Study area
The study area, Hua County, is located in Henan Province in northern China. In 2012, the county had a permanent resident population of 1.24 million, which declined to 1.15 million in 2023. In 2023, the county’s per capita Gross Domestic Product was 22,265.9 Chinese Yuan (US $3,063.79) [13]. Hua County was devastated by the “Chinese Great Famine” in 1959–1961. Official population data indicated that the mortality in Hua County reached 39.6‰ in 1960, doubling the average level from 1956 to 1958 [12, 14]. The county has a stable population (annual variation rate < 1%) and low mobility (out-migration rate < 5% between 2012 and 2023), making it an ideal location for long-term follow-up studies. Furthermore, 90% of the residents are engaged in agriculture in Hua County, making it a representative area for studying the impact of famine. Therefore, this study defines Hua County as a primary famine-affected area and considers its population as the study cohort.
Study subjects
Study subjects in whole population analysis. In this study, we retrospectively extracted the registry information, including personal ID, sex, date of birth and residence (detailed to the level of village), of local residents from the New Rural Co-operative Medical Scheme (NRCMS) in 2012 in Hua County, which is the sole government-run health insurance system for rural residents in China, achieving a coverage of > 95% in the study area at 2012 [15]. The records extracted from the NRCMS were then linked with the death registry data of Hua County.
The individuals meeting the following inclusion criteria were included: (1) being born within the period from 1 January 1959 to 31 December 1964; (2) having complete personal ID and sex information; and (3) being alive as of 1 January 2012 according to the local death registry. A total of 1,234,851 individuals were initially included in the whole population analysis. As shown in the flow diagram (see Supporting Material), 1,169,593 individuals born outside the period from 1 January 1959 to 31 December 1964 were excluded, leaving 65,258 individuals eligible based on the inclusion criteria. Among these, 122 individuals were further excluded due to missing or incorrect information, including 31 with invalid personal IDs and 91 with errors in names, villages, or sex. This resulted in 65,136 individuals with complete personal ID and sex information. Additionally, 124 individuals with recorded death dates prior to cohort enrollment on 1 January 2012 were excluded, leaving a final cohort of 65,012 participants.
Study subjects in individual-level analysis of population-based cohorts. In order to better control the potential confounding effects of age at enrollment and other risk factors on the association between the famine exposure and adulthood NCD outcomes, individualized data from two representative population-based cohorts in Hua County were used, namely the Endoscopic Screening for Esophageal Cancer in China (ESECC) trial [16,1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18] and Anyang Esophageal Cancer Cohort Study (AECCS) [19] conducted by our research team. Both studies were designed as community-based screening cohorts for upper gastrointestinal cancers and collected individual-level information using questionnaire survey by trained researchers according to a standard operation procedure, enabling adjustment for individual-level confounders (see supplementary methods for details). Both the ESECC and AECCS cohorts collected participants’ personal ID, which function as the unique identifiers in the NRCMS system. This allowed us to accurately link individual-level covariates with NRCMS reimbursement records and death registry data. The inclusion criteria for participants in the population-based cohorts are identical to those for the whole population analysis.
Exposure definition
Early-life undernutrition exposure was defined based on participants’ date of birth. Individuals born between 1 January 1959 and 31 December 1961, i.e., who were under the age of three during the 1959–1961 Chinese Great Famine, were classified as having been exposed to early-life undernutrition. The unexposed participants were those born between 1 January 1962 and 31 December 1964.
Outcomes ascertainment and follow-up
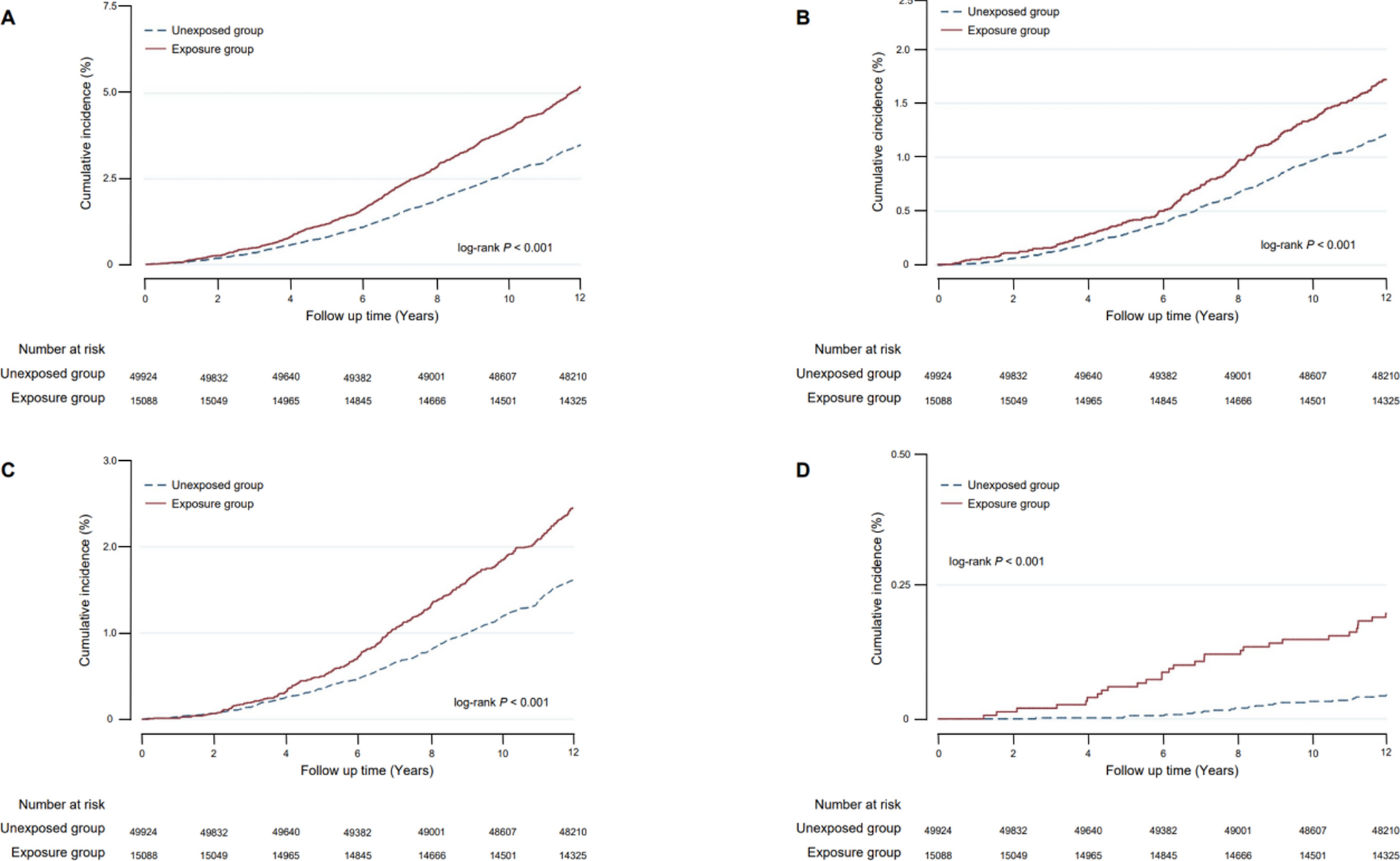
The primary outcomes of this study include all-cause mortality, cancer mortality, cardiovascular and cerebrovascular diseases mortality, and chronic obstructive pulmonary disease mortality during the follow-up period. Secondary outcomes involve mortality from lung cancer, esophageal cancer, gastric cancer, colorectal cancer, hepato-biliary cancer, pancreatic cancer, cardiovascular disease, and cerebrovascular disease separately.
Death events were ascertained using the death registry data from the Centers for Disease Control and Prevention (CDC) in Hua County. The registry records, after de-identification, include the date of death, the primary cause of death (coded according to the ICD-10), and basic personal information (e.g., personal ID, sex, date of birth, and residence). Linkage between the death registry, the NRCMS, and the individual-level databases of the ESECC and AECCS cohorts was performed using the encrypted personal ID as the primary matching variable. For records lacking a valid personal ID, we employed a fuzzy matching algorithm based on name, sex, date of birth, and residence (town and village) to identify death events. Any discrepancies were manually verified through double data entry and logical consistency checks, ensuring the accuracy of the linkage [20].
For the whole population analysis, the start of follow-up was set at 1 January 2012. For the individualized analysis of population-based cohorts, follow-up for ESECC started from the actual date of entry into the cohort for each individual, which occurred during 2012–2016; for the AECCS, although the cohort enrollment occurred during 2006–2009, to ensure a follow-up duration and baseline risk of death comparable with those of ESECC, the start of follow-up for this study was set to 1 January 2012. The end date of follow-up was set at 31 December 2023 for all analyses. Time at risk was calculated from the enrollment date until the end of follow-up or the date of death, whichever occurred first.
This study maintained a high quality of follow-up using linkage with the NRCMS database and the death registry from Hua County CDC. No loss to follow-up was observed during the study period due to the comprehensive coverage and robust data linkage mechanisms.
Statistical analysis
Whole population analysis. Sex distribution was compared between exposed and unexposed cohorts using the Chi-square test, and age and follow-up duration compared using Wilcoxon rank sum test. Survival curves for both exposed and unexposed cohorts were estimated using Kaplan–Meier method and compared using log-rank test. Associations between early-life undernutrition and all-cause mortality were evaluated using multivariable Cox proportional hazards model adjusted for sex. For all the other outcome events, competing risk regression models were employed treating causes of death other than the cause of interest as competing events. The competing risk model can estimate the cumulative incidence rate and hazard ratio of the target event more accurately by taking into account the influence of competing events.
Individualized analysis of population-based cohorts
Individualized analysis of population-based cohorts. Based on individual-level questionnaire data from two population-based cohorts conducted in Hua County, we further constructed three multivariable Cox models for all-cause mortality and three competing risk models for cause-specific mortality (labelled as Models 0, 1, 2, and 3) that adjusted for well-established determinants of death. For each outcome, Model 0 adjusted for sex; Model 1 adjusted for age at enrollment, sex, education (illiterate, primary school, junior high school, or high school and above), occupation (non-laborer or laborer), and marital status (married or others); Model 2 further included cigarette smoking (yes, no) and alcohol drinking (yes, no); and Model 3 further adjusted for body mass index (BMI; < 18.5 kg/m2, 18.5–24.9 kg/m2, 25.0–29.9 kg/m2, or ≥ 30 kg/m2), and additionally incorporated cancer family history for cancer mortality.
All statistical analyses were performed using STATA (Version 15.0; Stata Corp LLC, TX, USA). All tests were two-tailed, and P values < 0.05 were considered statistically significant.
Patient and public involvement statement
Patients and the public participated in individualized data collection for the Endoscopic Screening for Esophageal Cancer in China (ESECC) trial and the Anyang Esophageal Cancer Cohort Study (AECCS). They provided demographic, lifestyle, and health information through questionnaires and interviews. Research questions and survey tools were refined based on input from participants and community health workers. Participation burden was minimized through informed consent and consultation with local healthcare providers.
Findings will be shared with the community via health education programs, public health recommendations, and local events.


Comments (0)