Site of metastasis
The most common sites of metastasis in NSCLC include the bone, brain, and abdominal regions (liver, adrenal glands, kidneys, and gastrointestinal tract) and lymph node involvement [37]. Data analysis revealed that 28.4% of the patients had bone metastasis, 25.5% had brain metastasis, 25.5% had adrenal gland metastasis, and 39.2% had lymph node metastasis. Studies have suggested that bone metastasis reduces the efficacy of immunotherapy when used alone, thus recommending combination therapy [37]. In this study, 48.3% of the patients with bone metastasis received a combination of immunotherapy and chemotherapy, and 41.4% received monotherapy. Studies have suggested that bone metastasis reduces the efficacy of immunotherapy when used alone [38], suggesting the use of combination therapy, as hypothesized by a Lebanese study [39].
Patient prognosis
The efficacy of the selected treatment was determined by monitoring the tumor response 3 months after initiating treatment [40]. Complete response is very rare in metastatic lung cancer cases, considering the possibility of multiple site metastasis and late diagnosis [41], and as seen in the results, 0% of patients had no complete response. Most patients showed a partial and stable response, especially those receiving combination therapy (52.8% and 61.8%, respectively), indicating the extent of the therapy in tumor regression and stabilization of the disease from further growth, better outcomes, and fewer side effects [42]. Among patients with disease progression, 41.9% received combination therapy, and 38.7% received immunotherapy. The data analysis suggested that combination therapy has higher efficacy in tumor regression and disease stabilization than other therapies such as chemotherapy and immunotherapy monotherapy.
Progression-free survival is one of the main indicators of treatment efficacy and patient response to treatment. Thus, comparing the PFS associated with multiple treatments can yield promising outcomes, leading to the preferred treatment [43]. The data analysis of this study showed that patients receiving combination therapy as the main treatment (58.3%) had a higher PFS (> 1) than those receiving chemotherapy as monotherapy (19.7%), who had a lower PFS (≤ 1). The findings of improved PFS in patients receiving combination therapy are supported by clinical trials in Spain [44].
Overall survival
Overall survival (OS) is one of the most important outcomes of treatment. Figure 3 shows that patients who received a combination of chemotherapy and immunotherapy had an estimated mean survival of 2006.777 days, while patients who received mono-chemotherapy and mono-immunotherapy survived with a mean of 1219.200 and 720.152 days, respectively. This analysis revealed that the combination regimen had the most prolonged overall survival, followed by mono-chemotherapy and mono-immunotherapy. These results are confirmed by many previous studies, which state that using chemotherapy and immunotherapy combinations provides better outcomes and responses and improves survival in patients with NSCLC compared to monotherapy [45], regardless of PDL1 expression [42, 43, 46]. In a five-year follow-up of immunotherapy versus chemotherapy in metastatic NSCLC, pembrolizumab showed a median OS of 26.3 months vs 13.4 months in the chemotherapy group. Furthermore, the immunotherapy group experienced fewer adverse events [47].
Side effects
Nausea, vomiting, alopecia, fatigue, myelosuppression, and nephrotoxicity are the common side effects of chemotherapy [48]. Abdelazeem et al. [45] The side effects of immunotherapy include infusion reactions, rash, arthritis, muscle or joint aches, diarrhea, and fatigue [49]. The results of the present study show that nausea and vomiting were experienced by 50.0% of patients who received mono-chemotherapy compared to 35.30% of patients who received mono-immunotherapy. Nausea and vomiting are the side effects most likely caused by chemotherapy, and immunotherapy can also cause nausea and vomiting in patients, specifically nivolumab, as stated in other studies [50]. Alopecia was reported in 49.20% of patients receiving chemotherapy and 5.90% of patients receiving immunotherapy, indicating that alopecia is mainly associated with chemotherapy. Other studies suggested that alopecia may occur in patients receiving immunotherapy [51]. Infusion reactions are immunotherapy-mediated side effects that have been reported in several other studies [52]. Leana [49] In this study, 29.60% of patients receiving immunotherapy experienced an infusion reaction compared with 0% of those who received chemotherapy. Myelosuppression and hepatotoxicity were the other side effects that patients complained of regarding chemotherapy in this study, and the most common side effects and toxicities of chemotherapy were nausea, vomiting, alopecia, fatigue, myelosuppression, and nephrotoxicity [48]. However, regarding other side effects, immunotherapy patients complained of rash, which was the most common immune-mediated side effect, supported by studies that suggested that the side effects of immunotherapy include infusion reactions, rash, arthritis, muscle or joint aches, diarrhea, and fatigue [49]. When both agents are combined, there is a risk and severity of side effects, and toxicity increases [53], such as hematotoxicity, hepatotoxicity, and GI abnormalities [46].
Limitations
The main limitation of this study is its small sample size of 102 patients, which limits the generalization of the study to treatment groups; however, it sets the groundwork for future large-scale studies with larger sample sizes. Furthermore, sampling coverage bias may have occurred since the study only involved two hospitals, excluding patients with limited access to healthcare and those who transferred to be treated outside the country, further limiting the representation of patients with NSCLC. Hospital documentation lacks long-term follow-up and survival data, which could have affected the results. Another limitation is inadequate genetic testing or a lack of genetic data, as not all patients were tested for PDL-1 expression and other genetic mutations affecting treatment selection and outcomes.

Comments (0)